
Abstract
Purpose
This study aimed at evaluating the comorbidity between DSM-IV obsessive compulsive disorder (OCD) and subthreshold forms and physical diseases in the general population as well as disability associated with comorbidity.
Methods
We used data from the 1998 German Mental Health Survey, a representative survey of the German population. Mental disorders and physical diseases of 4181 subjects (aged 18–65) were cross-sectionally assessed. Mental disorders were diagnosed using the M-CIDI/DIA-X interview. Physical diseases were assessed through a self-report questionnaire and a standardized medical interview. We created three groups of obsessive–compulsive symptoms: (1) no obsessive compulsive symptoms (n = 3,571); (2) obsessive compulsive symptoms (OCS, n = 371; endorsement of OCS (either obsession or compulsion) without fulfilling any core DSM-IV criteria); (3) subthreshold OCD/OCD (n = 239; fulfilling either some or all of the core DSM-IV criteria).
Results
In comparison to subjects without OCS, subjects with subthreshold OCD/OCD showed higher prevalence rates of migraine headaches (OR 1.7; 95 % CI 1.1–2.5) and respiratory diseases (OR 1.7; 95 % CI 1.03–2.7); subjects with OCS showed higher prevalence rates of allergies (OR 1.6; 95 % CI 1.1–2.8), migraine headaches (OR 1.9; 95 % CI 1.4–2.7) and thyroid disorders (OR 1.4; 95 % CI 1.01–2.0). Subjects with both OCS and physical disease reported the highest number of days of disability due to physical or psychological problems during the past 30 days compared to subjects with only OCS, only physical disease or neither of them.
Conclusions
OCD and subthreshold forms are associated with higher comorbidity rates with specific physical diseases and higher disability than subjects without OCS. Possible etiological pathways should be evaluated in future studies and clinicians in primary care should be aware of these associations.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
There is increasing evidence that mental disorders frequently co-occur with physical diseases [1–4]. Such comorbidity between mental and physical diseases has been found in patients diagnosed with schizophrenia, bipolar disorder, schizoaffective disorder and major depressive disorder [5]. Among these patients, nutritional and metabolic diseases, cardiovascular diseases, viral diseases, respiratory tract diseases, musculoskeletal diseases, pregnancy complications and stomatognathic diseases were found to be more prevalent than in the general population [1, 6, 7]. Due to their higher risk of cardiovascular diseases, patients with affective disorders are even known to be at high risk for premature death [4, 8].
There is evidence from patients and community-based studies that physical health problems are also associated with anxiety disorders [2, 3, 9, 10]. Significant associations between anxiety disorders and cardiac disorders, hypertension, gastrointestinal problems, genitourinary disorders and migraine have been found in patients recruited from treatment and community sources [2]. Additionally, increased rates of arthritis, asthma and ulcers were detected in patients with anxiety disorders [10]. Likewise, population surveys showed that depressive and anxiety disorders without comorbidity were associated in equal degree with physical conditions [3]. In addition, analyses revealed that the presence of an anxiety disorder was significantly associated with thyroid disease, respiratory disease, gastrointestinal disease, arthritis, migraine headaches and allergic conditions in the general population [9]. Even community samples across different countries showed that anxiety disorders occurred at higher rates in persons with heart diseases compared to those without heart disease [11]. Moreover, community analyses revealed that specific anxiety disorders are also significantly associated with medically explained pain symptoms, unexplained pain symptoms and pain disorder [12].
This mental-physical comorbidity has negative consequences for subjects’ disability in daily life. Subjects with comorbid physical and anxiety disorders are more likely to be severely disabled than subjects with either condition alone [9, 13, 14]. This may suggest that it should be ensured that subjects with mental-physical comorbidity receive enough clinical care in order to recognize and treat both disorders.
Additionally, cross-sectional analyses of the association of specific physical diseases with certain mental disorders can lead to hypotheses concerning etiological mechanisms at least in subgroups of affected subjects. For example, asthma has been found to be associated with panic disorder in many cross-sectional community-based studies [15]. These findings stimulated longitudinal studies to evaluate the role of smoking as an etiological factor in asthma and panic disorder [15]. This illustrates how hypotheses of certain etiological factors can be derived from cross-sectional associations of mental-physical comorbidity.
Based on the fact that several studies showed associations between many mental disorders and specific physical diseases, we will report for the first time the association of specific physical diseases and OCD and disability related to this comorbidity. This is important because epidemiological studies showed that across anxiety disorders obsessive compulsive disorder (OCD) was found to be the disorder with the highest estimate of the number of life years lost due to the disease in men and second highest in women behind panic disorder [16]. Increased health care utilization among individuals with OCD [17] and decreased physical wellbeing (referring to physical health, sleep and pain) in patients with OCD [18] were found. Additionally, one study revealed that the presence of any chronic physical condition increases the prevalence of obsessive–compulsive symptoms [19]. Furthermore, it is known that subthreshold types of OCD that do not fulfill all DSM-IV diagnostic criteria are more prevalent in the general population compared to OCD [20–22]. Adam et al. [17] could show that subjects with such “subthreshold” OCD (i.e. fulfilling some but not all core DSM-IV criteria) and obsessive compulsive symptoms (i.e. endorsement of stem questions without fulfilling any core DSM-IV criteria) report higher disability and increased health care utilization in the community than subjects without these symptoms.
To our knowledge no community study about the physical health problems of individuals with OCD and subthreshold forms has been published, even though subthreshold forms of OCD are known to be associated with comparable disability as full diagnostic OCD. As shown above, these analyses are relevant for implications of the health care system and to generate etiological hypotheses of OCD.
In this report we, therefore, evaluate the association between physical diseases and individuals with OCD and subthreshold forms in the general population and the disability associated with comorbidity. For this purpose we use representative community data from the German Health Interview and Examination Survey and its Mental Health Supplement.
Method
Design and sample
We used Data from the German Health Interview and Examination Survey and its Mental Health Supplement (GHS-MHS) conducted in 1997. The GHS was the first nationwide cross-sectional study for medical and social assessments in Germany and was commissioned by the German Ministry of Science, Research and Education and the Robert Koch Institute and authorized by the relevant institutional review board and ethics committee. The aim of the core study was the assessment of sociodemographic characteristics, physical diseases, impairments and healthcare utilization in a representative community sample of 7,124 subjects aged 18–79 (overall response rate 61.5 %). It was a stratified, randomized sample from 113 communities throughout Germany with 130 sampling units (sampling steps: (1) selection of communities, (2) selection of sampling units, (3) selection of inhabitants) [23, 24]. To handle the stratified sampling design the data were weighted and confidence intervals were calculated by the Huber-White sandwich method to account for the weighting scheme as well as the stratified sampling design [24].
For the assessment of mental disorders in the GHS-MHS, a two-stage design was used: The first stage entailed the administration of a 12-item screening questionnaire for mental disorders at the end of the medical examination of the core survey (CID-S) [25]. The second stage involved the administration of a structured psychopathological interview, the Munich Composite International Diagnostic Interview (DIA-X/M-CIDI), to all core survey subjects who had screened positive for a mental disorder and to a random sample of 50 % who screened negative [25]. This subsample of the GHS built the sample of the Mental Health Supplement and included 4,181 subjects aged 18–65 years. The conditional response rate (i.e., subjects who completed the M-CIDI interview) was 87.6 %. All subjects gave their informed consent. Further description of aims, design and methods as well as sociodemographic characteristics of the whole GHS-MHS sample can be found elsewhere [23].
Assessment of OCD
For the diagnostic assessments, a modified version of the fully structured interview DIA-X/M-CIDI was used [26]. The questions covered DSM-IV and ICD-10 criteria. The DIA-X interview enables the assessments of symptoms, syndromes and onset, duration and severity. The interview was conducted by trained psychologists and physicians [27]. The test–retest reliability for OCD was found to be excellent (k = 0.81) with an average time interval of 38 days between interviews in a sample of 60 subjects in the community. The validity of the DIA-X/M-CIDI OCD diagnoses compared to diagnoses from independent treating physicians in a sample of 68 randomly chosen patients was also excellent (k = 0.91). The sensitivity was 100 %, while the specificity was 98.4 % [17, 28].
The DIA-X/M-CIDI module for OCD includes two parts: one for the assessment of obsessions and one for the assessment of compulsions. In each part, stem questions are asked at the beginning. In the obsession section the stem question refers to a wide range of potential thoughts and cognitions presented in the form of a symptom list: “During the last 12 month, have you been bothered by having certain unpleasant thoughts or images like recurrent arbitrary thoughts, such as the idea that your hands are dirty or have germs on them?” (yes or no). In the compulsion section three stem questions are asked to assess repetitive behaviors (“doing something like washing hands over and over again (yes or no) or “checking several times whether the door is locked” (yes or no) or mental acts (“counting something like tiles in a floor” (yes or no)). If the subject approves one of these stem questions, they are subsequently asked for the mandatory DSM-IV criteria. The DSM-IV mandatory criteria include criteria A for the diagnostic details of obsessions and compulsions, criteria B for the recognition that the obsessions or compulsions are excessive or unreasonable and C for the evaluation if the disorder causes distress or dysfunction. Diagnostic criteria refer to the past 12 months.
To facilitate comparisons with prior work [17], this paper splits the sample into the following three mutually exclusive groups:
-
1.
Subthreshold OCD/OCD (either (a) subthreshold OCD: the subject affirmed at least one of the stem questions for obsessive or compulsive symptoms and fulfilled at least one of the DSM-IV diagnostic criteria A, B or C, but not the full DSM-IV criteria, or (b) OCD: the subject met full DSM-IV criteria A, B and C for OCD)
-
2.
OCS (the subject affirmed at least one of the stem questions for obsessive or compulsive symptoms, but did not fulfill any of the DSM-IV criteria A, B or C)
-
3.
No OCS (the subject did not affirm any of the stem questions for obsessions or compulsions)
Due to the small group size of full diagnostic OCD (see Table 1) and the small cell sizes when combined with physical diseases, we merged the groups OCD and subthreshold OCD (group 1) in contrast to Adam et al. [17].
Assessment of physical conditions
In the GHS, physical conditions were assessed by a self-report questionnaire and a standardized computer-assisted medical interview by a general practice physician.
Based on the information on physical diseases in the self-report questionnaire, the physicians conducted information about lifetime prevalences, 12-month prevalences and point prevalences (4 weeks) of 44 physical diseases [23].
Additionally anthropometric and blood pressure measurements were conducted as well as blood and urine samples. Based on these laboratory analyses diagnoses were then supplemented and revised [23]. The following analyses are based on the physicians’ diagnoses during the medical interview. We, therefore, grouped the disorders into eleven groups of disorders (see Table 1).
Assessment of disability
Disability was assessed by asking the subjects whether he or she was completely or partially unable to carry out daily activities (i.e., function in work, in school or in family), because of psychological problems in the 4 weeks before the interview took place (yes or no) and whether he or she was completely or partially unable to carry out daily activities (function in work, in school or in family), because of physical problems in the 4 weeks before the interview took place (yes or no).
Sociodemographic correlates
For the present sample, earlier analyses revealed no associations between OCS, subthreshold OCD, OCD and gender, employment status and social class [17]. Significant associations between age and subthreshold OCD and OCS were found: the 12-month prevalence was lower in the older age group. Additionally, the 12-month prevalence of OCS was higher in the separated, divorced or widowed subjects group. More details can be seen elsewhere [17].
Statistical analyses
Comorbidity between OCS and physical diseases
We used logistic regression [odds ratio (OR) with 95 % confidence intervals (CI)] to examine associations between the groups OCS and subthreshold OCD/OCD and physical diseases. We considered a p value <0.05 as statistically significant. For the logistic regression analyses we used the STATA software package, version 11.0 [29].
Disability
To analyze the association between OCS and physical disease on the risk of physical or psychological disability we used the two factors OCS (combining both OCS groups) and physical disease (which includes any of the physical diseases), both having two levels (yes or no). To determine whether comorbidity of OCS and physical disease were associated with an increased likelihood of past 30-day disability due to physical or psychological problems, we considered the zero inflated negative binomial model and the Hurdle model as these models account for excessive zeros (85.8 % of subjects reported 0 days of disability due to physical problems and 98.7 % of subjects reported 0 days of disability due to psychological problems). These two models led to almost identical results and fitted the data equally well (based on the Akaike information criterion, AIC). We chose the Hurdle model because we think that its underlying process is somewhat more comprehensible compared with the zero inflated negative binomial model. The hurdle model (OR with 95 % CI and incidence risk ratio (IRR) with 95 % CI) assumes negative binomial (physical disability) or Poisson (psychological disability) distributed outcomes. This model accounts not only for the excessive number of zeros observed, but also for overdispersion (i.e. the fact that the observed variability in the outcome was higher than its mean, see e.g. [30]). Hurdle models consist of two parts. In the first part, a binomial model is used to model the probability of zeros versus non-zeros. In the second part that deals with the non-zero counts and which is hence often called the “count model”, a Poisson or a negative binomial model is used (depending on whether the counts are over dispersed or not). As only non-zero values are considered in this second part, this model is zero-truncated [31].
Our model contained the two factors OCS and physical disease plus the interaction between the two. For both factors we were thus able to test (1) whether they had an impact on the probability of physical or psychological disability and (2) whether they affected the number of days of disability among those subjects who have reported at least 1 day of disability. The interaction thereby tested whether subjects having both OCS and physical disease were (1) at a particularly high risk of physical or psychological impairment and (2) if so, how strongly. For calculating the hurdle model we used the software MPlus (version 6) [32].
To check for biological interaction as described by Rothman [33], i.e. whether the combined effect of both factors OCS and physical disease is larger than the sum of the individual effects of these two factors, denoting deviation from additivity in disease risks, we additionally calculated the relative excess risk due to interaction (RERI), the attributable proportion due to interaction (AP) and the synergy index (S) [34], using the software R (version 2.14) [35]. Absence of biological interaction thereby suggests independence of OCS and physical disease as risk factors of disability.
Results
12-month prevalence
The 12-month prevalence rate was 8.3 % for OCS, and 5.2 % for the combined OCD and subthreshold OCD (Table 1). Among physical diseases, the highest 12-month prevalence rate was detected for arthritic conditions (25.9 %), the lowest for neurological diseases (0.5 %).
Associations of physical diseases and OCS, subthreshold OCD/OCD
Significantly higher prevalence rates in subjects with OCS were found for allergies (OR 1.6; 95 % CI 1.1–2.8), migraine (OR 1.9; 95 % CI 1.4–2.7) and thyroid diseases (OR 1.4; 95 % CI 1.01–2.0) compared to the no OCS group (see Table 2).
The subthreshold OCD/OCD group was associated with elevated odds for respiratory diseases (OR 1.7; 95 % CI 1.03–2.7) and migraine (OR 1.7; 95 % CI 1.1–2.5).
Disability
Disability due to physical problems
We used the two factors OCS (combining both OCS groups) and physical disease (which includes any of the physical diseases) to analyze the association with disability. As there was no indication of statistical interaction between the two factors for both the binomial (p = 0.40) and the count model parts (p = 0.77), we reran the model without interaction. The binomial part of the model revealed that both OCS and physical disease significantly increased the probability of disability (OCS: OR 1.9; 95 % CI 1.4–2.5, p < 0.001; physical disease: OR 1.7; 95 % CI 1.2–2.2, p < 0.001). The count model part of the model showed that physical disease significantly increased the number of days of disability (IRR 1.6; 95 % CI 1.1–2.2, p = 0.008), whereas OCS did not (IRR 1.3; 95 % CI 0.9–1.8, p = 0.064).
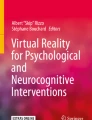
As shown in Fig. 1, the highest number of days of disability due to physical diseases was reported by subjects with both OCS and physical disease (n = 95 (2.74 %), M 2.33; 95 % CI 1.61–3.05), followed by subjects with OCS only (M 1.10; 95 % CI 0.64–1.55) and by subjects with physical disease only (M 1.09; 95 % CI 0.86–1.34). Subjects with neither OCS nor physical disease indicated the lowest number of days of disability (M 0.50; 95 % CI 0.3–0.7). There was no indication for the presence of biological interaction for any of the three measures (SI, RERI, AP; p > 0.05 in each case).

Mean days of disability during past 30 days. OCS obsessive compulsive symptoms; Error bars indicate standard errors
Disability due to psychological problems
As there was no indication of statistical interaction between the two factors for both the binomial (p = 0.24) and the count model parts (p = 0.74) in the disability due to psychological problems, we again reran the model without the interaction. The binomial part of the model revealed that both OCS and physical disease significantly increased the probability of disability (OCS: OR 3.8; 95 % CI 2.1–6.9, p < 0.01; physical disease: OR 3.7; 95 % CI 1.4–9.8, p < 0.01). Contrary to the disability due to physical problems, the count model part of the model revealed that there was no significant effect of both factors on the number of days of disability due to psychological problems (p > 0.55 for both model parts).
As for disability due to physical problems, the highest number of days of disability due to psychological problems was reported by subjects with both OCS and physical disease (n = 19 (0.55 %), M 0.47; 95 % CI 0.17–0.76), followed by subjects with OCS only (M 0.14; 95 % CI 0.03–0.31) and by subjects with physical disease only (M 0.10; 95 % CI 0.05–0.16). Subjects with neither OCS nor physical disease indicated the lowest number of disability days (M 0.03; 95 % CI 0.00–0.06; Fig. 1). Again, no indication for biological interaction was found for any of the three measures (SI, RERI, AP; p > 0.05 in each case).
Discussion
To the best of our knowledge, this is the first study that analyses the association between OCD and subthreshold forms and physical diseases in a representative community sample.
Our results show that obsessive compulsive symptoms are associated with higher prevalence rates of specific physical diseases in the general population. These results add to the body of literature on the comorbidity of physical diseases and other anxiety disorders. In comparison to findings from other anxiety disorders, we found associations with migraine headaches, allergies and thyroid diseases in OCS and significant associations with respiratory diseases and migraine headaches in subthreshold OCD/OCD [2, 9, 10]. Further, our analyses revealed that subjects with both OCS and physical disease report the highest number of days of disability compared to subjects having only OCS (without physical disease), only a physical disease or neither of them.
Different models exist to explain the cooccurrence of anxiety disorders and physical diseases: anxiety as consequent or antecedent factor of a physical disease, third variables that lead to the comorbidity or, common genetic, environmental or personality factors that contribute to the cooccurrence [9]. Even though only few specific hints for the explanations of associations between OCS and physical diseases exist, these hints can point towards important etiological pathways in subgroups of OCD patients and, therefore, will be discussed in the following.
First, defects in serotonin metabolism as possible neurochemical basis of both migraine and OCD have been proposed [36]. An abnormal serotonin function in subjects with OCD is one of the most consistent pathophysiologic findings [37]. Similarly, serotonin abnormalities have been implicated in the pathogenesis of migraine [36, 38]. Alternatively it has been proposed that anxiety disorders may be involved in peripheral and central mechanisms of pain sensitization which contributes to the evolution of chronic headaches [39]. Against this background, our results can support a suggested role of serotonin in an etiological pathway of OCD.
Second, an increased rate of immune-related symptoms among OCD patients has been reported [40]. As a possible explanation, one theory suggests that postinfectious autoimmune responses might be associated with the development of pediatric OCD, which leads to an increased rate of immune-related diseases in adults with OCD [40]. Our cross-sectional results match with this theory, as we found increased rates of allergies in subjects with OCS. Studies showed that especially immune responses to streptococcal infections may be relevant for the etiology of OCD [41]. Our analyses support a suggested involvement of immune responses that may be relevant in the etiology of a subgroup of OCD.
Third, the association between asthma and anxiety disorders, especially in panic disorder, is well established [42, 43]. Explanations range from hyperventilation that is commonly associated with anxiety disorders, subjective psychological disturbance which could lead to enhanced bronchoconstriction to biological effects of anxiety on immunological or biological factors [44]. Specific explanations of the association between OCD and respiratory diseases lack, however. Therefore, we can only speculate that comparable to other anxiety disorders, subjects with OCD could have an altered symptom perception leading to enhanced awareness of breathlessness and bronchoconstriction and therefore to asthma-like symptoms. Despite that no specific explanation for this association exists, our results nevertheless show that an involvement of the respiratory tract may be important in OCD.
Fourth, pervasive evidence documents the relationship between thyroid diseases and mental symptoms such as impairment of cognitive functions or behavioral and mood disturbances [45, 46]. Concerning OCD, some observations of increased rates of obsessive–compulsive symptoms in subjects with thyroid disease have been found [46]. As an explanation, common biochemical abnormalities that play a role for both thyroid diseases and OCD may exist [46]. A diminished thyrotropin releasing hormone (TRH) response to a TRH stimulation was detected in subjects with OCD, also [47] suggesting an alteration in the serotonergic system, as a decreased central serotonergic activity is associated with blunted TSH response [47]. The increased rates of thyroid diseases in our analyses support the hypothesis of an alteration of the hypothalamic-pituitary-thyroid axis in the pathophysiology of OCD, too.
Fifth, it could be suggested that certain behaviors that occur in OCD increase the vulnerability to develop a physical disease. As a lack of exercise has been associated with anxiety disorders [48] and physical inactivity is associated with many chronic physical diseases such as cardiovascular diseases or diabetes [49], it could be suggested that subjects with OCD are at increased risk to develop physical illnesses through physical inactivity. Further, it has been shown that cleaning activities related to exposure to certain cleaning products in the household are associated with asthma [50]. Extensive hand washing or cleaning can be a symptom of OCD. Through exposure to poisonous cleaning agents this could lead to higher prevalence of respiratory diseases in subjects with OCD. Additionally, subjects with OCD avoid uncertainty [51]. This might in addition be related to an increased prevalence of physical diseases in these subjects, as isolation and, therefore, a lack of exercise may be the consequences.
Given these etiological considerations, our results may be useful to deduce hypotheses concerning the involvement of certain physiological factors in the etiology of OCD in subgroups of subjects. Future studies are clearly needed to replicate these findings.
As some physical diseases were only associated with OCS and not OCD (higher prevalence of allergies and thyroid diseases only in OCS) or vice versa, it is possible that different etiological factors are related to OCS, subthreshold OCD and OCD. Future studies should, therefore, not only include OCD but also subthreshold forms to test these hypotheses.
Besides the documentation of the associations between physical diseases and OCS and the deduction of potential etiological hypotheses, our analyses show that both subjects with OCS or physical diseases have an increased probability of disability due to psychological or physical problems during the past 30 days. Comparable to previous studies on anxiety disorders [9] or mental disorders in general [13] and physical diseases, the highest number of days of disability was reported in the group with both OCS and physical diseases. This is supported by previous findings that subjects with both mental and physical conditions are more likely to be severely disabled than those with either condition alone [13].
Due to the fact that no indication for biological interaction was found between OCS and physical disease, the increased disability of subjects affected by both OCS and physical disease may be seen as an additive rather than a synergistic effect of both disorders.
The mechanisms leading to this specific increased disability are unknown. Research on other anxiety disorders, however, suggest that anxiety is associated with poor adherence to self-care regimen and increased medical complications in patients with chronic medical illness [52]. This could lead to decreased active behavioral self-management strategies and, therefore, to an increased burden of the physical disease in anxiety in general [53] and specifically in OCD.
The increased disability in subjects with both OCS and physical disease may reflect an increased need of recognition and treatment of both physical disorder and OCS in primary health care. Future studies could additionally investigate whether this comorbidity is associated with a loss in quality of life.
The current study has a number of limitations. First, the survey is limited to subjects aged 18–65 years, which does not enable generalization of the results to younger or older subjects. Second, as already mentioned by Sareen et al. [9], even though physicians’ diagnoses were used, certain diagnoses are more reliant on self-report data (e.g. arthritis) than others (e.g. diabetes). That may have led to over reporting of physical symptoms in anxious patients. Third, due to the cross-sectional nature of the study, it is not possible to draw conclusions about the causal nature of the associations between OCD or OCS and physical diseases. Fourth, although we used a large representative sample with 4,181 subjects, the sample size of full diagnostic OCD is rather small (n = 38). In addition, the combinations between OCD symptoms and physical diseases led to small cell sizes (especially in cardiac diseases, diabetes and neurological diseases). Fifth, it has to be considered that comorbidity between OCD and subthreshold forms and other mental disorders has been reported [17]. Thus, further investigation is needed to examine specificity of the results.
With these limitations in mind, our community study shows that subjects affected by DSM-IV obsessive compulsive disorder either on the full/subthreshold or even on the symptomatic level report higher rates of certain physical diseases than subjects without these symptoms. This comorbidity is associated with higher impairment than either condition alone.
These findings can be helpful to detect new etiological pathways underlying OCD in subgroups of affected subjects or support the ones suggested in earlier studies. In addition, clinicians and doctors in primary care need to be sensibilized for these associations to recognize and treat both physical disease and OCS to reduce disability in affected subjects.
Abbreviations
- OCD:
-
Obsessive compulsive disorder
- OCS:
-
Obsessive compulsive symptoms
- GHS-MHS:
-
German health interview and examination survey and its mental health supplement
- DIA-X/M-CIDI:
-
The Munich composite international diagnostic interview
- DSM-IV:
-
Diagnostic and statistical manual of mental disorders, Fourth Edition
- ICD-10:
-
International classification of diseases, Tenth Edition
- CI:
-
Confidence interval
- OR:
-
Odds ratio
- IRR:
-
Incidence risk ratio
- RERI:
-
Relative excess risk due to interaction
- AP:
-
The attributable proportion due to interaction
- S:
-
Synergy index
References
De Hert M, Dekker JM, Wood D, Kahl KG, Holt RI, Moller HJ (2009) Cardiovascular disease and diabetes in people with severe mental illness position statement from the European Psychiatric Association (EPA), supported by the European Association for the Study of Diabetes (EASD) and the European Society of Cardiology (ESC). Eur Psychiatry 24(6):412–424. doi:10.1016/j.eurpsy.2009.01.005
Harter MC, Conway KP, Merikangas KR (2003) Associations between anxiety disorders and physical illness. Eur Arch Psychiatry Clin Neurosci 253(6):313–320
Scott K, Bruffaerts R, Tsang A, Ormel J, Alonso J, Angermeyer M, Benjet C, Bromet E, De Girolamo G, De Graaf R, Gasquet I, Gureje O, Haro JM, He Y, Kessler RC, Levinson D, Mneimneh ZN, Oakley Browne MA, Posada-Villa J, Stein DJ, Takeshima T, Von Korff M (2007) Depression-anxiety relationships with chronic physical conditions: results from the World Mental Health Surveys. J Affect Disord 103:113–120
Shimoda H, Kawakami N, Tsuchiya M (2012) Epidemiology of psychiatric disorders among medically ill patients. Nihon Rinsho 70(1):7–13
De Hert M, Correll CU, Bobes J, Cetkovich-Bakmas M, Cohen D, Asai I, Detraux J, Gautam S, Moeller HJ, Ndetei DM, Newcomer JW, Uwakwe R, Leucht S (2011) Physical illness in patients with severe mental disorders. I. Prevalence, impact of medications and disparities in health care. World Psychiatry 10(1):52–77
Evans DL, Charney DS, Lewis L, Golden RN, Gorman JM, Krishnan KR, Nemeroff CB, Bremner JD, Carney RM, Coyne JC, Delong MR, Frasure-Smith N, Glassman AH, Gold PW, Grant I, Gwyther L, Ironson G, Johnson RL, Kanner AM, Katon WJ, Kaufmann PG, Keefe FJ, Ketter T, Laughren TP, Leserman J, Lyketsos CG, McDonald WM, McEwen BS, Miller AH, Musselman D, O’Connor C, Petitto JM, Pollock BG, Robinson RG, Roose SP, Rowland J, Sheline Y, Sheps DS, Simon G, Spiegel D, Stunkard A, Sunderland T, Tibbits P Jr, Valvo WJ (2005) Mood disorders in the medically ill: scientific review and recommendations. Biol Psychiatry 58:175–189
Moussavi S, Chatterji S, Verdes E, Tandon A, Patel V, Ustun B (2007) Depression, chronic diseases, and decrements in health: results from the World Health Surveys. The Lancet 370:851–858
Nemeroff CB, Musselman DL, Evans DL (1998) Depression and cardiac disease. Depress Anxiety 8(S1):71–79
Sareen J, Jacobi F, Cox BJ, Belik SL, Clara I, Stein MB (2006) Disability and poor quality of life associated with comorbid anxiety disorders and physical conditions. Arch Intern Med 166:2109–2116
Roy-Byrne PP, Davidson KW, Kessler RC, Asmundson GJ, Goodwin RD, Kubzansky L, Lydiard RB, Massie MJ, Katon W, Laden SK, Stein MB (2008) Anxiety disorders and comorbid medical illness. Gen Hosp Psychiatry 30(3):208–225. doi:10.1016/j.genhosppsych.2007.12.006
Ormel J, Von Korff M, Burger H, Scott K, Demyttenaere K, Huang Y, Posada-Villa J, Pierre Lepine J, Angermeyer MC, Levinson D (2007) Mental disorders among persons with heart disease - results from World Mental Health surveys. Gen Hosp Psychiatry 29(4):325–334
Beesdo K, Jacobi F, Hoyer J, Low NCP, Höfler M, Wittchen HU (2010) Pain associated with specific anxiety and depressive disorders in a nationally representative population sample. Soc Psychiatry Psychiatr Epidemiol 45(1):89–104
Scott K, Von Korff M, Alonso J, Angermeyer M, Bromet E, Fayyad J, De Girolamo G, Demyttenaere K, Gasquet I, Gureje O (2009) Mental-physical co-morbidity and its relationship with disability: results from the World Mental Health Surveys. Psychol Med 39(01):33–43
Sareen J, Cox BJ, Clara I, Asmundson GJ (2005) The relationship between anxiety disorders and physical disorders in the US National Comorbidity Survey. Depress Anxiety 21(4):193–202
Hasler G, Gergen PJ, Kleinbaum DG, Ajdacic V, Gamma A, Eich D, Roessler W, Angst J (2005) Asthma and panic in young adults: a 20-year prospective community study. Am J Respir Crit Care Med 171(11):1224
Wittchen HU, Jacobi F, Rehm J, Gustavsson A, Svensson M, Jonsson B, Olesen J, Allgulander C, Alonso J, Faravelli C, Fratiglioni L, Jennum P, Lieb R, Maercker A, van Os J, Preisig M, Salvador-Carulla L, Simon R, Steinhausen HC (2011) The size and burden of mental disorders and other disorders of the brain in Europe 2010. Eur Neuropsychopharmacol 21(9):655–679. doi:10.1016/j.euroneuro.2011.07.018
Adam Y, Meinlschmidt G, Gloster AT, Lieb R (2012) Obsessive-compulsive disorder in the community: 12-month prevalence, comorbidity and impairment. Soc Psychiatry Psychiatr Epidemiol 47:339–349. doi:10.1007/s00127-010-0337-5
Stengler-Wenzke K, Kroll M, Riedel-Heller S, Matschinger H, Angermeyer MC (2007) Quality of life in obsessive-compulsive disorder: the different impact of obsessions and compulsions. Psychopathology 40(5):282–289
Fullana M, Vilagut G, Rojas-Farreras S, Mataix-Cols D, de Graaf R, Demyttenaere K, Haro J, de Girolamo G, Lepine J, Matschinger H (2010) Obsessive-compulsive symptom dimensions in the general population: results from an epidemiological study in six European countries. J Affect Disord 124(3):291–299
Angst J, Gamma A, Endrass J, Goodwin R, Ajdacic V, Eich D, Rossler W (2004) Obsessive-compulsive severity spectrum in the community: prevalence, comorbidity, and course. Eur Arch Psychiatry Clin Neurosci 254(3):156–164. doi:10.1007/s00406-004-0459-4
De Bruijn C, Beun S, De Graaf R, Ten Have M, Denys D (2010) Subthreshold symptoms and obsessive compulsive disorder: evaluating the diagnostic threshold. Psychol Med 40(6):989–997
Grabe HJ, Meyer C, Hapke U, Rumpf HJ, Freyberger HJ, Dilling H, John U (2001) Lifetime-comorbidity of obsessive-compulsive disorder and subclinical obsessive-compulsive disorder in northern Germany. Eur Arch Psychiatry Clin Neurosci 251(3):130–135
Jacobi F, Wittchen HU, Holting C, Sommer S, Lieb R, Hofler M, Pfister H (2002) Estimating the prevalence of mental and somatic disorders in the community: aims and methods of the German National Health Interview and Examination Survey. Int J Methods Psychiatr Res 11(1):1–18
Jacobi F, Wittchen HU, Holting C, Hofler M, Pfister H, Muller N, Lieb R (2004) Prevalence, co-morbidity and correlates of mental disorders in the general population: results from the German Health Interview and Examination Survey (GHS). Psychol Med 34(4):597–611. doi:10.1017/S0033291703001399
Wittchen HU, Hoefler M, Gander F, Pfister H, Storz S, Uestun B, Mueller N, Kessler R (1999) Screening for mental disorders: performance of the Composite International Diagnostic Screener (CIDI-S). Int J Methods Psychiatr Res 8:59–70
Wittchen H, Pfister H (1997) DIA-X-Interviews: Manual für das Screening-Verfahren und Interview; Interviewheft Längsschnittuntersuchung (DIA-X-Lifetime); Ergänzungsheft (DIA-X-Lifetime): Interviewheft Querschnittsuntersuchung (DIA-X-12 Monate); Ergänzungsheft (DIA-X-12 Monate); PC-Programm zur Durchführung des Interviews (Längs- und Querschnittuntersuchung); Auswertungsprogramm. Swets & Zetilinger, Frankfurt
Wittchen HU, Lachner G, Wunderlich U, Pfister H (1998) Test-retest reliability of the computerized DSM-IV version of the Munich-Composite International Diagnostic Interview (M-CIDI). Soc Psychiatry Psychiatr Epidemiol 33(11):568–578
Reed V, Gander F, Pfister H, Steiger A, Sonntag H, Trenkwalder C, Hundt W, Wittchen HU (1998) To what degree does the Composite International Diagnostic Interview (CIDI) correctly identify DSM-IV disorders? Testing validity issues in a clinical sample. Int J Methods Psychiatr Res 7:142–155
StataCorp (2009) Stata Statistical Software: Release 11. College Station, TX
Agresti A (2002) Categorical data analysis. John Wiley and Sons Inc., Hoboken
Zuur A, Ieno E, Walker N, Saveliev A, Smith G (2009) Mixed effects models and extensions in ecology with R. Springer, New York
Muthén LK, Muthén BO (2006–2010) Mplus user’s guide, 6th edn. Muthén & Muthén, Los Angeles
Rothman K (2002) Epidemiology: an introduction. Oxford University Press, New York
Andersson T, Alfredsson L, Kaellberg H, Zdravkovic S, Ahlbom A (2005) Calculating measures of biological interaction. Eur J Epidemiol 20:575–579
R Development Core Team (2011) R: a language and environment for statistical computing. R Foundation for Statistical Computing, Vienna
Breslau N, Davis GC, Andreski P (1991) Migraine, psychiatric disorders, and suicide attempts: an epidemiologic study of young adults. Psychiatry Res 37(1):11–23
Micallef J, Blin O (2001) Neurobiology and clinical pharmacology of obsessive-compulsive disorder. Clin Neuropharmacol 24(4):191–207
Hamel E (2007) Serotonin and migraine: biology and clinical implications. Cephalalgia 27(11):1293–1300
Lake AE, Rains JC, Penzien DB, Lipchik GL (2005) Headache and psychiatric comorbidity: historical context, clinical implications, and research relevance. Headache 45(5):493–506
Dinn WM, Harris CL, McGonigal KM, Raynard RC (2001) Obsessive-compulsive disorder and immunocompetence. Int J Psychiatry Med 31:311–320
Murphy ML, Pichichero ME (2002) Prospective identification and treatment of children with pediatric autoimmune neuropsychiatric disorder associated with group A streptococcal infection (PANDAS). Arch Pediatr Adolesc Med 156(4):356
Goodwin RD, Olfson M, Shea S, Lantigua RA, Carrasquilo O, Gameroff MJ, Weissman MM (2003) Asthma and mental disorders in primary care. Gen Hosp Psychiatry 25(6):479–483
Scott KM, Von Korff M, Ormel J, Zhang M, Bruffaerts R, Alonso J, Kessler RC, Tachimori H, Karam E, Levinson D (2007) Mental disorders among adults with asthma: results from the World Mental Health Survey. Gen Hosp Psychiatry 29(2):123–133
Thomas M, Bruton A, Moffatt M, Cleland J (2011) Asthma and psychological dysfunction. Prim Care Respir J 20(3):250–256
Patten SB, Williams JVA, Esposito E, Beck CA (2006) Self-reported thyroid disease and mental disorder prevalence in the general population. Gen Hosp Psychiatry 28(6):503–508
Placidi G, Boldrini M, Patronelli A, Fiore E, Chiovato L, Perugi G, Marazziti D (1998) Prevalence of psychiatric disorders in thyroid diseased patients. Neuropsychobiology 38(4):222–225
Aizenberg D, Hermesh H, Gil-ad I, Munitz H, Tyano S, Laron Z, Weizman A (1991) TRH stimulation test in obsessive-compulsive patients. Psychiatry Res 38(1):21–26
Goodwin RD (2003) Association between physical activity and mental disorders among adults in the United States. Prev Med 36(6):698–703
Warburton DE, Nicol CW, Bredin SS (2006) Health benefits of physical activity: the evidence. CMAJ 174(6):801–809
Kogevinas M, Anto JM, Sunyer J, Tobias A, Kromhout H, Burney P (1999) Occupational asthma in Europe and other industrialised areas: a population-based study. The Lancet 353(9166):1750–1754
Tolin DF, Abramowitz JS, Brigidi BD, Foa EB (2003) Intolerance of uncertainty in obsessive-compulsive disorder. J Anxiety Disord 17(2):233–242
Katon W, Lin EHB, Kroenke K (2007) The association of depression and anxiety with medical symptom burden in patients with chronic medical illness. Gen Hosp Psychiatry 29(2):147–155
Katon WJ, Richardson L, Lozano P, McCauley E (2004) The relationship of asthma and anxiety disorders. Psychosom Med 66(3):349–355
Acknowledgments
We thank the Robert Koch Institute for kindly providing the data necessary for our analyses. The German Health Survey (GHS) was supported by Grant 01EH970/8 (German Federal Ministry of Research, Education and Science; BMBF). The reported data on mental disorders were assessed in the Mental Health Supplement of the GHS, conducted by the Max-Planck-Institute of Psychiatry, Munich, Germany. Principal investigator was Dr. Hans-Ulrich Wittchen. Reported somatic health status variables come from the GHS-Core Survey, conducted by the Robert Koch-Institute, Berlin, Germany. Principal investigators of the GHS-Core Survey were Dr. Bärbel-Maria Kurth and Dr. Wolfgang Thefeld. Data from this study are available as a Public Use File from: Dr. Frank Jacobi, Institute of Clinical Psychology and Psychotherapy, Chemnitzer Str. 46, 01187 Dresden, Germany; E-Mail: jacobi@psychologie.tu-dresden.de. For further information about the Core Survey and its Public Use File, contact the Robert Koch-Institute, Dr. Heribert Stolzenberg, Nordufer 20, 13353 Berlin, Germany; E-Mail: stolzenberg@rki.de.
Conflict of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution License which permits any use, distribution, and reproduction in any medium, provided the original author(s) and the source are credited.
About this article

Cite this article
Witthauer, C., T. Gloster, A., Meyer, A.H. et al. Physical diseases among persons with obsessive compulsive symptoms and disorder: a general population study. Soc Psychiatry Psychiatr Epidemiol 49, 2013–2022 (2014). https://doi.org/10.1007/s00127-014-0895-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00127-014-0895-z