
Abstract
Purpose
Major depression is a leading cause of morbidity in military populations. However, due to a lack of longitudinal data, little is known about the rate at which military personnel experience the onset of new episodes of major depression. We used a new source of clinical and administrative data to estimate the incidence of major depression diagnoses in Canadian Armed Forces (CAF) personnel, and to compare incidence rates between demographic and occupational factors.
Methods
We extracted all data recorded in the electronic medical records of CAF Regular Force personnel, at every primary care and mental health clinical encounter since 2016. Using a 12-month lookback period, we linked data over time, and identified all patients with incident diagnoses of major depression. We then linked clinical data to CAF administrative records, and estimated incidence rates. We used multivariate Poisson regression to compare adjusted incidence rates between demographic and occupational factors.
Results
From January to December 2017, CAF Regular Force personnel were diagnosed with major depression at a rate of 29.2 new cases per 1000 person-years at risk. Female sex, age 30 years and older, and non-officer ranks were associated with significantly higher incidence rates.
Conclusions
We completed the largest study to date on diagnoses of major depression in the Canadian military, and have provided the first estimates of incidence rates in CAF personnel. Our results can inform future mental health resource allocation, and ongoing major depression prevention efforts within the Canadian Armed Forces and other military organizations.
Similar content being viewed by others


Explore related subjects
Find the latest articles, discoveries, and news in related topics.Avoid common mistakes on your manuscript.
Introduction
Major depression is a recurring disorder that disproportionately affects military personnel. In Australia, Canada, the United Kingdom, and the United States, the prevalence of major depression in military personnel is at least twice that in comparable civilian populations [1,2,3,4]. Depressed soldiers are at increased risk of suicidal behaviors [5] poor job performance and absenteeism [6], and early separation from the military [7]. Because of its high prevalence and deleterious impact, major depression is a public health concern for military organizations. Epidemiological data are, therefore, needed to inform depression prevention strategies, and optimize the allocation of military mental health resources.
Until now, cross-sectional surveys have been the main source of epidemiological data on major depression in military personnel. These surveys have provided valuable information on the prevalence of major depression across different military organizations [1, 3, 8]. They have also shed new light on the occupational factors associated with major depression in military personnel [9] and on stigma perceptions [10] and care-seeking behaviors [11] related to this condition. However, cross-sectional surveys cannot provide information on the rate of major depression incidence.
Incidence rates are an important mental health indicator [12], particularly in open occupational cohorts such as an active military force. Military organizations must ensure that sufficient clinical resources are available to meet the mental health needs of their personnel. But mental health needs at the population level may change over time. New personnel are enlisted, currently serving personnel are exposed to occupational stressors, and other personnel release from military service. These factors can alter the population-level risks of mental disorder onset. Incidence rate estimates are needed to better forecast the future mental healthcare needs of military populations. However, due to a historical lack of longitudinal data, the incidence rate of major depression remains unknown for the military organizations of multiple nations.
Fortunately, recent developments in the Canadian Armed Forces (CAF) electronic medical record system have created new opportunities to fill this information gap. Since January 2016, all mental health assessments and treatments provided at CAF clinics have been documented using standardized electronic notes by the attending clinician. That clinician can be a psychiatrist, psychologist, social worker, counselor, nurse, or primary care physician. To estimate the rate of depression in the CAF, we had to develop and validate a customized algorithm to identify incident major depression diagnoses using the standardized electronic notes.
The primary objective of our study was to estimate the rate of major depression diagnoses in CAF personnel using data extracted from these electronic notes. However, current guidelines recommend assessing the quality of such data, when they are used for epidemiological research [13]. As a secondary objective, we, therefore, assessed the quality of our data by comparing our results to those of a recent cross-sectional study of self-reported mental health service utilization in a large representative sample CAF personnel with major depression [11]. This cross-sectional survey and our current study both measured similar outcomes in the same population; close agreement between their results would, therefore, support the validity of data used in the current study.
Methods
Study population
This study included all individuals who served in the CAF Regular Force between January and December 2017. Regular Force personnel are full-time soldiers who receive complete health coverage from the Canadian Forces Health Services. We excluded all CAF Reservists (who are mostly part-time soldiers) because they largely receive primary and specialty mental health care from the civilian sector. CAF electronic medical records would, therefore, have been at high risk of underestimating the mental health care utilization of Reservists.
CAF mental health care
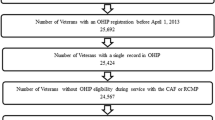
The Canadian Forces Health Services provide a comprehensive system of outpatient mental health care. Depressed patients may be assessed and treated in CAF primary care or specialty mental health clinics. They may also be referred to a civilian specialist in the surrounding community, if timely specialty care is not available at their local CAF clinic (Fig. 1).

Data elements generated in the electronic medical records of patients as they flow through the CAF system of outpatient mental health care
Clinical data
Whenever patients visit a CAF primary care or specialty mental health clinic, their care provider must complete an electronic note. CAF physicians, psychologists, and psychiatrists must record at least one diagnosis to complete their assessment and treatment notes (Fig. 1). Diagnoses are recorded using International Classification of Diseases (ICD-10) or Diagnostic and Statistical Manual of Mental Disorders (DSM-5) codes. CAF providers who do not have the professional authority to assign formal diagnoses (e.g., triage nurses, social workers, etc.) must record at least one symptom to complete their notes (Fig. 1). These symptoms are selected from a drop-down list of standardized clinical impressions.
External specialists do not have access to CAF electronic medical records. But to be reimbursed for services provided to externally referred patients, external specialists must send a paper copy of their clinical notes to the local CAF clinic. These notes are then scanned into the CAF electronic medical records of externally referred patients. A CAF healthcare provider—usually a nurse or social worker by training—periodically reviews the clinical progress of externally referred patients by completing an electronic note. External Provider Review notes are part of the CAF electronic medical record, and must contain at least one symptom code (Fig. 1).
Case definition
We sought to identify all personnel with an incident diagnosis of major depression, from January to December 2017. To do so, we extracted all diagnostic and symptom codes entered in CAF electronic medical records between January 2016 and June 2018.
We considered that personnel with at least one diagnostic code for major depressive episode (F32.x) or major depressive disorder (F33.x) in their electronic medical records were patients with major depression, irrespective of co-morbid psychiatric conditions. For all patients with major depression, we identified all clinical encounters related to major depression care as either: (1) clinical visits during which a diagnostic code for major depression was recorded, or (2) clinical visits that occurred within 6 months of a major depression diagnosis, and during which a code for “depressive symptoms” was recorded. Consistent with other studies [14,15,16], incident diagnoses were defined as the first clinical encounter for major depression in a 12-month period. With data available from January 2016 to June 2018, and with the case definition presented above, we were able to report on incident diagnoses from January to December 2017.
Patients with major depression who are exclusively assessed and treated by external specialists may never generate a depression code in CAF electronic medical records (Fig. 1). We, therefore, reviewed the scanned clinical notes of all externally referred patients with a “depressive symptom” code recorded on an External Provider Review note between January 2016 and June 2018 (n = 444); we, thus, identified an additional 116 patients who had been diagnosed with major depression over this time period. For these 116 patients, the incidence date was defined as the first encounter with the external specialist.
Demographic data
CAF administrative databases were used to determine the sex, age, rank, military unit, military trade, and duration of enlistment, for all CAF Regular Force personnel, from January to December 2017. Age was categorized into four groups: (a) 18–29 years, (b) 30–39 years, (c) 40–49 years, and (d) 50–60 years. Ranks were dichotomized as Non-Commissioned Members (NCM) and Officers.
Occupational data
Military units were linked to one of the six commands: (a) the Canadian Army, (b) the Royal Canadian Air Force, (c) the Royal Canadian Navy, (d) Military Personnel Command, (e) Joint and Special Forces, and (f) other central agencies. Military Personnel Command includes Joint Personnel Support Units (JPSU) that are administrative cells where ill or injured personnel from any command may be posted, if a medical condition precludes them from performing regular duties for a period of at least 6 months. JPSU personnel are expected to have much higher morbidity than other members of Military Personnel Command; we, therefore, reported on their incidence rates separately.
Military trades were linked to one of the ten occupational groups, as outlined on the CAF recruitment website (www.forces.ca): (a) technicians, (b) combat specialists, (c) administration and support, (d) engineers, (e) telecommunications, (f) air and ship crew, (g) health care, (h) sensor and radar, (i) public protection, including military police and firefighters, and (g) other.
Statistical analyses
For the estimation of incidence rates, we excluded all Regular Force personnel with any clinical encounter for major depression from January to December 2016. We then computed population-level counts of person-years at risk of an incident major depression diagnosis in remaining Regular Force personnel, from January to December 2017. We calculated the incidence of new major depression diagnoses per person-years at risk. We treated demographic categories (i.e., age group, rank category, command, and occupational group) as time-varying covariates, and used multivariate Poisson regression models to compare incidence rates across patient characteristics, adjusting for sex, age, and rank. We entered the log of person-years at risk as an offset in all multivariate Poisson analyses.
All analyses were performed using Stata, version 14.0 [17].
Secondary analysis: assessment of data source agreement
As recommended in current guidelines [13], we also sought to assess the validity of our case definition. Data source agreement is an accepted method for assessing the quality of case definitions in health administrative data research [18], and a large cross-sectional survey recently estimated that 6.0% of Regular Force personnel with major depression used mental health services in the previous year [11]. In an effort to assess the quality of data used in the current study, we identified all individuals who were serving in the Regular Force on the last day of our study period (i.e., December 31st 2017), and used our case definition to determine whether they had any clinical encounters for major depression at any point from January to December 2017. We qualitatively compared the sex and age distribution of patients with past-year clinical encounters for major depression to the results of the aforementioned survey [11].
Ethical considerations
The study was approved by the CAF Director of Force Health Protection, the CAF Director of Mental Health, and the University of Ottawa Office of Research Ethics and Integrity.
Results
A total of 72,054 individuals served in the CAF Regular Force at some point in 2017. We excluded 3638 (5.1%) of these individuals from our study because they had at least one diagnosis of major depression recorded in the 12 months preceding the study start date. The remaining 68,416 individuals contributed 61,997 service-years at risk of an incident major depression diagnosis during the study period; most of this person-time was contributed by males (86.0%) under the age of 40 years (69.5%) (Table 1).
During the study period, 1812 incident diagnoses of major depression were observed. Regular Force personnel were diagnosed at a rate of 29.2 new cases per 1000 person-years at risk (95% CI 27.9, 30.6). Female sex, age 30 years and older, and non-officer ranks were associated with higher incidence rates. After adjusting for demographic differences, technicians, and air and ship crewmembers, had significantly lower incidence rates than combat specialists. Adjusted rates were also lower in the Air Force than in the Army. Individuals posted to Joint Personnel Support Units, who were already ill or injured, were nearly three times more likely to have an incident diagnosis of major depression, compared to Army personnel of the same sex, age, and rank (Table 2).
For our secondary analysis, we identified all 66,605 individuals who were serving in the Regular Force on the last day of the 12-month study period. Using the case definition developed for our study, we estimated that 5.6% (95% CI 5.4%, 5.8%) of these individuals had a clinical encounter for major depression diagnosis at some point in the previous 12 months. Among these patients, 24.5% (95% CI 23.1, 25.9) were females, and 18.5% (95% CI 17.3%, 19.8%) were under the age of 30 years (Table 3). These results can be compared to those of a recent cross-sectional survey (see discussion below).
Discussion
This paper presents the most comprehensive examination to date of major depression incidence in serving CAF Regular Force personnel. We found that major depression amongst CAF personnel was diagnosed at a rate of 29.2 new cases per 1000 person-years of service, and that this rate varied considerably across demographic and organizational characteristics.
The overall incidence rate reported in this study is somewhat higher than that observed in the US Armed Forces, where 24.2 new cases of depressive disorders are diagnosed per 1000 person-years [19]. Several factors may account for this difference. First, CAF personnel suffering from major depression may be more likely to seek care than their American counterparts, and may, therefore, be more likely to receive a formal diagnosis; previous studies have found that 75% of depressed Canadian soldiers access mental health care in a 12-month period [11], compared to less than 50% in the US military [20,21,22]. This apparent difference in care-seeking propensity may be partly explained by the substantial difference in age composition between the two militaries; on average, CAF personnel are older than their American counterparts [23, 24], and older age is associated with higher mental health service use in depressed patients [25]. Second, our case-finding algorithm was likely more inclusive than that used for the US military study. In fact, US Armed Forces researchers only considered major depression diagnoses if they were recorded in the first or second diagnostic position during medical encounters [19]. In contrast, we used any major depression diagnosis to identify incident cases in our study, even if these diagnoses were recorded along with several co-morbid conditions.
We found that female sex, age 30 years and older, and non-officer ranks were associated with higher incidence of major depression diagnoses. These findings largely mirror those of previous studies. Indeed, a large body of research has already shown that, compared to males, females are more likely to suffer from major depression [26], and are more likely to seek care when experiencing depressive symptoms [25]. It is, therefore, not surprising to find that females were more likely to be diagnosed with major depression, compared to their male counterparts. Similarly, non-officer rank [27] and older age [25] have also been associated with greater likelihood of seeking mental healthcare, when needed.
Until now, researchers have depended on data from either population surveys (e.g., [28]) or manual reviews of medical charts (e.g., [29]) to investigate mental health care utilization in CAF personnel, and have lacked the statistical power required to compare occupational groups with the level of granularity reported in our study. With our large sample size, we found that combat specialists had a greater incidence of major depression than technicians, and air and ship crewmembers. However, incidence rates in combat specialists were not significantly different than in numerous other non-combat trades. This finding has important implications. Although combat experiences are associated with a substantial increase in depression risk [30], they only account for a small proportion of the major depression burden observed in Canada’s military [31]. Similarly, most American soldiers who attempt suicide have never deployed [5]. Since the early 2000s, the CAF have improved access to mental health care, implemented mental health training programs across the organization, and provided post-deployment mental health screening to all personnel returning from an overseas deployment, irrespective of their specific occupations [32]. Our findings support this holistic strategy, in the context of major depression prevention.
After excluding Joint Personnel Support Units (JPSU, i.e., service centers where seriously ill or injured personnel are posted if a medical condition precludes them from performing regular military duties for a period of at least 6 months) from Military Personnel Command, we found no large difference in the incidence rate of major depression diagnoses between the six CAF commands. Of note, JPSU personnel were nearly three times more likely to be diagnosed with major depression compared to any other personnel, even after using a 12-month lookback period to exclude prevalent cases. This elevated incidence rate is, therefore, not a consequence of personnel with prevalent major depression diagnoses being transferred to a JPSU. Rather, our finding suggests that individuals are at particularly high risk of being newly diagnosed with major depression after being transferred to a JPSU. This could be explained by several factors. First, individuals who are posted to a JPSU without a prevalent major depression diagnosis must have another physical or mental health condition. These pre-existing conditions could be strong risk factors for major depression onset [33]. Second, individuals who are separating from the military on medical grounds are often posted to a JPSU, and may be more willing to disclose their depressive symptoms. Fear of negative career repercussions is commonly reported as a barrier to mental health care among military personnel [34], but that barrier is unlikely to impact individuals already in the process of releasing from military service. Third, the process of transitioning out of an operational unit and into a JPSU may represent a stressful life event for some individuals which may, therefore, increase their risk of major depression onset [35]. In any case, our findings suggest that military personnel posted to administrative units such as JPSUs may benefit from counseling and other enhanced mental health prevention efforts.
When used to assess past-year prevalence of clinical encounters related to major depression, our case definition produced results that were highly consistent with previous research on CAF personnel. Indeed, a large population-based survey conducted in 2013 found that 6.0% of all CAF Regular Force personnel had sought care for major depression in the previous 12 months [11]; this estimate is remarkably close to the 5.6% past-year prevalence of diagnosed major depression reported herein. The estimated age and sex distribution of diagnosed patients was also similar between studies. Such a high level of data source agreement supports the quality of our data, and the validity of the case definitions used in our study.
Our study had noteworthy limitations. First, not all depressed individuals seek care. In fact, a recent study found that only 75% of CAF Regular Force personnel who met diagnostic criteria for major depression at any point in the previous year had sought professional mental health care over the same time period [11]. While this treatment gap is much smaller than in other populations [36, 37], 25% of depressed personnel remain undiagnosed. Clinical data can only be used to identify major depression in care-seeking individuals. Our study, therefore, misclassified a substantial number of depressed patients, and underestimated the true incidence of major depression in the CAF Regular Force. While our results cannot be used to measure major depression morbidity in the Canadian military, they nonetheless reflect current mental health service utilization rates for this condition.
Second, we relied on diagnostic codes extracted from electronic medical records to identify depressed patients. Previous authors have argued that diagnostic codes can be inaccurate; psychiatrists may incorrectly code their patients’ diagnoses, and may also code only one of the several co-morbid conditions [38]. Depressed patients may, therefore, not generate a diagnostic code for major depression every time they encounter a health professional. We mitigated this risk of misclassification bias by creating a case-finding algorithm, and linking data elements over time. Although we did not validate our case-finding algorithm against a gold-standard measure of major depression, our estimates of past-year treatment prevalence were highly consistent with those obtained from a 2013 population-based survey [11], as discussed above. As already noted, data source agreement is an accepted method for assessing the quality of case-finding algorithms using routinely collected data sources [18].
Despite the limitations listed above, we completed the largest study to date on major depression diagnoses in the Canadian military, and provided the first estimates of incident rates in CAF personnel. Our results have highlighted that the rates of major depression diagnoses vary substantially across sex, age, and rank categories, but are very similar between combat and non-combat trades. Our findings make an important contribution to military population health surveillance, and may be used by military organizations to better prepare for their future mental healthcare needs. For example, our estimated incidence rates could be used in predictive models to forecast the expected number of new major depression cases in a military population, given the age, sex, and occupational profile of its personnel. Furthermore, our study clearly demonstrated the feasibility of using electronic medical records as a powerful tool to study the incidence of mental disorder diagnoses in military populations.
References
Mcfarlane A, Sriapada R, Ganoczy D, et al (2011) Mental health in the Australian Defence Force: 2010 ADF mental health and wellbeing study: Full report. Canberra
Rusu C, Zamorski MA, Boulos D, Garber BG (2016) Prevalence comparison of past-year mental disorders and suicidal behaviours in the Canadian Armed Forces and the Canadian General Population. Can J Psychiatry 61:46S–55S. https://doi.org/10.1177/0706743716628856
Goodwin L, Wessely S, Hotopf M et al (2015) Are common mental disorders more prevalent in the UK serving military compared to the general working population? Psychol Med 45:1881–1891. https://doi.org/10.1017/S0033291714002980
Gadermann AM, Engel CC, Naifeh JA et al (2012) Prevalence of DSM-IV major depression among U.S. military personnel: meta-analysis and simulation. Mil Med 177:47–59
Ursano RJ, Kessler RC, Stein MB et al (2016) Risk factors, methods, and timing of suicide attempts among US Army Soldiers. JAMA psychiatry 73:741–749. https://doi.org/10.1001/jamapsychiatry.2016.0600
Pflanz SE, Ogle AD (2006) Job stress, depression, work performance, and perceptions of supervisors in military personnel. Mil Med 171:861–865. https://doi.org/10.7205/MILMED.171.9.861
Littman AJ, Jacobson IG, Boyko EJ et al (2013) Weight change following US military service. Int J Obes 37:244–253. https://doi.org/10.1038/ijo.2012.46
Zamorski MA, Bennett RE, Rusu C et al (2016) Prevalence of past-year mental disorders in the Canadian Armed Forces, 2002-2013. Can J Psychiatry 61:26S–35S. https://doi.org/10.1177/0706743716628854
Nelson C, Cyr KS, Corbett B et al (2011) Predictors of posttraumatic stress disorder, depression, and suicidal ideation among Canadian Forces personnel in a National Canadian Military Health Survey. J Psychiatr Res 45:1483–1488. https://doi.org/10.1016/j.jpsychires.2011.06.014
Weeks M, Zamorski MA, Rusu C, Colman I (2017) Mental illness-related stigma in Canadian military and civilian populations: a comparison using population health survey data. Psychiatr Serv 68:710–716. https://doi.org/10.1176/appi.ps.201600398
Thériault FL, Garber BG, Momoli F et al (2019) Mental Health Service utilization in depressed Canadian armed forces personnel. Can J Psychiatry 64:59–67. https://doi.org/10.1177/0706743718787792
Tannenbaum C, Lexchin J, Tamblyn R, Romans S (2009) Indicators for measuring mental health: towards better surveillance. Healthc Policy 5:e177–e186
Benchimol EI, Smeeth L, Guttmann A et al (2015) The REporting of studies Conducted using Observational Routinely-collected health Data (RECORD) Statement. PLoS Med. https://doi.org/10.1371/JOURNAL.PMED.1001885
Spettell CM, Wall TC, Allison J et al (2003) Identifying physician-recognized depression from administrative data: consequences for quality measurement. Health Serv Res 38:1081–1102
Yoon G, Petrakis IL, Rosenheck RA (2015) Correlates of major depressive disorder with and without comorbid alcohol use disorder nationally in the veterans health administration. Am J Addict 24:419–426. https://doi.org/10.1111/ajad.12219
Shrestha A, Cornum BGR, Vie LL et al (2018) Protective effects of psychological strengths against psychiatric disorders among soldiers. Mil Med 183:386–395. https://doi.org/10.1093/milmed/usx189
StataCorp (2015) Stata Statistical Software: Release 14
Weiskopf NG, Weng C (2013) Methods and dimensions of electronic health record data quality assessment: enabling reuse for clinical research. J Am Med Inform Assoc 20:144–151. https://doi.org/10.1136/amiajnl-2011-000681
Stahlman S, Oetting AA (2018) Mental health disorders and mental health problems, active component, U.S. Armed Forces, 2007–2016. MSMR 25:2–11
Hoge CW, Castro CA, Messer SC et al (2004) Combat duty in Iraq and Afghanistan, mental health problems, and barriers to care. N Engl J Med 351:13–22. https://doi.org/10.1056/NEJMoa040603
Welsh MM, Federinko SP, Burnett DG et al (2014) Deployment-related depression screening, 2001-2008: comparing clinical versus research surveys. Am J Prev Med 47:531–540. https://doi.org/10.1016/j.amepre.2014.07.036
Morgan JK, Hourani L, Lane ME, Tueller S (2016) Help-seeking behaviors among active-duty military personnel: utilization of Chaplains and Other Mental Health Service Providers. J Health Care Chaplain 22:102–117. https://doi.org/10.1080/08854726.2016.1171598
Office of the Deputy Assistant Secretary of Defense for Military Community and Family Policy (2015) 2015 Demographics Profile of the Military Community
Thériault FL, Gabler K, Naicker K (2016) Health and lifestyle information survey of Canadian Armed Forces Personnel 2013/2014—Regular Forces Report. Department of National Defence, Ottawa, Canada
Twomey CD, Baldwin DS, Hopfe M, Cieza A (2015) A systematic review of the predictors of health service utilisation by adults with mental disorders in the UK. BMJ Open 5:e007575. https://doi.org/10.1136/bmjopen-2015-007575
Ferrari AJ, Somerville AJ, Baxter AJ et al (2013) Global variation in the prevalence and incidence of major depressive disorder: a systematic review of the epidemiological literature. Psychol Med 43:471–481. https://doi.org/10.1017/S0033291712001511
Hines LA, Goodwin L, Jones M et al (2014) Factors affecting help seeking for mental health problems after deployment to Iraq and Afghanistan. Psychiatr Serv 65:98–105. https://doi.org/10.1176/appi.ps.004972012
Fikretoglu D, Liu A, Pedlar D, Brunet A (2010) Patterns and predictors of treatment delay for mental disorders in a nationally representative, active Canadian military sample. Med Care 48:10–17. https://doi.org/10.1097/MLR.0b013e3181bd4bf9
Boulos D, Zamorski MA (2016) Delay to mental healthcare in a cohort of Canadian Armed Forces personnel with deployment-related mental disorders, 2002-2011: a retrospective cohort study. BMJ Open 6:e012384. https://doi.org/10.1136/bmjopen-2016-012384
Bonde JP, Utzon-Frank N, Bertelsen M et al (2016) Risk of depressive disorder following disasters and military deployment: systematic review with meta-analysis. Br J Psychiatry 208:330–336. https://doi.org/10.1192/bjp.bp.114.157859
Boulos D, Zamorski MA (2016) Contribution of the mission in Afghanistan to the burden of past-year mental disorders in Canadian Armed Forces Personnel, 2013. Can J Psychiatry 61:64S–76S. https://doi.org/10.1177/0706743716628857
Zamorski MA, Bennett RE, Boulos D et al (2016) The 2013 Canadian Forces Mental Health Survey. Can J Psychiatry 61:10S–25S. https://doi.org/10.1177/0706743716632731
Katon WJ (2011) Epidemiology and treatment of depression in patients with chronic medical illness. Dialogues Clin Neurosci 13:7–23
Hom MA, Stanley IH, Schneider ME, Joiner TE (2017) A systematic review of help-seeking and mental health service utilization among military service members. Clin Psychol Rev 53:59–78. https://doi.org/10.1016/j.cpr.2017.01.008
Kendler KS, Karkowski LM, Prescott CA (1999) Causal relationship between stressful life events and the onset of major depression. Am J Psychiatry 156:837–841. https://doi.org/10.1176/ajp.156.6.837
Mojtabai R, Olfson M (2006) Treatment Seeking for Depression in Canada and the United States. Psychiatr Serv 57:631–639. https://doi.org/10.1176/ps.2006.57.5.631
Quartana PJ, Wilk JE, Thomas JL et al (2014) Trends in mental health services utilization and stigma in US soldiers from 2002 to 2011. Am J Public Health 104:1671–1679. https://doi.org/10.2105/AJPH.2014.301971
Crumlish N, Kelly BD (2009) How psychiatrists think. Adv Psychiatr Treat 15:72–79. https://doi.org/10.1192/apt.bp.107.005298
Acknowledgements
The authors wish to thank the dedicated healthcare providers, business analysts, and programmers without whom data used for this study could not have been extracted from CAF electronic medical records. This research was undertaken, in part, thanks to funding from the Canada Research Chairs program for IC, and from the Surgeon General’s Health Research Program for FLT.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Thériault, F.L., Hawes, R.A., Garber, B.G. et al. Incidence of major depression diagnoses in the Canadian Armed Forces: longitudinal analysis of clinical and health administrative data. Soc Psychiatry Psychiatr Epidemiol 55, 581–588 (2020). https://doi.org/10.1007/s00127-019-01754-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00127-019-01754-2