
Abstract
Purpose
Stigma is a common barrier to mental health professionals (MHPs) seeking help for occupational stress and burnout, although there is a lack of psychometrically sound tools to measure this construct. The current study aimed to develop and validate a scale (the Mental Health Professional Stigma Scale; MHPSS) for this purpose.
Methods
The MHPSS and related measures were completed by 221 Australian MHPs via online survey, with a subsample completing the MHPSS again 2 weeks after initial completion.
Results
Exploratory factor analysis revealed a four-factor solution, comprising of 13 items and accounting for 50.16% of variance. Factors were Perceived Other Stigma, Perceived Structural Stigma, Personal Stigma, and Self stigma. The internal consistency, test–retest reliability, and validity of the scale were supported.
Conclusions
The MHPSS has utility to capture stigmatising attitudes and beliefs related to occupational stress and burnout among MHPs. It may be used to assist in the development and evaluation of initiatives to reduce stigma and increase help-seeking among MHPs.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The prevalence and impact of stress and burnout in mental health professionals (MHPs) are well-documented [1], with an average of 40% experiencing high emotional exhaustion [2]. In addition to the occupational stressors experienced by other health professionals, such as time pressure, workload, and ongoing contact with the physical and emotional pain of others [3, 4] MHPs also encounter additional unique stressors, such as greater probability of difficult interactions with patients and families, patient suicide, and the stigma associated with the field [5]. The prevalence of burnout among mental health professionals (MHPs) has been estimated at between 21 and 67% [1]. However, help-seeking among MHPs remains low [6], with stigma (e.g., fear of colleagues finding out about their difficulties) emerging as a key barrier preventing MHPs from seeking help [6]. Research in this field has been hampered by a lack of psychometrically valid tools to measure stigma of occupational stress and burnout among MHPs. Such a tool would allow for more rigorous measurement and understanding of this construct, as well as for the accurate assessment of interventions to reduce stigma among MHPs.
Occupational stress and burnout among MHPs
Occupational stress is characterised by physiological and psychological reactions that occur when there is a discrepancy between a person’s workplace demands and their capacity to cope with those demands [7, 8]. Prolonged stress can lead to the psychological syndrome of burnout, which is marked by feelings of depletion and overwhelming exhaustion, heightened cynicism, detachment, and an inability to feel accomplishment within one’s work [9, 10].
Occupational stress and burnout are associated with numerous adverse outcomes for MHPs, their patients, and the healthcare systems in which they work [1, 5, 8, 11, 12]. MHPs report that burnout affects their empathy, communication, therapeutic alliance, and patient engagement [13]. It has also been associated with poorer expectations about patient recovery by MHPs [14] and contributes to additional organisational stressors through increased absenteeism and staff turnover [1].
Stigma and help-seeking
Despite the negative outcomes associated with the experience of stress and burnout, many MHPs do not seek help when experiencing distress. Edwards and Crisp [6] reported over half (57%) of their sample of MHPs had not sought help when it was needed [6], with stigma emerging as a common factor among the barriers to help-seeking identified by the MHPs. Similarly, a review of stigma and help-seeking found that health professionals were more likely to report the experience of stigma as a barrier to help seeking when compared to other professionals [15] and among psychiatrists, is the most commonly cited reason for choosing to not disclose personal mental health concerns [16].
Four types of stigma have commonly been linked to help-seeking for mental health: public (other) stigma; personal stigma; self-stigma; and structural stigma [17, 18]. Public stigma refers to how a person perceives that the general population typically views a person with the condition, whilst personal stigma refers to the stigmatising attitudes held by oneself towards the person or population with that condition [17, 19]. Self-stigma involves the attitudes and perceptions a person with a condition may hold about themselves, whilst structural stigma refers to limitations (real or perceived) placed on persons with mental illness as a result of intentional or unintentional societal level policies and practices of organisations or institutions [20,21,22].
Within these types of stigma, MHPs may experience unique aspects that prevent or delay help-seeking behaviours [6, 23]. Harris et al. [23] suggest a culture of nondisclosure exists within the mental health profession, and that this non-disclosure works to increase stigma among MHPs. Registration requirements concerning professional impairment and mandatory reporting may contribute to this culture of non-disclosure within the professions [6, 24]. Di Benedetto [25] suggests that implicit in legal and ethical mandates for the mental health profession is the faulty notion that MHPs should be immune to mental health problems. Fears of career and organisational repercussions from disclosing difficulties, negative views from and toward colleagues experiencing difficulties, and the view that as health professionals one should be able to manage such difficulties without external intervention are reported to perpetuate stigma within the field [26]. These concerns map directly to issues of public, personal, self, and structural stigma within the MHP field, and suggest there are unique aspects to the experience of stigma within this population. However, to date stigma has primarily been measured using general stigma scales.
Measures of stigma
To the researchers’ knowledge there is no existing standardised instrument designed to measure MHP’s stigmatising attitudes and perceptions of stigma towards stress and burnout in their work. Current instruments are inadequate to capture this phenomenon largely due to the broad label of mental illness and the focus of most measures on only one type of stigma. Furthermore, these measures are often focused on how MHPs might stigmatise their patients, rather than focusing within the profession [27]. To improve help-seeking in this population, there is a need to understand the effects and interrelationships of these types of stigma together, in particular the effects of structural stigma which is often omitted in scales of stigma for MHPs [28,29,30]. The Stigma of Occupational Stress Scale for Doctors (SOSS-D) does measure these attitudinal barriers to help-seeking and has demonstrated strong psychometric properties and structural validity [26]. However, the SOSS-D only targets three of the four facets of stigma (perceived other stigma, perceived structural stigma, and personal stigma) and was developed for use only among medical practitioners. Although there is overlap between the occupational groupings, the differences in training, job roles, and professional culture between medical and the broader MHP populations suggests the need for a measure specifically for use among MHPs.
The current study
The aim of this study was to develop and test a measure of stigma of occupational stress and burnout among MHPs. An initial psychometric investigation was also planned for the final scale, focussing on structural validity, internal consistency, test–retest reliability, and convergent and divergent validity. As a newly developed measure, no predictions were made as to the factor structure of the Mental Health Professionals Stigma Scale (MHPSS) and its internal consistency or test–retest reliability. Rather, these were analysed in an exploratory manner and interpreted with reference to established guidelines. It was predicted that the Mental Health Professionals Stigma Scale (MHPSS) and underlying stigma constructs would exhibit convergent validity through moderate to high positive correlations with similar stigma measures and divergent validity through weak correlations with psychological distress.
Method
Participants
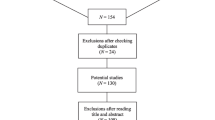
A minimum sample size of 119 participants was required in accordance with the participant to variable (7:1) ratio recommended by the consensus based standards for the selection of health instruments checklist [31]. Australian MHPs were recruited from public, private, and non-government organisation and services, with 253 participants accessing the survey and 221 completing the minimum MHPSS questionnaire for inclusion. An overall response rate was unable to be determined based on the use of electronic advertisements and snowball methods of recruitment. Recruitment notices invited practising MHPs to take part in a brief online survey related to practitioner health and wellbeing. Of the 221 participants 184 provided demographic data, with 160 (87.0%) identified as female, 23 as male (12.5%), and 1 participant as being “other gender” (0.5%). Participants ranged in age from 23 to 78 years (M = 43.81, SD = 13.10) and had an average of 12.81 years (SD = 10.43) of experience working in the mental health field. On average participants spent 20.72 h per week (SD = 11.97; MIN = 0, MAX = 45) in direct client care. There were 49 (26.9%) psychologists, 11 (6.0%) occupational therapists, 23 (12.6%) social workers, 13 (7.1%) General Practitioners, 7 (3.8%) psychiatrists, 29 (15.9%) nurses or mental health nurses, 25 (13.7%) counsellors, and 25 (13.7%) other MHPs (not listed, e.g. school guidance counsellors, provisionally registered psychologists, youth workers, aboriginal mental health workers, and consumer consultants/partners in recovery) who participated in the study. Participants worked in public (N = 78; 43.6%), private (N = 54; 30.2%), or non-government organisation (N = 47; 26.3%) sectors.
Materials and measures
Development of the MHPSS
As the closest measure with strong psychometric properties, all original items from the SOSS-D [26] were revised to specifically address MHPs rather than medical doctors. The relevance of items was then considered with reference to existing literature and consultation with mental health professionals and field experts. All 11 items were considered to have relevance to MHPs and were retained. Ten original items, developed based on previous literature, were included to measure the construct of self-stigma. Two mental health experts reviewed these items, and selected four of the ten items as being relevant, as well as suggesting an additional two self-stigma items. The modified scale was provided to a panel of current mental health professionals, comprised of seven professionals with backgrounds in clinical psychology, social work, occupational therapy, and mental health nursing. Years of experience working in mental health ranged from 3 to 23 years (M = 10.43, SD = 7.30). The panel completed their feedback independently and responded to a short feedback questionnaire.
Input from MHPs yielded two key recommendations. The first involved duplicating items to have separate items pertaining to management and colleagues. However, to account for the diversity of the mental health profession, in which not all MHPs work in a workplace with a management structure (for example, private practice) and the potential to substantially increase burden and repetition within the measure, this recommendation was not implemented. The second recommendation related to support for the addition of items on self-stigma, as being a particularly relevant construct for MHPs. As such, the final version of the MHPSS put forward for further investigation contained 17 items. For each item, participants respond using 7-point rating scales ranging from 1 (strongly disagree) to 7 (strongly agree), with higher scores indicating greater stigmatising attitudes and perceptions.
Opening minds stigma scale for health care providers (OMSHC)
The OMSHC is a 15-item measure designed to capture general stigmatising attitudes and behaviours of health care providers towards persons with mental illness [32]. The scale is a self-report measure employing a 5-point rating scale from 1 (strongly disagree) to 5 (strongly agree). Items are summed, with higher scores representing more stigmatising attitudes and behaviours (Modgill et al. 2014). The 15-item version of the OMSHC has demonstrated excellent overall internal consistency (α > 0.80) for allied health professionals, nurses, and social workers. Internal consistency in the present study was 0.73.
Perceived discrimination and devaluation scale (PDD)
An updated version of the Perceived Devaluation Scale was used [33]. The 12-item scale measures the degree to which respondents perceive most other people would devalue or discriminate against a person with a mental illness. Participants respond using 4 point rating scales, ranging from 1 (strongly disagree) to 4 (strongly agree). Higher scores reflect a stronger perception that others will likely discriminate and devalue people recognised as having lived experience of mental illness. The scale has previously demonstrated excellent internal consistency (α = 0.86 to α = 0.88) and was also excellent (0.86) in the current study.
Kessler psychological distress scale (K10)
The K10 is a 10-item self-report questionnaire designed to provide an indication of a person’s global distress [34]. Respondents rate the frequency with which they have experienced each item symptom over the previous 30 days, using 5-point rating scales ranging from 1 (none of the time) to 5 (all of the time). Higher scores are indicative of greater psychological distress. The K10 has demonstrated excellent internal consistency (α = .86), which was also found to be excellent (0.91) in the current study.
Procedure
Ethical approval was granted from the institution’s Human Research Ethics Committee (protocol 2017/398). Participants accessed the online survey through electronic links which were distributed via email, professional newsletters, social media forums, and workplace briefings. Informed consent was obtained and participants were directed to the completion of the self-report questionnaire package, which took approximately 30 min to complete. Study participants had the chance to enter a prize draw. Available prizes were one $100 department store gift card and five $20 department store gift cards, given individually. All survey responses were anonymous. Participants who entered the prize draw were redirected to a separate survey to enter their contact details. Participant generated identification codes were used to match responses over time, for the subgroup (N = 16) of participants who completed the follow-up survey 2 weeks after completion of the initial survey. The follow up survey contained only the MHPSS, with data used for test–retest correlation analyses.
Results
Data screening and assumptions
Checks for normality revealed skewness and kurtosis were present on a number of the study variables. Analyses were performed with transformed and untransformed data. However, as transformations did not alter the significance or interpretation of results, only untransformed data are reported. The data met the assumptions for linearity and multicollinearity [35], with bivariate correlations displayed in Table 1. A small number of multivariate outliers were identified. Analyses were conducted with and without the outliers. As the outliers did not change the pattern or significance of results, all cases were retained.
Initial factor analysis
Principle axis factoring (PAF) was conducted. The 17 items supported factorability, with many coefficients of 0.3 or greater present in the correlation matrix, the Kaiser–Meyer–Olkin (KMO) minimum value exceeded (0.88) [36], Bartlett’s Test of Sphericity significant (χ2 (136) = 1445.82, p < 0.001), and communalites greater than 0.3 present for most variables. While low communalities were found for two items these items were not removed as they were above the recommended exclusion limit (< 0.2) recommended by Child [37]. Linearity of variables was also supported and no issues of multicollinearity among varibables were identified. Thus data were considered suitable for EFA and all 17 items were included in the analysis.
To determine the number of factors to extract, an unrotated PAF analysis was conducted. Based on Kaiser’s [38] criterion four factors were suggested for extraction. The scree plot indicated a three- or four-factor structure. However, as the four-factor solution produced the fewest cross-loadings and was consistent with the theoretical underpinnings of the MHPSS, a decision was made to extract four factors.
Within this four-factor solution, item loadings on the first, second, and third factors supported meaningful interpretation of theoretical constructs. However, the fourth factor contained items expected to measure theoretically different constructs and interpretation was difficult. Further examination of this item indicated three items shared theoretical bases and had materialised as a factor in previous research [26]. As such, four items (4, 7, 10, 16) were removed from the analysis as they loaded weakly, had cross loadings, or were not meaningful in the context of other items from the factor. The 13 remaining items comprised the final MHPSS scale (see Appendix A) and were submitted to further EFA with promax rotation.
Final factor analysis
The final scale was subjected to PAF with promax rotation. Data were factorable, based on the same criteria as the previous EFA (communalities displayed in Table 2). PAF revealed the presence of four factors with eigenvalues exceeding 1, explaining 31.13%, 9.99%, 4.95%, and 4.09% of the variance, respectively with this result also consistent with the scree plot. The four-factor solution explained a total of 50.16% of the variance. This solution had the closest representation of simple structure, with three of the four factors exhibiting a number of high factor loadings. The fourth factor had one high loading, two moderate loadings, and one relatively small loading. All variables loaded onto only one factor. All factors demonstrated correlations with all other factors with most of these correlations in the moderate range, supporting oblique (promax) rotation (Table 3).
Factor 1 comprised of four items consistent with the construct of Perceived Structural Stigma, and was named as such. Factor 2, consisted of three items reflecting the construct of Self Stigma. Factor 3, comprised of three items consistent with the construct of Perceived Other Stigma. The fourth factor was comprised of three items consistent with the construct of Personal Stigma.
Reliability analyses
Internal consistency
Alpha coefficients for all MHPSS subscales (Table 3), except Personal Stigma, exceeded Nunnally’s [39] threshold of 0.70 for acceptable internal consistency in early phases of scale development.
Test–retest reliability
Intraclass correlation coefficients (ICC) two-way random absolute agreement with 95% confidence intervals (CIs) were calculated to determine test–retest reliability over a 2-week interval, with high reliability found across all scales (Table 3).
Validity analyses
Construct validity of the MHPSS was investigated using Pearson’s bivariate correlations (Table 4).
Convergent validity
A significant moderate positive correlation was found between the MHPSS total scores and the Opening Minds Stigma Scale for Health Care Professionals (OMSHC). The Self Stigma and Personal Stigma subscales also demonstrated a significant moderate positive relationship with the OMSHC. Significant but weak positive correlations were found between the MHPSS and the PDD.
Divergent validity
A weak but significant positive correlation was found between MHPSS total scores and the K10 indicating the constructs were not measuring the same construct but were not however completely distinct.
Discussion
This research aimed to develop and test a measure of stigma of occupational stress and burnout among MHPs. A structured approach to scale development was used, integrating previous literature and scales from the broader health and medical field. MHPs and experts were also involved in the development stages, following which, the underlying factor structure and initial psychometric properties of the MHPSS were assessed.
Structural validity
The four interrelated factors of the MHPSS were Perceived Other Stigma, Perceived Structural Stigma, Personal Stigma and Self Stigma (50.16% total variance explained). Perceived Other Stigma contained items related to how MHPs perceive the majority of other MHPs hold stigmatising attitudes towards stress and burnout.
Perceived Structural Stigma items reflected MHP’s perceptions of stigma of stress and burnout within the context of broader structural influences operating in their workplace. These items related to broad conceptualisations of stigma within the workplace rather than specifically from either managers of colleagues. A recommendation to duplicate items as pertaining to either managers or colleagues was made during the MHP panel feedback stage of scale development. However, the decision was made to keep these items relating to the workplace more broadly due to concerns that items specific to the role of management may not be relevant for the significant proportion of MHPs who work in solo private practice settings within the Australian context (e.g., 24.7% of psychiatrists, 21.1% of psychologists, [40]). It should be noted though, that whilst this decision was made for pragmatic reasons, it does have implications for the conceptualisation of structural stigma provided by the scale. Future versions of the scale could look at revisions to these items to better differentiate between stigma from specific sources within the workplace, and would likely provide greater insight into these issues for MHPs. As a preliminary tool though, the structural validity of the broader conceptualisation of structural stigma was supported in the current version.
Personal Stigma items reflected the personal attitudes MHPs hold towards occupational stress and burnout among MHPs. Finally, Self-Stigma was the final factor to emerge in the MHPSS. Items provide an impression of the attitudes MHPs express towards their own hypothetical experience of stress or burnout. The factors were consistent with previous conceptualisations of these constructs in the field (e.g., [18, 21, 41, 42]).
Reliability
Reliability analyses provided a good degree of support for the MHPSS. Internal consistency of the total MHPSS scale was good, with three of the four subscales (perceived structural stigma, self-stigma, and perceived other stigma) also exhibiting acceptable to good internal consistency. The personal stigma subscale was below the conventionally accepted threshold for internal consistency, suggesting the need for caution in interpretation of this subscale. One explanation for this finding is that this subscale may have been particularly susceptible to social desirability effects. Future research should include a measure of social desirability. Test–retest reliability was however found to be excellent across all subscales and the total scale.
Convergent and divergent validity
It was predicted that the MHPSS would demonstrate convergent validity with measures of similar stigma constructs through moderate to high positive correlations. Partial support for this hypothesis was found. A significant moderate positive correlation was found between the OMSHC, a measure of stigmatising attitudes and behaviours in health care professionals, and the MHPSS total scale, Personal, and Self Stigma subscales. Although the Perceived Other and Perceived Structural subscales showed weaker correlations, these were still in the expected direction and logical given the OMSHC does not contain items corresponding to these constructs [32]. The PDD, which measured the extent to which respondents believe most other people hold stigmatising attitudes towards people with mental illness, had a significant weak positive relationship with the MHPSS total scale. A weak but significant correlation was also found between the PDD and the Perceived Other Subscale of the MHPSS, with other subscales demonstrating very weak relationships. Although the relationships were weaker than expected, the pattern provides support for the convergent validity of the MHPSS, in particular with the Perceived Other Stigma subscale and PDD measuring similar constructs. The weaker strength may be accounted for by the PDD being developed on a general population sample and also referring to the broader “mental illness” term rather than stress and burnout specifically. As such, although the convergent validity relationships were weaker than expected, the pattern provides confidence that the MHPSS is measuring the intended concepts.
The divergent validity of the MHPSS was supported by weak positive correlations between the scale and psychological distress (K10). This relationship indicated that as expected, the MHPSS shared only a small amount of variance with psychological distress. This overlap could be explained by the potential for stigma to exacerbate distress and deter help seeking, which in turn can increase distress.
Strengths and limitations
Results of the current study should be considered within the context of a number of limitations. In particular, not all validity domains could be assessed in the current study. Further research is required to assess the predictive and criterion validity of the measure, as well as relevance across different populations. In addition, it is important to be aware that sampling may be affected by survivor bias. In this study, survivor bias would refer to the potential for MHPs with high levels of burnout to be more likely to leave the profession early, and thus their experiences within the profession may not be captured, biasing the sample.
The recruitment methods employed likely also influenced results of the currently study. Recruitment methods such as the use of posts on social media, meant that a response rate for the sample was unable to be determined. As such, the representativeness of the sample to the broader profession cannot be inferred. Within the specific professions of MHPs some were also represented more than others, and future research may be required to test the scale among the individual mental health professions.
Lastly, the sample was also predominantly (87%) female and results should thus be interpreted with some caution. The structure and validity of the scale may require further investigation among a larger sample of male MHPs to assess for any possible differences in performance of the scale across genders. However, it should also be noted that despite the large proportion of females in this sample, this does not necessarily indicate that the sample was biased with respect to the general population of MHPs. In the Australian context these fields are largely female dominated. According to 2019 registrations with the Australian Health Practitioner Regulation Agency (AHPRA), females comprised 80% of the psychologist workforce, 88% of the nursing workforce, and 91% of the occupational therapy workforce. As such, the gender composition of the current sample was not unlike that of the broader MHP population.
Despite these limitations, the current study contained a number of strengths. In particular, care was taken to ensure MHPs were included in the development and design of the MHPSS, enhancing the validity of the measure within this population. Furthermore, care was taken to follow the COSMIN guidelines for scale development, to ensure an empirical approach was taken to testing and interpretation of the scale properties.
Practical implications and conclusions
This study provided initial support for the MHPSS as a valid and reliable measure of stigma towards occupational stress and burnout among MHPs. Future research should focus on further development, refinement, and confirmation in independent samples. The measure has utility for researchers, practitioners, and organisations interested in stigma and occupational stress and burnout among MHPs.
In particular, we anticipate that the MHPSS may have utility for investigating the interplay of the different stigma types on MHPs’ attitudes and perceptions, enabling the development and empirical assessment of interventions to improve help-seeking and mental health among this population. In assessing for stigma among this population, we have not provided guidance for users of the MHPSS on cutoffs or score bands to indicate problematic levels of stigmatised beliefs. Similar to conceptualisations of the broader barriers to care concept (e.g., [43]), we expect that stigmatised beliefs will likely have a cumulative effect, with greater endorsement of stigmatised beliefs being associated with reduced likelihood of disclosure or help-seeking. However, it is also possible that endorsement of a single stigmatised belief (for example, relating to potential discrimination in the workplace), when of significant distress may be sufficient to preventing help-seeking. As such, use of the scale may provide insight into overall patterns of beliefs and relative endorsement of stigma, although clinical attention should also be paid to the relationship each belief has with help-seeking for the individual. To this end, the scale may be useful in assessing macro level patterns of stigma in populations and workplaces, as well as understanding an individual’s potential barriers to treatment seeking. Tailored individual and group level interventions may then be developed to target salient stigmatised beliefs and challenge potential cultural issues within professions and workplaces. We believe that the MHPSS may be a valuable tool to contribute to the emerging empirical knowledge base on stigmatising attitudes and perceptions of occupational stress and burnout among MHPs.
Data Availability
The data is available from the authors upon request.
References
Morse G et al (2012) Burnout in mental health services: a review of the problem and its remediation. Adm Policy Mental Health Mental Health Serv Res 39(5):341–352
O’Connor K, Neff DM, Pitman S (2018) Burnout in mental health professionals: a systematic review and meta-analysis of prevalence and determinants. Eur Psychiatry 53:74–99
McCann CM et al (2013) Resilience in the health professions: a review of recent literature. Int J Wellbeing 3(1):60–81
Clough BA et al (2017) Psychosocial interventions for managing occupational stress and burnout among medical doctors: a systematic review. Syst Rev 6(1):144
Rössler W (2012) Stress, burnout, and job dissatisfaction in mental health workers. Eur Arch Psychiatry Clin Neurosci 262(2):65–69
Edwards JL, Crisp DA (2017) Seeking help for psychological distress: barriers for mental health professionals. Aust J Psychol 69(3):218–225
Karasek Jr, RA (1979) Job demands, job decision latitude, and mental strain: Implications for job redesign. Adm Sci Q 24(2):285–308
Rabin S, Feldman D, Kaplan ZE (1999) Stress and intervention strategies in mental health professionals. Psychol Psychother 72(2):159–169
Maslach C, Jackson SE (1984) Burnout in organizational settings. Appl Soc Psychol Annual 5:133–153
Maslach C, Jackson SE, Leiter MP (1986) Maslach burnout inventory. 3rd edn. Consulting Psychologists Press, Palo Alto, CA
Ray SL et al (2013) Compassion satisfaction, compassion fatigue, work life conditions, and burnout among frontline mental health care professionals. Traumatology 19(4):255–267
Green AE et al (2014) The roles of individual and organizational factors in burnout among community-based mental health service providers. Psychol Serv 11(1):41
Salyers MP et al (2015) Clinicians’ perceptions of how burnout affects their work. Psychiatr Serv 66(2):204–207
Salyers MP et al (2013) Job satisfaction and burnout among VA and community mental health workers. Adm Policy Mental Health Mental Health Serv Res 40(2):69–75
Clement S et al (2015) What is the impact of mental health-related stigma on help-seeking? A systematic review of quantitative and qualitative studies. Psychol Med 45(01):11–27
White A et al (2018) Barriers to mental healthcare for psychiatrists. Psychiatr Bull 30(10):382–384
Corrigan PW (2004) How stigma interferes with mental health care. Am Psychol 59(7):614
Schnyder N et al (2018) Association between mental health-related stigma and active help-seeking: systematic review and meta-analysis. Br J Psychiatry 210(4):261–268
Link BG, Phelan JC (2001) Conceptualizing stigma. Ann Rev Sociol 27(1):363–385
Corrigan PW et al (2010) Self-stigma and coming out about one’s mental illness. J Commun Psychol 38(3):259–275
Corrigan PW, Markowitz FE, Watson AC (2004) Structural levels of mental illness stigma and discrimination. Schizophr Bull 30(3):481
Overton SL, Medina SL (2008) The stigma of mental illness. J Counsel Dev 86(2):143–151
Harris JI, Leskela J, Hoffman-Konn L (2016) Provider lived experience and stigma. Am J Orthopsychiatr 86(6):604
Dattilio FM (2015) The self-care of psychologists and mental health professionals: a review and practitioner guide. Aust Psychol 50(6):393–399
Di Benedetto M (2015) Comment on “the self-care of psychologists and mental health professionals”(Dattilio, 2015)—working with the mentally ill is a mental health hazard: what can we do about it? Aust Psychol 50(6):400–404
Clough BA, Ireland MJ, March S (2017) Development of the SOSS-D: a scale to measure stigma of occupational stress and burnout in medical doctors. J Mental Health 28(1):1–8
Yang LH, Link BG (2015) Measurement of attitudes, beliefs and behaviors of mental health and mental illness. https://sites.nationalacademies.org/cs/groups/dbassesite/documents/webpage/dbasse_170048.pdf. Accessed 26 June 2018
Link BG et al (2004) Measuring mental illness stigma. Schizophr Bull 30(3):511–541
Pescosolido BA, Martin JK (2015) The stigma complex. Ann Rev Sociol 41:87–116
Pugh T, Hatzenbuehler M, Link B (2018) Structural stigma and mental illness. https://sites.nationalacademies.org/cs/groups/dbassesite/documents/webpage/dbasse_170045.pdf. Accessed 26 June 2018
Mokkink LB (2017) COSMIN risk of bias checklist. https://cosmin.nl/wp-content/uploads/COSMIN_risk-of-bias-checklist_dec-2017.pdf. Accessed 26 June 2018
Modgill G et al (2014) Opening minds stigma scale for health care providers (OMS-HC): examination of psychometric properties and responsiveness. BMC Psychiatr 14(1):120
Link BG et al (2015) Understanding the importance of “symbolic interaction stigma”: how expectations about the reactions of others adds to the burden of mental illness stigma. Psychiatr Rehabil J 38(2):117
Kessler RC et al (2002) Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychol Med 32(6):959–976
Tabachnick BG, Fidell LS (2007) Using multivariate statistics. Pearson/Allyn and Bacon, Boston
Kaiser HF (1970) A second generation little jiffy. Psychometrika 35(4):401–415
Child D (2006) The essentials of factor analysis. Continuum, New York
Kaiser HF (1974) An index of factorial simplicity. Psychometrika 39(1):31–36
Nunnally JC, Bernstein IH, Berge JMT (1967) Psychometric theory, vol 226. McGraw-hill, New York
Australian Institute of Health and Welfare (2019) Mental Health Services in Australia. https://www.aihw.gov.au/reports/mental-health-services/mental-health-services-in-australia. Accessed 7 Nov 2019
Link BG (1987) Understanding labeling effects in the area of mental disorders: an assessment of the effects of expectations of rejection. Am Sociol Rev 52(1):96–112
Corrigan PW, Watson AC (2002) The paradox of self-stigma and mental illness. Clin Psychol Sci Pract 9(1):35–53
Mohr DC et al (2006) Barriers to psychotherapy among depressed and nondepressed primary care patients. Ann Behav Med 32(3):254–258
Funding
None to declare.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no competing interests.
Ethical statement
None to declare.
Appendix A: The Mental Health Professionals Stigma Scale (MHPSS) for occupational stress and burnout
Appendix A: The Mental Health Professionals Stigma Scale (MHPSS) for occupational stress and burnout
The following items relate to occupational stress and burnout. Occupational stress occurs in, or as a result of, the workplace. Burnout can be conceptualised as a specific type of occupational stress. It is the chronic depletion of energy that results from the ongoing demands of one’s occupation. Please use the scales below to indicate the extent to which you agree or disagree with the following statements.
- 1.
A mental health professional who is experiencing occupational stress or burnout would be treated fairly compared to any other mental health professional.
Strongly disagree
Disagree
Somewhat disagree
Neither agree nor disagree
Somewhat agree
Agree
Strongly agree
1
2
3
4
5
6
7
- 2.
I would try to distance myself from a mental health professional who was experiencing occupational stress or burnout.
Strongly disagree
Disagree
Somewhat disagree
Neither agree nor disagree
Somewhat agree
Agree
Strongly agree
1
2
3
4
5
6
7
- 3.
As a mental health professional, I should be able to manage any stress or burnout myself without seeking help from others.
Strongly disagree
Disagree
Somewhat disagree
Neither agree nor disagree
Somewhat agree
Agree
Strongly agree
1
2
3
4
5
6
7
- 4.
If I were to experience stress or burnout in my job I should be able to snap out of it.
Strongly disagree
Disagree
Somewhat disagree
Neither agree nor disagree
Somewhat agree
Agree
Strongly agree
1
2
3
4
5
6
7
- 5.
Where I work, any mental health professional who was experiencing occupational stress or burnout would be given understanding and support.
Strongly disagree
Disagree
Somewhat disagree
Neither agree nor disagree
Somewhat agree
Agree
Strongly agree
1
2
3
4
5
6
7
- 6.
A mental health professional who experiences occupational stress or burnout is somehow less capable than a mental health professional who does not experience those difficulties.
Strongly disagree
Disagree
Somewhat disagree
Neither agree nor disagree
Somewhat agree
Agree
Strongly agree
1
2
3
4
5
6
7
- 7.
Where I work, a mental health professional who reports experiencing occupational stress or burnout is more likely to experience discrimination or prejudice.
Strongly disagree
Disagree
Somewhat disagree
Neither agree nor disagree
Somewhat agree
Agree
Strongly agree
1
2
3
4
5
6
7
- 8.
Most mental health professionals would consider the experience of occupational stress or burnout as a sign that the mental health professional is not ‘right’ for the profession.
Strongly disagree
Disagree
Somewhat disagree
Neither agree nor disagree
Somewhat agree
Agree
Strongly agree
1
2
3
4
5
6
7
- 9.
Where I work, a mental health professional who was experiencing occupational stress or burnout would probably be better off not telling anyone.
Strongly disagree
Disagree
Somewhat disagree
Neither agree nor disagree
Somewhat agree
Agree
Strongly agree
1
2
3
4
5
6
7
- 10.
If I were to experience stress or burnout in my job, I should be able to fix it on my own.
Strongly disagree
Disagree
Somewhat disagree
Neither agree nor disagree
Somewhat agree
Agree
Strongly agree
1
2
3
4
5
6
7
- 11.
Most mental health professionals would consider a mental health professional who was experiencing occupational stress or burnout as being too sensitive or weak.
Strongly disagree
Disagree
Somewhat disagree
Neither agree nor disagree
Somewhat agree
Agree
Strongly agree
1
2
3
4
5
6
7
- 12.
I would have reservations about working with a mental health professional who is experiencing difficulties with occupational stress or burnout.
Strongly disagree
Disagree
Somewhat disagree
Neither agree nor disagree
Somewhat agree
Agree
Strongly agree
1
2
3
4
5
6
7
- 13.
Most mental health professionals would agree that occupational stress or burnout is a state of mind that one should snap out of.
Strongly disagree | Disagree | Somewhat disagree | Neither agree nor disagree | Somewhat agree | Agree | Strongly agree |
|---|---|---|---|---|---|---|
1 | 2 | 3 | 4 | 5 | 6 | 7 |
Scoring
Perceived structural stigma: (Sum items 1*, 5*, 7, and 9)/4
Self stigma: (Sum items 3, 4, and 10)/3
Perceived other stigma: (Sum items 8, 11, and 13)/3
Personal stigma: (Sum items 2, 6, and 12)/3
*Items 1 and 5 should be reverse scored prior to summation
Rights and permissions
About this article

Cite this article
Clough, B.A., Hill, M., Delaney, M. et al. Development of a measure of stigma towards occupational stress for mental health professionals. Soc Psychiatry Psychiatr Epidemiol 55, 941–951 (2020). https://doi.org/10.1007/s00127-019-01820-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00127-019-01820-9