
Abstract
Purpose
Vulnerability to stress is linked to poor mental health. Stress management interventions for people with mental health conditions are numerous but they are difficult to implement and have limited effectiveness in this population. Virtual reality (VR) relaxation is an innovative intervention that aims to reduce stress. This review aimed to synthesize evidence of VR relaxation for people with mental health conditions (PROSPERO 269405).
Methods
Embase, Medline, PsycInfo, and Web of Science were searched until 17th September 2021. The review was carried out according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses. The Effective Public Health Practice Project (EPHPP) tool assessed methodological quality of studies.
Results
Searching identified 4550 studies. Eighteen studies (N = 848) were included in the review. Studies were published between 2008 and 2021. Eleven were conducted in Europe. Thirteen studies were controlled trials. Participants were mostly working-age adult outpatients experiencing anxiety or stress-related conditions. Other conditions included eating disorders, depression, bipolar disorder, and psychosis. Five studies tested inpatients. All studies used a range of nature-based virtual environments, such as forests, islands, mountains, lakes, waterfalls, and most commonly, beaches to promote relaxation. Studies provided evidence of the feasibility, acceptability, and short-term effectiveness of VR relaxation to increase relaxation and reduce stress. EPHPP ratings were ‘strong’ (N = 11), ‘moderate’ (N = 4), and ‘weak’ (N = 3).
Conclusions
VR relaxation has potential as a low-intensity intervention to promote relaxation and reduce stress for adults with mental health conditions, especially anxiety and stress-related problems. Further research is warranted on this promising intervention.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Vulnerability to stress is linked to mental health conditions, such as depression and anxiety, and has been exacerbated by the COVID-19 pandemic [1, 2]. Having a mental health condition can in turn increase stress levels, consequently creating a vicious bidirectional relationship in which stress maintains and worsens mental health symptoms [3], which can be a trigger for more severe and prolonged problems [4, 5]. Numerous stress management interventions aim to reduce stress and improve well-being [6]. Stress management techniques such as meditation, yoga, and progressive muscle relaxation can improve mental health outcomes by promoting relaxation, reducing tension, and activating the parasympathetic nervous system [7], which reduces stress-associated physiological responses, such as elevated blood pressure and heart rate [6]; while mindfulness-based interventions can improve short-term cognitive outcomes and emotion regulation [8]. Stress management relaxation techniques are widely considered to be cost-effective and low risk [9]; however, they can be difficult to implement due to time constraints, stigma about help-seeking, lack of consumer confidence, and needing high levels of consumer effort in terms of concentration and attention, which can often be impaired in people with mental health conditions [10].
Innovative approaches are therefore needed to supplement existing stress management techniques, particularly for people with mental health conditions. Virtual reality (VR) relaxation is one such innovation that is attempting to meet this need. VR is an immersive technology that is increasingly being used in various healthcare settings [11], including for people with mental health conditions [12,13,14]. Research indicates that VR-based relaxation, using head mounted displays (HMD) to deliver the VR, is feasible, acceptable, and is effective in the short-term to promote relaxation and reduce stress for the general, non-clinical population [15]. However, despite the emergence of promising studies that test VR relaxation in clinical samples, there is no systematic review of VR relaxation for people with mental health conditions. Therefore, the aim of this systematic review is to identify, narratively synthesize, and quality rate existing research on VR relaxation for people with mental health conditions (PROSPERO: 269405).
Methods
Search strategy
This review was carried out according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [16]. Academic databases Embase, Medline, PsycInfo and Web of Science were searched until 17th September 2021. Search terms were: “virtual real*” OR “virtual-real*” OR “VR” OR “virtual enviro*” OR “virtual character*” OR “VCs” OR “avatar*” AND “relax*” OR “autogen*” OR “meditat*” OR “mindful*” OR “rest*” OR “PMR” OR “progressive muscle” OR “imagery” OR “breath*” OR “distract*” OR “wellness” OR “wellbeing” OR “well-being” AND “mental health” OR “mental illness” OR “mental disorder” OR “psych*" OR "schiz*" OR "mood" OR “depress*” OR “bipolar” OR “anxi*” OR “panic disorder” OR “obsessive compulsive” OR “obsessive–compulsive” OR “OCD” OR “stress” OR “PTSD” OR “dissociat*” OR “eating” OR “anorexi*” OR “bulim*” OR “substance us*” OR “substance misuse” OR “addict*” OR “dissocial” OR “personality disorder”. Truncations were used to account for alternative spellings and word endings. Search terms associated with VR and relaxation were adapted from a previous systematic review on VR relaxation for the general population [15]. Search terms associated with mental health conditions were adapted from diagnostic labels in the International Statistical Classification of Diseases and Related Health Problems, (11th ed; ICD-11; World Health Organization [17]. Studies categorized under key subject headings (‘Virtual Reality’, ‘Relaxation’, and ‘Mental Disorders’) were extracted using the ‘explode’ function on Embase, Medline and PsycInfo. These studies, and those from other sources, such as reference lists of review articles, were pooled with those identified using search terms. Studies were extracted and screened using reference management software Endnote. All stages of the search strategy and data extraction were carried out by two independent researchers (PJ, LT), under the supervision of the lead author (SR). There was regular checking and consultation on this process between the research team to ensure that relevant articles were not overlooked.
Studies were included in the review if they were published in a peer-reviewed journal; written in English; used quantitative research methods of any study design; had a sample size of N ≥ 5; tested clinical populations with either a formal mental health diagnosis from manuals such as ICD or DSM or, more informally, reported symptoms that could be interpreted as consistent with recognized mental health conditions; tested a virtual reality-based relaxation intervention; and measured relaxation or relaxation-related variables. Studies were excluded if they were abstracts, conference proceedings, dissertations, non-empirical, reviews, used only qualitative methods, or targeted specific, non-clinical anxieties, for example, dental anxiety or exam anxiety. The review used a narrative approach to synthesize findings. Findings were analyzed in terms of feasibility (i.e., safety, accessibility), acceptability (i.e., user experience, lack of adverse effects), and effectiveness (i.e., outcomes, impact on mental health symptoms). In the event of any discrepancies or disagreement between researchers on the search strategy and data extraction, studies were discussed between the research team (SR, PJ, LT) until discrepancies were resolved.
Quality assessment
Quality rating was carried out by four independent reviewers (PJ, LT, CF, JL), under the supervision of the lead author (SR), using the Effective Public Health Practice Project (EPHPP) tool. EPHPP has good content and construct validity, and inter-rater reliability [18], and can provide consistent quality ratings for a range of study designs. EPHPP’s six subscales (selection bias, study design, confounders, blinding, data collection methods, and withdrawals and drop-outs) are given a rating of ‘strong’, ‘moderate’, or ‘weak’. A global rating for each study is calculated. Studies receive a global rating of ‘strong’ if there are no weak subscale ratings, ‘moderate’ if there is one weak subscale rating, and ‘weak’ if there are two or more weak subscale ratings. EPHPP reclassifies randomized controlled trials (RCTs) as controlled clinical trials (CCTs) if studies do not report information on method of randomization. Discrepancies in ratings were discussed between researchers (SR, PJ, LT, CF, JL) and studies were re-evaluated until consensus was reached.
Results
Study characteristics
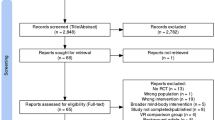
A total of 4,550 studies were identified through database searching and an additional four studies were identified from other sources. From this total, 26 full papers were screened, and of these, eighteen studies, published between 2008 and 2021, met inclusion criteria and were included in the review. See Fig. 1 for the PRISMA diagram. See Table 1 for full details of study characteristics. Most of the eighteen studies were from European research groups (N = 11); specifically, studies were conducted in Italy (N = 6), The Netherlands (N = 3), Singapore (N = 2), Australia (N = 1), Canada (N = 1), France (N = 1), South Korea (N = 1), Taiwan (N = 1), United Kingdom (N = 1), and United States of America (N = 1). In total, 848 participants took part in the studies. Almost all studies tested working-age adult participants, who were mostly female. There were four RCTs and nine CCTs. Study samples ranged from eight to 175 participants; seven studies had samples of over 50 participants; and two studies used the same sample due to the participants being followed up three months after the initial study [19, 20]. Thirteen VR interventions had interactive components for participants to engage with and five were passively viewed by participants. Sixteen interventions were facilitator-led, one was self-led by participants in their homes, and in one case, this aspect of the intervention was unclear.

Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram of studies investigating virtual reality relaxation for people with mental health conditions
Fifteen studies tested samples of participants with one specific mental health condition. Six studies tested people with Generalized Anxiety Disorder [21,22,23,24,25,26]. Three studies tested people experiencing stress, such as posttraumatic stress [27], high stress [28], and stress-related problems [29]. Three studies tested people who experienced emotional eating in the context of obesity [19, 20], including with high anxiety [30]. Two studies tested people with depression, including Major Depressive Disorder and Bipolar Disorder with a depressive episode [31], and in the context of suicidality [32]. One study tested people with psychosis [33]. Three studies tested mixed samples of participants with a range of different diagnoses. One study tested participants with mental health conditions such as anxiety, bipolar disorder, depressive, and psychotic disorders, where 30% had an anxiety-related disorder [34]; another study tested mostly male adolescent participants with attention deficit hyperactivity disorder (ADHD) or autism spectrum disorder (ASD), accompanied with anxiety and behavioral problems [35]; and another tested participants with depression, bipolar disorder, or schizophrenia [36]. Thirteen studies tested outpatient service users and five studies tested inpatient service users on psychiatric wards, including one study that took place in a psychiatric intensive care unit with a male sample [33]. Most studies on outpatient participants were conducted in labs, apart from the study on adolescents with ADHD or ASD, which was conducted in a specialist school [35] and another which involved participants of various diagnoses accessing content remotely using an HMD at home [34].
Studies varied considerably in number of VR relaxation sessions offered. One study used 20 sessions of VR relaxation, two studies used 12, three studies used eight, two studies used six, two studies used three, three studies used two, and five studies used one. All studies used a range of nature-related scenes, such as forests, islands, mountains, lakes, waterfalls, and most commonly, beaches. One study involved cycling through virtual forests and parks while seated on a real-world static bike [26]; but all other studies involved participants in a stationary position, generally seated, wearing an HMD, often with relaxing narratives or audio. Six studies involved participants using biofeedback to control in-game play, on a tropical island, a trekking path, or underwater, in order for users to change features of the virtual environment, such as the movement of a waterfall or the waves of the sea, or the intensity of a campfire on a beach [22,23,24, 28, 29, 35]. In these biofeedback-assisted studies, biofeedback data, such as a participant’s heart rate, could be used to reduce the intensity of the virtual campfire until it disappeared or could make the virtual sea calmer. Some studies used stressful virtual environments or exercises, such walking on a virtual shaky path, words or images related to stressful events, or a mathematical task, against which to compare virtual relaxation environments [22, 28]. Seven studies incorporated standard, non-virtual relaxation techniques, such as progressive muscle relaxation [21] and guided meditation using an audio track [34], in combination with the VR relaxation. One study reported follow-up sessions, which occurred three months after patients were discharged from hospital following treatment for emotional eating [20]. HMDs used in the studies were Samsung Gear (N = 3), HTC Vive (N = 2), Sony Glasstron (N = 2), Vuzix iWear (N = 2), Dell Visor Windows (N = 1), iTVGoggles (N = 1), model ITG-PCX3 (N = 1), Oculus Go (N = 1), and Sensics zSight (N = 1). One study used 3D wraparound projection technology, using two projectors, to display the 3D environment [26]. Three studies did not report HMD models [22, 30, 32]. Most studies used different software, and several did not provide software information.
Evidence of feasibility, acceptability, and effectiveness
Studies used self-report scales to measure relaxation, mood, anxiety, worry, and perceived stress [21,22,23, 26, 34, 36]. Other measures, such as observational teacher reports, were used to measure behavioral problems [35]. Some studies used physiological measurements, such as heart rate and galvanic stress response, as indicators of stress [22, 31, 36]. All studies had findings that indicated that VR relaxation is feasible, including in non-lab-based settings, such as psychiatric wards for various mental health conditions [33, 36] and in a specialist school [35]. Studies reported that VR relaxation is accessible [25] and can reduce pressure on clinicians [27, 31]. Studies indicated that nature-based VR environments are feasible as a low-intensity treatment for people with mental health conditions [26, 34], including for people who experience severe and acute conditions [33], and especially where participants lack access or exposure to real-world nature [25]. Most studies reported no user difficulties. A small number of participants in a minority of studies sometimes observed discomfort with HMDs [19] or experienced other user difficulties [23]. One study reported participants experiencing cybersickness, the phenomenon of motion sickness experienced in VR, which resulted in two drop-outs [34]; while others indicated some visual discomfort [33] and discomfort wearing HMDs over glasses [36]. However, all studies indicated overall acceptability of VR relaxation. Participants mostly reported that VR relaxation was calming [27, 32], helpful [31], enjoyable [27], relaxing [25, 33], useful [23], and an experience that they would recommend to others [27, 36].
Studies indicated that VR relaxation led to short-term improvements in levels of relaxation, and most reported reduced anxiety or stress. In most studies that included another, non-virtual form of relaxation exercise as a control condition, this exercise was also found to improve levels of relaxation and stress. However, VR relaxation was always more effective or equally effective when compared to the non-virtual relaxation exercises. Six studies measured perceived stress and reported improvements in levels, experience, or management of stress, four of which were RCTs or CCTs. Five of these studies showed significantly greater short-term improvements in stress levels, and experience of stress, following VR relaxation [26, 28, 29, 31, 36]. Studies also found post-VR reductions in worry [21,22,23], hopelessness [32], and negative affect [32, 34]. Four studies reported a decrease in depression or depressive symptoms [19,20,21, 31]. Studies also found an increase in positive affective states [27, 32, 34], positive emotions [30], positive thinking [31], and quality of life [21]. One CCT reported lower levels of subjective anxiety in both experimental and control groups with generalized anxiety disorder; however, physiological markers confirmed more significant changes in the experimental group who experienced VR relaxation [25]. Another CCT highlighted the effectiveness of nature exposure in VR, as outpatients with generalized anxiety disorder had significantly reduced levels of stress compared to an alternative, non-nature-based environment [26]. One large CCT, with the largest sample size (N = 175) of all studies included in this review, found that outpatients with significant stress at baseline could experience stress in more functional ways after three sessions of VR relaxation [29]. The small cohort study (N = 8) on adolescents with ASD and ADHD found that a biofeedback game reduced short-term state anxiety and disruptive classroom behavior [35]. The only study reporting longer-term data was an RCT that collected follow-up data from 36 inpatient female adults with eating disorders. This study found improved self-efficacy in eating after VR relaxation, which was supported by follow-up data after three months. Reduction in trait anxiety was also observed at follow-up [20].
Quality ratings
Eleven studies were given a global EPHPP rating of ‘strong’, four were rated ‘moderate’, and three were rated ‘weak’. See Table 2 for full-quality ratings. All ‘strong’ studies reported positive outcomes. All studies were moderate for selection bias as they were all judged to be somewhat likely to be representative of the target population. Thirteen of the eighteen studies were rated as strong for study design. In some cases, studies that described themselves as RCTs in the published paper were reclassified in the review as CCTs because the studies did not report information on method of randomization. Twelve out of eighteen studies were rated as strong for their controlling of confounding variables, and the remaining studies were weak, as little or no information was provided. All studies were rated moderate for blinding as information about whether the outcome assessor was aware of the intervention or whether the participants were aware of the research questions was not provided. For data collection methods, seven out of eighteen studies were rated strong, as they reported both validity and reliability. Twelve of the eighteen studies were rated strong for withdrawals and dropout, as 80–100% of their participants completed the study.
Discussion
This systematic review aimed to narratively synthesize current evidence of feasibility, acceptability, and effectiveness of VR relaxation for people with mental health conditions. The review included eighteen studies; there were thirteen controlled studies, of which seven were RCTs. Seventeen studies tested adult participants, with a range of mental health conditions, mostly anxiety and stress-related; and one study tested adolescents with ASD and ADHD. All studies used nature-based VR environments and provided evidence of feasibility, acceptability, and short-term effectiveness of VR relaxation to promote relaxation and reduce stress. A minority of studies highlighted emerging evidence for the applicability of VR relaxation to support service users on psychiatric wards; and for its application to a wider range of more severe mental health conditions, such as eating disorders, depression, bipolar disorder, and psychotic disorders. This wider application is consistent with previous research that indicates that VR is a tool that can support social functioning impairments in people with more severe mental health conditions, such as psychosis [37,38,39].
Although some of the comparison conditions, such as guided meditation and progressive muscle relaxation, were also found to be effective in aiding relaxation and reducing symptoms of anxiety, low mood, and stress [21, 34], the general outcome was that VR relaxation was more or equally effective compared to these other, non-VR-based relaxation interventions. This indicates that VR relaxation has potential to supplement existing relaxation techniques or provide users with alternative relaxation and stress-reduction options.
VR relaxation is a low-effort intervention in terms of attention and concentration due to its immersive nature; it has a standalone use; it has fewer requirements from staff and is less time intensive; and it can be used autonomously, even in the home. VR relaxation could be especially helpful during and after the COVID-19 pandemic, given that the pandemic has led to the increase and exacerbation of mental health problems [40]. This application may be especially timely given that VR has recently become much more affordable and more accessible in portable ways, and so this technology is likely to be available to more users than ever before [34, 41]. Nevertheless, the digital divide remains a significant problem and is highly likely to exclude people from lower socioeconomic backgrounds and various other groups who may be less likely to have access to technology, such as older adults [42]. Given that people from lower socioeconomic backgrounds are at greater risk of developing mental health problems, VR relaxation interventions may be less likely to reach this population and so this remains an ongoing challenge to make effective digital interventions more accessible [43].
Strengths and limitations of studies included in the review
Strengths of the studies included in this review are the innovative use of technology; the commonalities in VR environments and measures of stress, anxiety, and relaxation, which enables comparison between studies; and the frequent use of control groups and standardized pre- and post-intervention measures, which meant that the overall quality of the studies was acceptable.
Limitations of the studies include the small clinical samples in several studies; lack of large RCTs; and testing mostly working-age adults, female participants, and clinical samples with mainly anxiety disorders or stress-related problems, which limits generalizability, especially to other genders, age groups, and other mental health conditions. Use of mixed diagnosis samples could be interpreted as a weakness in that it can hinder comparison between studies; but it could also be perceived as a strength because stress is a transdiagnostic factor in many mental health conditions and DSM and ICD classifications are not neatly defined in clinical practice, given the many comorbidities, overlapping symptoms, and subthreshold symptoms. Most studies used self-report measures to assess relaxation, stress, and other outcome variables, and therefore their findings could be subject to researcher or participant bias. Use of physiological outcome measures was limited, which would be one way to address this bias. A major limitation of the research is lack of evidence of longer-term benefits of VR relaxation for people with mental health conditions given that only one study collected follow-up data. This is consistent with a similar finding about short-term evidence and lack of longer-term data in non-clinical samples [15]. Other methodological issues such as lack of controlling for potential confounding variables and lack of information on randomization and blinding also weakens the research. Given the dominance of positive findings, it is also possible that the literature is subject to publication bias.
Overall, studies indicate emerging evidence for the potential of VR relaxation for mental health service users, especially to treat anxiety or stress-related problems. However, at this stage, one should be cautious about making stronger claims about its effectiveness or about its application to a wider range of mental health conditions.
Strengths and limitations of the review
This is the first systematic review to narratively synthesize the current evidence of feasibility, acceptability, and effectiveness of VR relaxation for people with mental health conditions. The review included a comprehensive search strategy, using a combination of formal searches of four databases and non-indexed reference lists. The review used the EPHPP, which is an evidenced tool that assesses the methodological quality of quantitative studies, and was administered by independent reviewers, thus strengthening the methodological rigor of the review.
Important limitations of the review include the limited number of studies, and lack of standardization of interventions, conceptual definitions, and measures within the existing research. For instance, the concept of relaxation was interpreted and measured in the included studies using a variety of self-report surveys, physiological parameters, and qualitative observations, which lacks consistency and limits comparisons within the review. Similarly, despite the dominant use of nature-based themes, virtual environments used in the studies were not standardized, including both animated and video content; and there was great variation in HMDs and software, intervention tasks, level of interactivity, and number and duration of sessions, which also limits comparison between studies. In some cases, the interactivity component comprised participants making choices about which environments they explored, whereas other interventions included more active, gamified elements to the interactivity. Similarly, the role and level of input of facilitators was unclear and not standardized across studies. The review deliberately and necessarily employed a broad concept of mental health, including clinical samples with recognized diagnoses or conditions, symptoms consistent with a mental health diagnosis, and mixed samples of various diagnoses and conditions. This broad approach was intended to provide a comprehensive review of the clinical interventions that have been tested in what is still a relatively new field of research with a limited number and range of studies, but it could be interpreted as a limitation, and the broad scope of the review should be considered when interpreting the findings.
Lack of inclusion of gray literature, lack of qualitative research, and a search strategy that used a limited number of academic databases means it is possible the review has not included all studies relevant to VR relaxation for people with mental health conditions and, therefore, there may be additional evidence excluded from this review. Given that the EPHPP tool reclassifies RCTs as CCTs if they do not adequately describe the randomization method, regardless of whether the published paper describes itself as an RCT, it could be argued that the review underreports the number of RCTs in this area of research. Perceived limited information on certain domains, e.g., confounders, by researchers may also have impacted on quality ratings of studies.
Clinical applications
A previous systematic review on VR relaxation for the general population highlighted its possibility as a low-intensity intervention for people with mental health conditions [15]. This review is consistent with that finding and shows that most of the evidence for VR relaxation as a clinical intervention is in anxiety and stress-related problems, suggesting the possibility of piloting the VR relaxation in anxiety clinics; but the findings also suggest the potential of VR relaxation for service users with a wider range of mental health diagnoses. Given that stress is a major trigger and ongoing problem in a range of mental health conditions, including for people with severe mental health conditions on psychiatric wards, its application may be wider, as indicated by some of the inpatient studies included in this review.
There is now considerable research integrating VR with cognitive behavior therapies [12, 44]. There may be ways of integrating VR relaxation with cognitive behavioral therapy, as a behavioral means of coping with stress. In cognitive behavioral interventions that use VR relaxation, it may be helpful to work with service users to develop real-world applications for their relaxation practices that build on the experiential learning gained in the VR, as a way of creating a treatment that has sustainability and is tailored to individuals [45]. However, it is also important to recognize that VR relaxation has potential as a standalone intervention, that can stand apart from other psychosocial interventions, and gives people with mental health problems the same access to relaxation as the general population.
The increased availability, accessibility, and portability of VR indicates that VR relaxation may be a useful method of prevention, management, and treatment of mental health problems outside of the clinic, including at the homes and workplaces of people with mental health problems [15, 46, 47]. It could be particularly beneficial for those who lack access to real-world nature, such as people living in urban areas or those with mobility difficulties. Some caution to this interpretation might need to be applied to conditions like social anxiety, where use of home-based VR relaxation as a coping strategy might reduce beneficial exposure to real-world social situations, and inadvertently function as a maintenance factor or safety behaviour, potentially worsening symptoms [48]. Nevertheless, there are people with mental health conditions who can access real-world nature but do not do so because of their mental health problems, and VR relaxation may be a way to overcome this problem and make relaxation easier.
Future research
Future research should prioritize longitudinal studies to assess if there are sustained, longer-term benefits of VR relaxation for people with mental health conditions. These studies should aim to provide greater standardization of interventions, definitions, and measures; recruit larger numbers from more diverse populations, including a wider range of mental health conditions, and a variety of age groups, including young people and older adults, to aid generalisability. Mixed diagnosis samples powered adequately to perform subgroup analysis could be a useful dimension to this research. Service users should be involved in this future research and have a key role in development of VR relaxation interventions. A key next step would be to evaluate VR relaxation for people with mental health conditions in more naturalistic clinical and non-clinical settings, such as clinics, psychiatric wards, or in the home. These settings would provide further evidence of VR relaxation as a protective measure to reduce the strain on mental health services, especially given that existing studies are mainly conducted in laboratory settings. Future reviews of the literature might also consider using specific theoretical models of technology to provide a more in-depth analysis of the research.
Given the dominance of nature-based scenes in the environments, it would be useful to evaluate the importance of HMDs by comparing VR-based nature with similar scenes on 2D screens, including on mobile devices, particularly given the ultra-high-definition quality of many 2D screen projections, as this may provide a different kind of immersive user experience. Although 2D interventions are likely to be less immersive and experiential and may not hold users’ attention so effectively, they may still promote relaxation and reduce stress for people with mental health conditions. This may be one way to make these benefits available to a wider audience, potentially using technology that is likely to be more easily accessed or already possessed by many mental health service users.
Conclusion
This is the first systematic review to narratively synthesize current evidence on VR relaxation for people with mental health conditions. All studies used nature-based VR environments and indicated that they are feasible, acceptable, and effective in the short term to promote relaxation and reduce stress, especially for people with anxiety disorders and stress-related problems. Despite methodological limitations, this appears to be a promising intervention for people with mental health conditions and an important area of future research.
Data availability
Data sharing not applicable to this article.
References
Luo M et al (2020) The psychological and mental impact of coronavirus disease 2019 (COVID-19) on medical staff and general public–A systematic review and meta-analysis. Psychiatry Res 291:113190
Salari N et al (2020) Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: a systematic review and meta-analysis. Glob Health 16(1):1–11
Wilson D (2009) Anxiety and depression: it all starts with stress. Integr Med 8(3):42–44
Aas M et al (2014) A systematic review of cognitive function in first-episode psychosis, including a discussion on childhood trauma, stress, and inflammation. Front Psych 4:182
Martland N et al (2020) Are adult stressful life events associated with psychotic relapse? A systematic review of 23 studies. Psychol Med 50(14):2302–2316
Shah LBI et al (2014) Efficacy of psychoeducation and relaxation interventions on stress-related variables in people with mental disorders: a literature review. Arch Psychiatr Nurs 28(2):94–101
Klainin-Yobas P et al (2015) Effects of relaxation interventions on depression and anxiety among older adults: a systematic review. Aging Ment Health 19(12):1043–1055
Howarth A et al (2019) Effects of brief mindfulness-based interventions on health-related outcomes: a systematic review. Mindfulness 10(10):1957–1968
Li M et al (2020) Relaxation techniques for depressive disorders in adults: a systematic review and meta-analysis of randomised controlled trials. Int J Psychiatry Clin Pract 24(3):219–226
Dunley P, Papadopoulos A (2019) Why is it so hard to get help? Barriers to help-seeking in postsecondary students struggling with mental health issues: a scoping review. Int J Ment Heal Addict 17(3):699–715
Aziz HA (2018) Virtual reality programs applications in healthcare. J Health Med Inform 9(1):305
Freeman D et al (2017) Virtual reality in the assessment, understanding, and treatment of mental health disorders. Psychol Med 47(14):2393–2400
Bell IH et al (2020) Virtual reality as a clinical tool in mental health research and practice. Dialogues Clin Neurosci 22(2):169
Geraets CN et al (2021) Advances in immersive virtual reality interventions for mental disorders–a new reality? Curr opin Psychol 41:40–45
Riches S et al (2021) Virtual reality relaxation for the general population: a systematic review. Soc Psychiatry Psychiatr Epidemiol 56:1707–1727
Moher D et al (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 6(7):e1000097
Organization W.H. (2019) International statistical classification of diseases and related health problems, 11th edn. Available from: https://icd.who.int/. Accessed 23 Sept 2022
Thomas B et al (2004) A process for systematically reviewing the literature: providing the research evidence for public health nursing interventions. Worldviews Evid Based Nurs 1(3):176–184
Manzoni GM et al (2008) New technologies and relaxation: an explorative study on obese patients with emotional eating. J Cyberther Rehabil 1(2):182–192
Manzoni GM et al (2009) Can relaxation training reduce emotional eating in women with obesity? An exploratory study with 3 months of follow-up. J Am Diet Assoc 109(8):1427–1432
Malbos E et al (2020) Virtual reality for relaxation in the treatment of generalized anxiety disorder : a comparative trial. Annu Rev Cyberther Telemed 18:183–187
Gorini A et al (2010) Virtual reality in the treatment of generalized anxiety disorders. Stud Health Technol Inform 154:39–43
Pallavicini F et al (2009) Biofeedback, virtual reality and mobile phones in the treatment of generalized anxiety disorder (gad): a phase-2 controlled clinical trial. J Cyber Ther Rehabilit 2(4):315–327
Repetto C et al (2013) Virtual reality and mobile phones in the treatment of generalized anxiety disorders: a phase-2 clinical trial. Pers Ubiquit Comput 17(2):253–260
Tarrant J, Viczko J, Cope H (2018) Virtual reality for anxiety reduction demonstrated by quantitative EEG: a pilot study. Front Psychol 9:15
Wang TC et al (2020) Psychological and physiological responses in patients with generalized anxiety disorder: the use of acute exercise and virtual reality environment. Int J Environ Res Public Health 17(13):06
Mistry D et al (2020) Meditating in virtual reality: proof-of-concept intervention for posttraumatic stress. Psychol Trauma Theory Res Pract Policy 12(8):847–858
H Kim et al. (2021) Effect of virtual reality (VR) on stress reduction and change of physiological parameters including heartrate variability in people with high stress: an open randomized cross-over trial. Asia Pacific Psychiatry. Conference: 19th International Congress of the Pacific Rim College of Psychiatrists. Seoul South Korea. 13(1)
Maarsingh BM et al (2019) Changing stress mindset through Stressjam: a virtual reality game using biofeedback. Games Health J 8(5):326–331
Riva G et al (2008) Why you really eat? Virtual reality in the treatment of obese emotional eaters. Stud Health Technol Inform 132:417–419
Shah LB et al (2015) Efficacy of the virtual reality-based stress management program on stress-related variables in people with mood disorders: the feasibility study. Arch Psychiatr Nurs 29(1):6–13
Habak S et al (2021) Edge of the present: a virtual reality tool to cultivate future thinking, positive mood and Wellbeing. Int J Environ Res Public Health 18(1):13
Mark I et al (2021) The use of virtual reality in a psychiatric intensive care unit: a pilot study. J Psychiatr Intensive Care 17:123–128
Veling W et al (2021) Virtual reality relaxation for patients with a psychiatric disorder: crossover randomized controlled trial. J Med Internet Res 23(1):e17233
Bossenbroek R et al (2020) Efficacy of a virtual reality biofeedback game (DEEP) to reduce anxiety and disruptive classroom behavior: single-case study. Jmir Ment Health 7(3):18
Tan HLE et al (2021) Investigating the effects of a virtual reality-based stress management programme on inpatients with mental disorders: a pilot randomised controlled trial. Int J Psychol 56(3):444–453
Riches S et al (2021) Virtual reality-based assessment and treatment of social functioning impairments in psychosis: a systematic review. Int Rev Psychiatry 33:337–362
Valmaggia LR et al (2016) Virtual reality in the psychological treatment for mental health problems: an systematic review of recent evidence. Psychiatry Res 236:189–195
Veling W, Moritz S, Van Der Gaag M (2014) Brave new worlds—review and update on virtual reality assessment and treatment in psychosis. Schizophr Bull 40(6):1194–1197
Xiong J et al (2020) Impact of COVID-19 pandemic on mental health in the general population: a systematic review. J Affect Disord 277:55–64
Jerdan SW et al (2018) Head-mounted virtual reality and mental health: critical review of current research. Jmir Serious Games 6(3):12
Robotham D et al (2016) Do we still have a digital divide in mental health? A five-year survey follow-up. J Med Int Res 18(11):e309
Reiss F (2013) Socioeconomic inequalities and mental health problems in children and adolescents: a systematic review. Soc Sci Med 90:24–31
Berkhof M et al (2021) Virtual reality cognitive-behavioural therapy versus cognitive-behavioural therapy for paranoid delusions: a study protocol for a single-blind multi-Centre randomised controlled superiority trial. BMC Psychiatry 21(1):1–10
Riches S et al (2020) Subjective experience of paranoid ideation in a virtual reality social environment: a mixed methods cross-sectional study. Clin Psychol Psychother 27(3):337–345
Riches S, Smith H (2022) Taking a break in the ‘new normal’: virtual reality relaxation for a stressed workforce. Mental Health Rev J 27(2)
S Riches et al (In press) Virtual reality and immersive technologies to promote workplace wellbeing: a systematic review. J Mental Health
Mayo-Wilson E et al (2014) Psychological and pharmacological interventions for social anxiety disorder in adults: a systematic review and network meta-analysis. Lancet Psychiatry 1(5):368–376
Author information
Authors and Affiliations
Corresponding author
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Riches, S., Jeyarajaguru, P., Taylor, L. et al. Virtual reality relaxation for people with mental health conditions: a systematic review. Soc Psychiatry Psychiatr Epidemiol 58, 989–1007 (2023). https://doi.org/10.1007/s00127-022-02417-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00127-022-02417-5