
Abstract
Aims/hypothesis
The aim of this study was to assess the interaction between genetic risk and lifestyle intervention on the occurrence of gestational diabetes mellitus (GDM) and postpartum diabetes.
Methods
The RADIEL study is an RCT aimed at prevention of GDM and postpartum diabetes through lifestyle intervention. Participants with a BMI ≥30 kg/m2 and/or prior GDM were allocated to intervention and control groups before pregnancy or in early pregnancy. The study visits took place every 3 months before pregnancy, once in each trimester, and at 6 weeks and 6 and 12 months postpartum. We calculated a polygenic risk score (PRS) based on 50 risk variants for type 2 diabetes.
Results
Altogether, 516 participants provided genetic and GDM data. The PRS was associated with higher glycaemic levels (fasting glucose and/or HbA1c) and a lower insulin secretion index in the second and third trimesters and at 12 months postpartum, as well as with a higher occurrence of GDM and glycaemic abnormalities at 12 months postpartum (n = 356). There was an interaction between the PRS and lifestyle intervention (p=0.016 during pregnancy and p=0.024 postpartum) when analysing participants who did not have GDM at the first study visit during pregnancy (n = 386). When analysing women in tertiles according to the PRS, the intervention was effective in reducing the age-adjusted occurrence of GDM only among those with the highest genetic risk (OR 0.37; 95% CI 0.17, 0.82). The risk of glycaemic abnormalities at 12 months postpartum was reduced in the same group after adjusting additionally for BMI, parity, smoking and education (OR 0.35; 95% CI 0.13, 0.97).
Conclusions/interpretation
Genetic predisposition to diabetes modifies the response to a lifestyle intervention aimed at prevention of GDM and postpartum diabetes. This suggests that lifestyle intervention may benefit from being tailored according to genetic risk.
Clinical trial registration
ClinicalTrials.gov identifier: NCT01698385
Graphical abstract

Similar content being viewed by others

Avoid common mistakes on your manuscript.

Introduction
Gestational diabetes mellitus (GDM) is the most common pregnancy complication, with prevalence rates ranging from 1 to 28% [1], with adverse effects for the mothers and children involved. It results in increased short- and long-term morbidity, from perinatal complications such as macrosomia, birth trauma and increased Caesarean section rates [2], to elevated risk of diabetes and adiposity later in life, in both the mother and the child [3]. As women with prior GDM are at a tenfold higher risk of developing type 2 diabetes [4], there is an urgent need for prevention.
Lifestyle intervention has been successful in slowing, or even preventing, progression to type 2 diabetes in high risk individuals [5], and specifically among women with prior GDM [6]. However, the results of GDM prevention studies have been less consistent [7]. Some obtained positive results [8, 9] whereas others failed in their attempt [10]. In the RADIEL study (the Finnish Gestational Diabetes Prevention Study), lifestyle intervention succeeded in preventing GDM only in specific subgroups [8], and not among those recruited before pregnancy, for example [11]. The most recent Cochrane review [7] stated that the current evidence for a possible benefit from lifestyle intervention is at most modest, and that varying diagnostic criteria and heterogeneous study populations challenge the conclusions. The authors called for further research to disentangle the specific effects of lifestyle intervention in diverse groups of women.
One possible contributor to the discordant results may be genetic susceptibility. Studies over recent decades have provided interesting insights into the interplay between our genome and lifestyle. With regard to type 2 diabetes, several studies have revealed gene–environment interactions between specific SNPs and certain dietary factors and physical activity (PA), as well as weight reduction intervention [12]. Similarly, in the RADIEL study, we demonstrated how the MTNR1B polymorphism affected individual responses to lifestyle intervention [13]. Lately, the focus has shifted to the use of polygenic risk scores (PRS) [14], which enable calculation of the genetic risk based on multiple SNPs. However, it is not known whether the genetic risk of type 2 diabetes, as assessed by a PRS, affects the individual response to pregnancy lifestyle intervention aimed at prevention of GDM and early postpartum diabetes.
As lifestyle intervention requires both financial and human resources, it is crucial to identify those people benefitting the most from preventive efforts. Therefore, the aim of this study was to explore to what extent a type 2 diabetes PRS is associated with the glycaemic health of women at high risk of GDM, and whether the genetic risk modifies the effect of lifestyle intervention aimed at prevention of GDM and postpartum diabetes.
Methods
Study design and participants
This study is a secondary analysis of the randomised controlled intervention study RADIEL, which was performed during the years 2008–2013 in Helsinki University Hospital in Helsinki, Finland, and South Karelia Central Hospital, Lappeenranta, Finland. Previous publications have presented the details of the study [8, 15, 16].
The study participants were 18 years of age or older, and had a BMI ≥30 kg/m2 and/or a history of GDM. Multiple pregnancy, communication problems (based on language skills, for example), physical disabilities, medications or diagnoses affecting glucose metabolism, severe psychiatric diagnoses and current substance abuse led to exclusion. Women were recruited either before or in early pregnancy before 20 weeks of gestation, and allocated to an active lifestyle intervention group or a control group.
The study complied with the Declaration of Helsinki. All participants entered the study voluntarily, signed an informed consent form and were free to discontinue the study at any stage. The study was approved by the ethics committees of Helsinki University Hospital (14 September 2006, Dnro 300/E9/06) and South Karelia Central Hospital (11 September 2008, Dnro M06/08), and it was registered at ClinicalTrials.gov (clinical trial registration number NCT01698385).
Intervention
The combined lifestyle intervention, provided by trained study nurses, aimed at prevention of GDM among women at high diabetes risk. The study visits took place every 3 months before pregnancy, once in each trimester, and at 6 weeks and 6 and 12 months postpartum. The intervention group received individualised advice on increasing moderate-intensity PA to 150 min/week and limiting gestational weight gain. The dietary advice followed the Nordic dietary recommendations [17], and focused mainly on increasing the intake of fibre, vegetables, fruits and berries, as well as decreasing the intake of saturated fats. The control group attended the study visits for measurements but received only standard care such as general leaflets usually provided by antenatal clinics.
Measurements
At each study visit, anthropometric measurements were obtained and venous blood samples were taken. The biochemical analyses at each visit included assessments of glucose metabolism (HbA1c, fasting glucose, fasting insulin) and lipid metabolism (cholesterol, LDL-cholesterol, HDL-cholesterol, triacylglycerols), and inflammatory markers (high-sensitivity C-reactive protein). A 2 h 75 g OGTT was performed at enrolment, in the first and second trimester of pregnancy (unless GDM was diagnosed earlier), and at 6 weeks and 12 months postpartum. Participants with prior bariatric surgery or those with known diabetes diagnosis did not receive an OGTT. Background questionnaires covered socioeconomic status, lifestyle (e.g. smoking and medications), previous pregnancies, and family history of diabetes and cardiovascular diseases. Smoking in any trimester of pregnancy was recorded as ‘smoking during pregnancy’.
PA was self-reported as minutes of at least moderate-intensity PA per week. Based on the data from food frequency questionnaires, we calculated a healthy food intake index describing the quality of the diet overall. The maximum score was 18, with points for each nutritional goal: intake of high-energy/low-nutrient snacks (0, 1 or 2 points), sugar-sweetened beverages (0 or 1 points), fast food (0 or 1 points), high-fibre grains (0, 1 or 2 points), fat spread (0, 1 or 2 points), low-fat cheese (0 or 1 points), low-fat milk (0, 1 or 2 points), fish (0, 1 or 2 points), red and processed meat (0, 1 or 2 points), vegetables (0, 1 or 2 points), and fruits and berries (0 or 1 points). A higher score indicated a healthier diet.
Genotyping and calculating the type 2 diabetes polygenic risk score
DNA was extracted from whole blood samples from 537 participants using a Maxiprep kit (Qiagen, Valencia, CA, USA). We genotyped 336 SNPs associated with type 2 diabetes, obesity or hyperlipidaemia using a Sequenom iPLEX platform (Sequenom, San Diego, CA, USA) in the year 2014.
We used PLINK 1.9 software (http://pngu.mgh.harvard.edu/~purcell/plink/) for genotype quality control and clumping [18]. We used the following parameters for clumping of the genotype data: p value threshold 1, linkage disequilibrium threshold (r2) 0.5, clumping window width 250 kb. Prior to clumping, we excluded all SNPs with a minor allele frequency <0.05, genotyping rate <0.9 and Hardy–Weinberg equilibrium p value <1 × 10−4. We also excluded samples if data on >10% of SNPs were missing. After quality control, there were 537 samples with genotype data on 195 SNPs. We used PRSice 2.1 [19] to calculate the PRS, using the genotype quality control settings recommended by the software developers [20]. For the SNP weights, we used the effect-size estimates obtained from Xue et al [21]. We applied a p value threshold of 5 × 10−8 for including type 2 diabetes-associated SNPs in the PRS. This resulted in inclusion of 50 SNPs in the PRS.
Outcomes
The Finnish Current Care Guidelines provided the thresholds for diagnosing GDM based on 2 h 75g OGTT: 0 h ≥ 5.3 mmol/l, 1 h ≥10.0 mmol/l and 2 h ≥8.6 mmol/l [22]. One value exceeding any of the cut-offs led to a GDM diagnosis, and exceeding these thresholds in the first trimester led to a diagnosis of early GDM. ‘Booking GDM’ refers to a GDM diagnosis at enrolment (mean 13 gestational weeks) for the women recruited in early pregnancy.
Abnormal glucose metabolism 12 months postpartum refers to a diagnosis of either impaired fasting glucose (fasting glucose 6.1–6.9 mmol/l), impaired glucose tolerance (2 h glucose 7.8–11.0 mmol/l) or type 2 diabetes (fasting glucose ≥7.0 mmol/l or 2 h glucose ≥11.1 mmol/l). Alternatively, prior physician-diagnosed diabetes led to registration of a glycaemic abnormality. The indices for insulin resistance (HOMA-IR) and insulin secretion (HOMA-B) used the equations according to Matthews et al [23].
We also calculated a success score based on the example in the Finnish Diabetes Prevention Study [5], and modified the components of the score on achievement of the predefined lifestyle goals specific to this study. The maximum score was 5, consisting of the following: increasing fibre intake to 30 g or more (0 or 1 points), consumption of five or more portions of fruits, berries and vegetables per day (0 or 1 points), intake of saturated fats less than 10% of daily energy intake (0 or 1 points), gestational weight gain adequate or less than adequate according to the US Institute of Medicine’s guidelines [24] (0 or 1 points), and self-reported duration of moderate-intensity PA per week of 150 min or more (0 or 1 points). The definition of a successful intervention was three or more points.
Statistical analyses
The data are presented as mean values with SD, medians with IQR, or as frequencies with percentages. We used the Shapiro–Wilk test to examine the normal distribution of the variables. The χ2 test, Fisher’s exact test, Mann–Whitney U test, Kruskal–Wallis test, ANOVA, or independent-samples t test were used for between-group comparisons as appropriate.
Associations between the PRS and glycaemic markers were assessed using linear regression, and logistic regression was used when analysing the association with glycaemic diagnoses. Additionally, we included an interaction term in the regression analyses to detect the possible effect of an interaction between a type 2 diabetes PRS and lifestyle intervention on GDM incidence or the incidence of glycaemic abnormalities 12 months postpartum. In the case of any significant PRS × intervention interaction effects, we also assessed the SNP-level interactions. These analyses were adjusted for age.
To compare the effects of the intervention according to genetic risk, we divided the participants into tertiles based on their type 2 diabetes PRS: low risk (n = 176), medium risk (n = 176) and high risk (n = 177). The adjusted means for the occurrence of GDM and glycaemic abnormalities at 12 months postpartum were calculated using ANCOVA. All statistical tests were two-tailed.
All analyses were performed using the SPSS 24.0 software program (IBM SPSS, Chicago, IL, USA), and we considered a p value ≤0.05 as statistically significant.
Results
Of the 720 originally recruited women, DNA and data on GDM diagnosis during pregnancy were available from 516 women, of whom 356 attended the study visit at 12 months postpartum. Previous publications have provided detailed flow charts of the study [11, 25]. The participants who did not provide samples for the genetic studies were similar in terms of their baseline characteristics such as pre-pregnancy BMI, age, parity, occurrence of GDM and early GDM, PA and diet at baseline, as well as GDM history. However, they were more likely to smoke during pregnancy (10.3% vs 4.6%, p=0.020).
Among the participants included in this substudy, 130 presented with ‘booking GDM’, i.e. were already diagnosed at enrolment. There were no statistically significant differences between the intervention and control groups in terms of their age, pre-pregnancy BMI, socioeconomic status and parity. Additionally, there were no differences in the occurrence of GDM (48.9% in the intervention group vs 48.0% in the control group, p=0.852), GDM treated with medication (14.9% vs 12.0%, p=0.329), incidence of pre-eclampsia (5.3% vs 3.5%, p=0.299), smoking during pregnancy (4.3% vs 6.0%, p=0.396), Caesarean section rate (22.5% vs 24.3%, p=0.627) or newborn birthweight SD (0.23 SD vs 0.38 SD, p=0.110). However, women in the intervention group achieved the lifestyle intervention goals (3/5) more often (18.6% vs 10.6%, p=0.016).
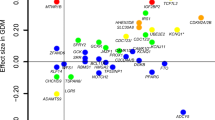
The type 2 diabetes PRS was associated with higher fasting glucose and/or HbA1c throughout pregnancy and during the first postpartum year (Table 1). With respect to insulin indices, an association was evident only for HOMA-B and not for HOMA-IR. There was also an association between the PRS and GDM, early GDM and glycaemic abnormalities at 12 months postpartum (Table 2). Electronic supplementary material (ESM) Table 1 lists all the included SNPs and their individual associations with the main outcomes (GDM and glycaemic abnormalities 12 months postpartum).
To assess the influence of a type 2 diabetes PRS on the effect of lifestyle intervention during pregnancy on GDM incidence, we excluded the participants with booking GDM, leaving a study population of 386 women. There was a statistically significant interaction between the PRS and the RADIEL lifestyle intervention on age-adjusted GDM incidence (p value for interaction = 0.014). To assess this effect further, we categorised the participants into tertiles according to their type 2 diabetes PRS: low, medium or high. Table 3 shows the characteristics of these three groups. Lifestyle intervention was effective in reducing the incidence of GDM only among women with a high type 2 diabetes PRS when adjusted for age (intervention effect OR 0.37; 95% CI 0.17, 0.82; p=0.014). The association remained significant after adjusting for age, pre-pregnancy BMI, parity, smoking, and years of education (intervention effect OR 0.39; 95% CI 0.17, 0.91; p=0.029) (Fig. 1).

Occurrence of GDM among women in the control and intervention groups according to their genetic risk of type 2 diabetes (tertiles of PRS), adjusted for age, smoking, years of education, parity and pre-pregnancy BMI. Error bars indicate 95% CI
There was also a statistically significant interaction between the type 2 diabetes PRS and the lifestyle intervention on the incidence of glycaemic abnormalities 12 months postpartum (p value for interaction = 0.023). When the analysis was performed using PRS tertiles, the intervention effect among women with a high type 2 diabetes PRS did not reach statistical significance when adjusted only for age (OR 0.41; 95% CI 0.16, 1.05; p=0.064). However, in the fully adjusted model (age, pre-pregnancy BMI, smoking and parity), the intervention was significantly associated with a reduced incidence of glycaemic abnormalities only among women with a high type 2 diabetes PRS (OR 0.35, 95% CI 0.13, 0.97, p=0.043) (Fig. 2). While there were a few significant individual SNP-level interactions, none of them were strong enough to drive the PRS interaction results (ESM Table 1).

Occurrence of glycaemic abnormalities (impaired fasting glucose, impaired glucose tolerance or type 2 diabetes) at 12 months postpartum among women in the control and intervention groups according to their genetic risk of type 2 diabetes (tertiles of PRS), adjusted for age, smoking, years of education, parity and pre-pregnancy BMI. Error bars indicate 95% CI
Discussion
Women with the highest type 2 diabetes PRS were most likely to benefit from lifestyle intervention for prevention of GDM in a randomised trial during pregnancy and the first postpartum year. A high PRS was associated with GDM diagnosis and markers of abnormal glucose metabolism in mid- and late pregnancy as well as 12 months postpartum. There was also an association with a lower insulin secretion index at various time points. The combined lifestyle intervention prevented GDM and postpartum glycaemic abnormalities 1 year after delivery only among the women with the highest type 2 diabetes PRS.
The RADIEL lifestyle intervention was not effective in preventing GDM or postpartum diabetes when analysing the entire study population. Many previous studies have also struggled to find an intervention effect [7]. Hence, researchers have attempted to identify discriminating factors that may explain heterogeneous responses between individuals. For example, O’Brien et al found that diet and/or lifestyle intervention had no clear effect on GDM incidence among women with a normal BMI [26]. In the meta-analysis by Madhuvrata et al, there was a reduction in GDM after diet intervention in women with risk factors for GDM [27]. Interestingly in the RADIEL study, despite having no clear impact on the primary study outcome (GDM incidence), the intervention improved the lifestyle of the participants significantly when measured using a success score. This may have potential implications. GDM is a complex metabolic disorder affecting more than just glycaemic variables, and lifestyle changes may influence the overall metabolic milieu of the fetus. In our previous study, the success score was associated with a more beneficial early growth profile of the offspring [28].
Previous studies on type 2 diabetes have suggested that genetic background may moderate individual responses to lifestyle intervention. A systematic review in 2019 reported that 28 of 66 eligible publications discovered significant gene–environment interactions [12]. These concerned specific SNPs and their interactions with either PA, diet or weight reduction interventions. For example, in the Diabetes Prevention Program and Diabetes Prevention Study, participants with the risk genotype TT in the TCF7L2 rs12255372 showed lower type 2 diabetes incidence in the intervention group than in the control group [29, 30]. In the Diabetes Prevention Program, the lifestyle intervention was effective in reducing type 2 diabetes incidence in individuals with higher genetic risk, such as risk variants in PPARG [31] and TNF [32]. The Nurses’ Health Study II showed that, when measuring genetic risk using a PRS, the quality of the diet [33] had the strongest effect among the participants with the highest type 2 diabetes PRS. Also, among women with prior GDM, lifestyle intervention has been associated with better postpartum glycaemic levels among carriers of a risk variant in CDKAL1 [34].
Less is known about the potential of genetic profiles to modify individual responses to lifestyle intervention aimed at GDM prevention. To our knowledge, this is the first study to report that genetic risk of type 2 diabetes modified the effectiveness of GDM lifestyle intervention. One of the few prior studies showed that women carrying the T allele of TCF7L2 rs7903146 showed a lower incidence of GDM when adhering to a Mediterranean diet [35]. The genetic background (rs10830963 in MTNR1B and rs1799884 in GCK) also modified the association between sausage intake and GDM risk [36]. In the RADIEL study, we have previously demonstrated an interaction between the MTNR1B risk allele and lifestyle intervention on GDM incidence [13], but that study included only the 269 participants recruited in early pregnancy with normal glucose tolerance in the first trimester.
There are also studies that did not detect any modifying effect of distinct genetic risk profiles. In the Diabetes Prevention Program study comparing 280 women with prior GDM with 1100 control women, the PRS was positively associated with history of GDM but did not modulate the response to a lifestyle intervention aimed at prevention of type 2 diabetes [37]. However, in that study, the PRS was calculated using only 34 diabetes-associated SNPs. Many studies assessing the effect of lifestyle intervention on overall cardiovascular risk have also not seen any interaction with the PRS used [38].
Choosing a PRS based on type 2 diabetes-related SNPs appears justified, as GDM shares a partly similar genetic background. A recent meta-analysis has supported this, finding 16 variants in eight loci common to both conditions [39]. Similar to previous studies [40], the type 2 diabetes PRS [21] was associated in our study with indices suggesting deficient insulin secretion but not with insulin resistance. It was also associated with most of the glycaemic markers assessed, especially in the second and third trimesters. In fact, the performance of the PRS was remarkably good considering that we were only able to include 50 SNPs instead of the original 143 significant SNPs listed by Xue et al [21].
Many earlier PRS studies have also aimed to identify women at high risk of GDM. Several studies [37, 41,42,43] discovered an association between a PRS based on type 2 diabetes-related variants and glycaemic traits during pregnancy. For example, the PRS used by Kawai et al comprised 34 SNPs previously associated with type 2 diabetes [43]. These scores also identify the women with prior GDM who are at higher risk of type 2 diabetes postpartum [37, 42]. One of the largest studies assessing postpartum diabetes risk was no exception: using 59 variants and analysing a total of 2434 women of European descent with a history of GDM from two independent cohorts, it found that a higher PRS was associated with an increased risk of postpartum type 2 diabetes [33].
Importantly, we did not identify any differences between the genetic risk groups in terms of their background characteristics such as years of education and age, or lifestyle factors such as smoking, PA or healthy food intake index. This improves the reliability and interpretation of our findings. There was a lower high-sensitivity C-reactive protein (p=0.012) in the high-risk group, and a lower pre-pregnancy BMI (p=0.072), although this did not reach statistical significance. Our recruitment criterion of only including normal-weight women if they had a history of GDM offers a natural and plausible explanation for this.
Among the strengths of our study is the study design, comprising an early pregnancy randomised lifestyle intervention, with a pre-pregnancy intervention arm and continuation of the intervention until the end of the first postpartum year. The diabetes risk of GDM women is suspected to be highest during the first 5 years after pregnancy, and therefore this early postpartum period may be particularly important for the future health of these women [4]. Moreover, it is advantageous that an OGTT was performed at the start of the study, enabling us to identify those with ‘booking GDM’. This is crucial when assessing the effects of the intervention. An additional strength is the use of a PRS to assess the genetic risk instead of only specific SNPs, as it gives a more comprehensive estimate of an individual’s genetic predisposition.
One of the limitations of our study is the moderate and focused sample of analysed SNPs. Of the original 143 loci reported by Xue et al [21], only 50 were genotyped in our focused analysis based on the known variants at that time. Naturally, genome-wide data may have given a greater perspective, and most probably would have improved the accuracy of the PRS. On the other hand, our PRS was highly correlated with glycaemic values (fasting glucose and HbA1c) during pregnancy. It is remarkable that genotyping only 50 SNPs could be used to target lifestyle intervention for GDM and postpartum diabetes prevention. This may be an advantage in the context of limited resources. Another limitation of our study is relying solely on calculated indices when referring to insulin secretion. This is important due to the hepatic extraction of insulin prior to its appearance in the systemic circulation. As obesity alters the fraction of hepatic insulin extraction, this may affect our results. The fact that our study comprised a genetically homogeneous population of women of European descent reduces the generalisability of our findings, but this may have contributed to the fact that our results are relatively unambiguous despite our small sample size compared with most genetic studies, and we believe that the randomised intervention design and the well-documented glycaemic values and clinical variables during pregnancy and the first postpartum year counteract this limitation.
Given the constantly increasing numbers of individuals with GDM and type 2 diabetes, finding a powerful means of individualised prevention is of great importance. In the present study, those at highest genetic risk of GDM and type 2 diabetes did not differ in their background characteristics or lifestyle, demonstrating the difficulty of stratifying women based only on their clinical characteristics. Therefore, including a type 2 diabetes PRS in the risk assessment may help to identify those women at highest risk and thus benefitting most from targeted intervention. To this end, there is a need to investigate larger and more diverse ethnic populations as well as various types of interventions. Additionally, it is important to assess whether genetic susceptibility modulates the effects of lifestyle intervention on outcomes in the offspring. As GDM is also associated with a higher risk of developing type 2 diabetes and obesity among offspring, future generations may also benefit from these essential interventions.
Data availability
The present informed consents do not allow archiving of clinical or register data in open repositories. Data described in the manuscript together with the codebook and the analytic code will be made available upon reasonable request. Requests regarding data availability can be addressed to the corresponding author (EH) and will be subject to further review by the national register authority and by the ethical committees.
Abbreviations
- GDM:
-
Gestational diabetes mellitus
- PA:
-
Physical activity
- PRS:
-
Polygenic risk score
- RADIEL:
-
The Finnish Gestational Diabetes Prevention Study
References
Saeedi M, Cao Y, Fadl H, Gustafson H, Simmons D (2021) Increasing prevalence of gestational diabetes mellitus when implementing the IADPSG criteria: A systematic review and meta-analysis. Diabetes Res Clin Pract 172:108642. https://doi.org/10.1016/j.diabres.2020.108642
Ornoy A, Becker M, Weinstein-Fudim L, Ergaz Z (2021) Diabetes during pregnancy: a maternal disease complicating the course of pregnancy with long-term deleterious effects on the offspring. A clinical review. Int J Mol Sci 22(6):2965
Lowe WL Jr, Scholtens DM, Lowe LP et al (2018) Association of gestational diabetes with maternal disorders of glucose metabolism and childhood adiposity. J Am Med Assoc 320(10):1005–1016. https://doi.org/10.1001/jama.2018.11628
Vounzoulaki E, Khunti K, Abner SC, Tan BK, Davies MJ, Gillies CL (2020) Progression to type 2 diabetes in women with a known history of gestational diabetes: systematic review and meta-analysis. BMJ 369:m1361. https://doi.org/10.1136/bmj.m1361
Tuomilehto J, Lindstrom J, Eriksson JG et al (2001) Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. N Engl J Med 344(18):1343–1350
Ratner RE, Christophi CA, Metzger BE et al (2008) Prevention of diabetes in women with a history of gestational diabetes: effects of metformin and lifestyle interventions. J Clin Endocrinol Metab 93(12):4774–4779. https://doi.org/10.1210/jc.2008-0772
Shepherd E, Gomersall JC, Tieu J, Han S, Crowther CA, Middleton P (2017) Combined diet and exercise interventions for preventing gestational diabetes mellitus. Cochrane Database Syst Rev 11(11):Cd010443. https://doi.org/10.1002/14651858.CD010443.pub3
Koivusalo SB, Rono K, Klemetti MM et al (2016) Gestational diabetes mellitus can be prevented by lifestyle intervention: the Finnish Gestational Diabetes Prevention Study (RADIEL) a randomized controlled trial. Diabetes Care 39(1):24–30. https://doi.org/10.2337/dc15-0511
Lin X, Yang T, Zhang X, Wei W (2020) Lifestyle intervention to prevent gestational diabetes mellitus and adverse maternal outcomes among pregnant women at high risk for gestational diabetes mellitus. J Int Med Res 48(12):300060520979130. https://doi.org/10.1177/0300060520979130
Simmons D, Devlieger R, van Assche A et al (2017) Effect of physical activity and/or healthy eating on GDM risk: the DALI lifestyle study. J Clin Endocrinol Metab 102(3):903–913. https://doi.org/10.1210/jc.2016-3455
Rönö K, Stach-Lempinen B, Eriksson JG et al (2018) Prevention of gestational diabetes with a prepregnancy lifestyle intervention - findings from a randomized controlled trial. Int J Womens Health 10:493–501. https://doi.org/10.2147/ijwh.S162061
Dietrich S, Jacobs S, Zheng JS, Meidtner K, Schwingshackl L, Schulze MB (2019) Gene–lifestyle interaction on risk of type 2 diabetes: A systematic review. Obes Rev 20(11):1557–1571. https://doi.org/10.1111/obr.12921
Grotenfelt NE, Wasenius NS, Rono K et al (2016) Interaction between rs10830963 polymorphism in MTNR1B and lifestyle intervention on occurrence of gestational diabetes. Diabetologia 59(8):1655–1658. https://doi.org/10.1007/s00125-016-3989-1
Ye Y, Chen X, Han J, Jiang W, Natarajan P, Zhao H (2021) Interactions between enhanced polygenic risk scores and lifestyle for cardiovascular disease, diabetes, and lipid levels. Circ Genom and Precis Med 14(1):e003128. https://doi.org/10.1161/CIRCGEN.120.003128
Rono K, Stach-Lempinen B, Klemetti MM et al (2014) Prevention of gestational diabetes through lifestyle intervention: study design and methods of a Finnish randomized controlled multicenter trial (RADIEL). BMC Pregnancy Childbirth 14:70. https://doi.org/10.1186/1471-2393-14-70
Huvinen E, Koivusalo SB, Meinila J et al (2018) Effects of a lifestyle intervention during pregnancy and first postpartum year – findings from the RADIEL study. J Clin Endocrinol Metab 103(4):1669–1677. https://doi.org/10.1210/jc.2017-02477
Nordic Council of Ministers (2014) Nordic nutrition recommendations 2012: Integrating nutrition and physical activity, 5th ed. Nordisk Ministerråd, Copenhagen
Purcell S, Neale B, Todd-Brown K et al (2007) PLINK: a tool set for whole-genome association and population-based linkage analyses. Am J Hum Genet 81(3):559–575. https://doi.org/10.1086/519795
Choi SW, O'Reilly PF (2019) PRSice-2: polygenic risk score software for biobank-scale data. GigaScience 8(7):giz082
Euesden J, Lewis CM, O'Reilly PF (2015) PRSice: polygenic risk score software. Bioinformatics 31(9):1466–1468. https://doi.org/10.1093/bioinformatics/btu848
Xue A, Wu Y, Zhu Z et al (2018) Genome-wide association analyses identify 143 risk variants and putative regulatory mechanisms for type 2 diabetes. Nat Commun 9(1):1–14
Finnish Medical Society Duodecim (2013) Gestational diabetes. Current care recommendation. Available from http://www.kaypahoito.fi/web/english/guidelineabstracts/guideline?id=ccs00047. Accessed 12 Nov 2021
Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC (1985) Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 28(7):412–419. https://doi.org/10.1007/bf00280883
US Institute of Medicine and US National Research Council Committee to Reexamine Institute of Medicine Pregnancy Weight Guidelines (2009) Weight gain during pregnancy: reexamining the guidelines, Rasmussen KM, Yaktine AL (eds). National Academies Press, Washington DC, USA
Rönö K, Grotenfelt NE, Klemetti MM et al (2018) Effect of a lifestyle intervention during pregnancy – findings from the Finnish gestational diabetes prevention trial (RADIEL). J Perinatol 38(9):1157–1164. https://doi.org/10.1038/s41372-018-0178-8
O'Brien CM, Grivell RM, Dodd JM (2016) Systematic review of antenatal dietary and lifestyle interventions in women with a normal body mass index. Acta obstetricia et gynecologica Scandinavica 95(3):259–269
Madhuvrata P, Govinden G, Bustani R, Song S, Farrell TA (2015) Prevention of gestational diabetes in pregnant women with risk factors for gestational diabetes: a systematic review and meta-analysis of randomised trials. Obstet Med 8(2):68–85
Huvinen E, Tuomaala AK, Bergman PH et al (2021) Ascending growth is associated with offspring adiposity in pregnancies complicated with obesity or gestational diabetes. J Clin Endocrinol Metab 106(5):e1993–e2004. https://doi.org/10.1210/clinem/dgaa979
Florez JC, Jablonski KA, Bayley N et al (2006) TCF7L2 polymorphisms and progression to diabetes in the Diabetes Prevention Program. N Engl J Med 355(3):241–250. https://doi.org/10.1056/NEJMoa062418
Wang J, Kuusisto J, Vänttinen M et al (2007) Variants of transcription factor 7-like 2 (TCF7L2) gene predict conversion to type 2 diabetes in the Finnish Diabetes Prevention Study and are associated with impaired glucose regulation and impaired insulin secretion. Diabetologia 50(6):1192–1200. https://doi.org/10.1007/s00125-007-0656-6
Kilpeläinen TO, Lakka TA, Laaksonen DE et al (2008) SNPs in PPARG associate with type 2 diabetes and interact with physical activity. Med Sci Sports Exerc 40(1):25–33. https://doi.org/10.1249/mss.0b013e318159d1cd
Kubaszek A, Pihlajamäki J, Komarovski V et al (2003) Promoter polymorphisms of the TNF α (G 308A) and IL-6 (C 174G) genes predict the conversion from impaired glucose tolerance to type 2 diabetes: the finnish diabetes prevention study. Diabetes 52(7):1872–1876. https://doi.org/10.2337/diabetes.52.7.1872
Li M, Rahman ML, Wu J et al (2020) Genetic factors and risk of type 2 diabetes among women with a history of gestational diabetes: findings from two independent populations. BMJ Open Diabetes Res Care 8(1):e000850. https://doi.org/10.1136/bmjdrc-2019-000850
Liang Z, Wang L, Liu H et al (2020) Genetic susceptibility, lifestyle intervention and glycemic changes among women with prior gestational diabetes. Clin Nutr 39(7):2144–2150. https://doi.org/10.1016/j.clnu.2019.08.032
Barabash A, Valerio JD, Garcia de la Torre N et al (2020) TCF7L2 rs7903146 polymorphism modulates the association between adherence to a Mediterranean diet and the risk of gestational diabetes mellitus. Metabol Open 8:100069. https://doi.org/10.1016/j.metop.2020.100069
Popova PV, Klyushina AA, Vasilyeva LB et al (2017) Effect of gene–lifestyle interaction on gestational diabetes risk. Oncotarget 8(67):112024–112035. https://doi.org/10.18632/oncotarget.22999
Sullivan SD, Jablonski KA, Florez JC et al (2014) Genetic risk of progression to type 2 diabetes and response to intensive lifestyle or metformin in prediabetic women with and without a history of gestational diabetes mellitus. Diabetes Care 37(4):909–911. https://doi.org/10.2337/dc13-0700
Said MA, Verweij N, van der Harst P (2018) Associations of combined genetic and lifestyle risks with incident cardiovascular disease and diabetes in the UK biobank study. JAMA Cardiol 3(8):693–702. https://doi.org/10.1001/jamacardio.2018.1717
Powe CE, Kwak SH (2020) Genetic studies of gestational diabetes and glucose metabolism in pregnancy. Curr Diab Rep 20(12):69. https://doi.org/10.1007/s11892-020-01355-3
Zhang C, Bao W, Rong Y et al (2013) Genetic variants and the risk of gestational diabetes mellitus: a systematic review. Hum Reprod Update 19(4):376–390. https://doi.org/10.1093/humupd/dmt013
Powe CE, Nodzenski M, Talbot O et al (2018) Genetic determinants of glycemic traits and the risk of gestational diabetes mellitus. Diabetes 67(12):2703–2709. https://doi.org/10.2337/db18-0203
Cormier H, Vigneault J, Garneau V et al (2015) An explained variance-based genetic risk score associated with gestational diabetes antecedent and with progression to pre-diabetes and type 2 diabetes: a cohort study. BJOG 122(3):411–419. https://doi.org/10.1111/1471-0528.12937
Kawai VK, Levinson RT, Adefurin A et al (2017) A genetic risk score that includes common type 2 diabetes risk variants is associated with gestational diabetes. Clin Endocrinol 87(2):149–155. https://doi.org/10.1111/cen.13356
Authors’ relationships and activities
MO-M is a member of the editorial board of Diabetologia. The authors declare that there are no other relationships or activities that might bias, or be perceived to bias, their work.
Contribution statement
SBK, the principal investigator of the study, initiated and coordinated the study, and SBK, EH, JL, HL, MMK, MO-M, PHB and KR participated in the design of the study. EH and SBK participated in the implementation of the study. EH performed the literature search. EH, JL and PHB performed the statistical analyses of the data, and HL, SBK, MMK, KR and MO-M participated in the data interpretation. EH, JL, SBK and HL performed the initial drafting of the article and MMK, PHB, MO-M and KR participated in the editing of the article. HL is the principal investigator of the genetic substudy and MO-M was responsible for genotyping the samples. All authors have read and approved the final version of the manuscript. EH is the guarantor of this work, and, as such, had full access to all the data in the study and takes full responsibility for the integrity of the data and the accuracy of the data analysis.
Funding
Open Access funding provided by University of Helsinki including Helsinki University Central Hospital. This study was funded by the Finnish Medical Foundation, the Alfred Kordelin Foundation, the Juho Vainio Foundation, the Ahokas Foundation, the Finnish Foundation for Cardiovascular Disease, the Academy of Finland, the Special State Subsidy for Health Science Research of Helsinki University Hospital, Samfundet Folkhälsan, Finska Läkaresällskapet, the Viipuri Tuberculosis Foundation, the Finnish Diabetes Research Foundation, the State Provincial Office of Southern Finland, a health promotion grant from the Finnish Ministry of Social Affairs and Health (EU H2020-PHC-2014 DynaHealth grant number 633595) and the Social Insurance Institution of Finland. The funders did not have any role in designing or conducting the study, in the collection, management, analysis or interpretation of the data, or in the preparation, review or approval of the manuscript and the decision to submit the manuscript for publication.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
ESM 1
(PDF 176 kb)
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Huvinen, E., Lahti, J., Klemetti, M.M. et al. Genetic risk of type 2 diabetes modifies the effects of a lifestyle intervention aimed at the prevention of gestational and postpartum diabetes. Diabetologia 65, 1291–1301 (2022). https://doi.org/10.1007/s00125-022-05712-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00125-022-05712-7