
Abstract
Aims/hypothesis
The aim of this work was to examine the associations of average weight and weight velocity in three growth periods from birth through adolescence with type 2 diabetes incidence.
Methods
Child participants were selected from a 43 year longitudinal study of American Indians to represent three growth periods: pre-adolescence (birth to ~8 years); early adolescence (~8 to ~13 years); and late adolescence (~13 to ~18 years). Age-, sex- and height-standardised weight z score mean and weight z score velocity (change/year) were computed for each period. Participants were followed for up to 25 years from the end of each growth period until they developed diabetes. Associations of weight z score mean or weight z score velocity with diabetes incidence were determined with sex-, birth date- and maternal diabetes-adjusted Poisson regression models.
Results
Among 2100 participants representing the pre-adolescence growth period, 1558 representing the early adolescence period and 1418 representing the late adolescence period, there were 290, 315 and 380 incident diabetes cases, respectively. During the first 10 years of follow-up, the diabetes incidence rate ratio (95% CI) was 1.72 (1.40, 2.11)/SD of log10 weight z score mean in pre-adolescence, 2.09 (1.68, 2.60)/SD of log10 weight z score mean in early adolescence and 1.85 (1.58, 2.17)/SD of log10 weight z score mean in late adolescence. The diabetes incidence rate ratio (95% CI) was 1.79 (1.49, 2.17)/SD of log10 weight z score velocity in pre-adolescence, 1.13 (0.91, 1.41)/SD of log10 weight z score velocity in early adolescence and 1.29 (1.09, 1.51)/SD of log10 weight z score velocity in late adolescence. There were strong correlations in the weight z score means and weak correlations in the weight z score velocities between successive periods.
Conclusions/interpretation
Higher weight and accelerated weight gain in all growth periods associate with increased type 2 diabetes risk. Importantly, higher weight and greater weight velocity during pre-adolescence jointly associate with the highest type 2 diabetes risk.

Graphical abstract
Similar content being viewed by others

Introduction
The incidence and prevalence of obesity are increasing among children and adolescents in the USA [1, 2], coinciding with an increasing type 2 diabetes incidence among youth and young adults [3, 4]. Excessive body weight in childhood or adolescence often persists into adulthood [5], thereby increasing the risk of early-onset type 2 diabetes [6, 7]. Given the significant long-term complications and mortality risk associated with early-onset type 2 diabetes [8, 9], careful monitoring of growth in childhood and adolescence is important. However, evidence on the impact of variability in weight gain at critical growth periods on type 2 diabetes development is limited by a paucity of serial anthropometric data for weight tracking from early childhood or prospective biochemical data for ascertaining type 2 diabetes incidence [6, 10,11,12,13,14,15,16,17,18,19].
Obesity and type 2 diabetes are highly prevalent among Pima Indians living in south-western USA, especially among children and young adults [20, 21], with associated long-term effects on health [22]. In the present study, we use longitudinal data obtained from Pima children and adults to identify critical growth periods during childhood and adolescence that are associated with type 2 diabetes incidence. We hypothesised that both higher average weight and faster weight gain in childhood and adolescence associate with greater type 2 diabetes risk, and that these associations differ by the growth period.
Methods
Study design and participants
A longitudinal open cohort study of diabetes and related complications in individuals aged ≥5 years was conducted in the Gila River Indian Community in Arizona from 1965 to 2007. Diabetes in this community is thought to be exclusively type 2, as available data from children and adults with diabetes suggest no autoimmunity (i.e. islet cell antibodies including GAD65) typical of type 1 diabetes or insulin dependence even in those with very young onset [23, 24].
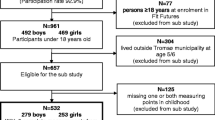
Participants undertook standardised research examinations approximately every 2 years. Although longitudinal study participants were aged ≥5 years, data on events preceding participation (e.g. birthweight) were obtained from secondary sources (medical records, birth certificates) when available. Because participants entered the biennial study at different ages, and the time points at which research examinations occurred were not uniform, serial data in childhood were limited. To maximise the available data, we used data obtained at four time points (Fig. 1): birth; age ~8 (range 7–9 at the last birthday, median 8.4) years; age ~13 (range 12–14, median 13.2) years; and age ~18 (range 17–19, median 18.3) years. If a participant had more than one examination in the window defining a time point, only the examination closest to the midpoint age was used. These time points were used to define three sequential growth periods: pre-adolescence (birth to ~8 years); early adolescence (~8 to ~13 years); and late adolescence (~13 to ~18 years) (Fig. 1).

Study design and calculation of weight z score means and velocities. Age ~8 years ranged from 7–9 (median 8.4) years, age ~13 years ranged from 12–14 (median 13.2) years, age ~18 years ranged from 17–19 (median 18.3) years; wtz is the log10 weight z score at the indicated time point. Analyses were conducted separately for each growth period, so a participant representing more than one growth period could be followed for varying lengths of time as the start point for follow-up varies by growth period
Although adolescence is typically defined as age 10–19 years, this period varies across populations and contexts [25]. Data are limited on age at puberty among American Indians. We selected 7–9 years as the endpoint for pre-adolescence, as the mean age at menarche among Pima Indian girls is 12 years [26] and menarche occurs 2–3 years after the onset of the first signs of puberty. Coincidentally, most of the available data points in early childhood were concentrated in this age range. We selected age 12–14 and 17–19 years as the endpoint for early and late adolescence, respectively, to maximise available data points in adolescence while reflecting the variability in growth at this stage of childhood.
Participants were included in the analysis for a growth period if they met the following requirements: had height and weight measurements at the beginning and the end of the period; did not have diabetes during the period (ascertained using OGTTs at the research examinations, including examinations defining the growth periods); and had at least one research examination after the period. Participants could be included in the analysis for more than one growth period. The study was approved by the Institutional Review Board of the National Institute of Diabetes and Digestive and Kidney Diseases. Minors (aged <18 years) gave assent, and written informed consent was obtained from their parents. Participants aged ≥18 years provided written informed consent.
Data collection
At each research examination, height was measured to the nearest cm and weight to the nearest kg while participants were dressed in light clothing without shoes. Birthweight was obtained from birth certificates and medical records. A 75 g OGTT was performed at each examination. Diabetes was ascertained using WHO criteria (2 h plasma glucose concentration ≥11.1 mmol/l [200 mg/dl]) [27] or by diagnosis documented during routine clinical care between research examinations. More recently adopted tests for diabetes, such as fasting plasma glucose and HbA1c, were not used in this analysis because they were not used throughout the longitudinal study, which began in 1965. OGTT or documented clinical diagnosis were used to ascertain maternal diabetes prior to the birth of the participant. A subgroup of 2630 participants was assessed for functional mutation of the melanocortin-4 receptor gene (MC4R), a common cause of both obesity and type 2 diabetes in childhood and adolescence in this study population [26]. MC4R variants have a larger effect on obesity traits among Pima Indians than other known genetic variants associated with obesity in childhood and adolescence.
Statistical analysis
Participants’ characteristics were summarised with descriptive statistics, including median, 25th (Q1) and 75th (Q3) centiles for non-normally distributed variables. The objective was to estimate the associations with diabetes incidence of two growth variables at different points in childhood: standardised weight at a point and standardised weight velocity at an interval leading to that point. To achieve this, we modelled weight-for-height rather than BMI since the former is more appropriate for modelling growth in children and the latter leaves residual confounding by height [28]. Weights in childhood and adolescence were standardised to the study population to obtain z scores: (1) by identifying sex-specific age- and height-adjusted regression models that provide the best fit for weight (i.e. log10 weight = β0 + β1age + β2height for male and female sex); and (2) by standardising residuals from each model to mean = 0 and SD = 1. Because data on gestational age and length at birth were unavailable, birthweight was standardised to mean = 0 and SD = 1, separately by sex.
Standardised measures of weight at a point and of weight velocity during an interval leading to that point are strongly correlated thereby limiting the ability to clearly delineate their individual and joint associations. This correlation can be minimised considerably by using the average and the difference of two scores [29, 30], so we analysed both the weight z score mean and the weight z score velocity of each participant for each growth period (Fig. 1). The weight z score mean was the z score of the mean of log10 weight z scores at the points defining a growth period, while the weight z score velocity was the z score of the difference in log10 weight z scores divided by the length (in years) of the growth period (Fig. 1). Growth was modelled using this approach because of limited data at regular age intervals in childhood in this study.
Although some correlation was introduced by using some of the same measures to calculate the weight z score mean or weight z score velocity for the growth periods (Fig. 1), these overlapping measures were not included in the same model, thus avoiding collinearity. Diabetes incidence was analysed separately for each growth period and, thus, separately for each group of participants representing the growth periods. Each participant was followed from the examination that defined the end of the corresponding growth period until diabetes incidence or the last research examination, whichever came first (Fig. 1). Follow-up was restricted to up to 25 years as inclusion of the limited (<1000 person-years) follow-up data beyond this point may reduce the precision of the incidence rate estimates and its omission ensured better balance in the length of follow-up between groups.
Diabetes incidence rate was calculated per 1000 person-years of follow-up. Poisson regression was used to model diabetes incidence rate ratios (IRRs) for the weight z score mean or weight z score velocity in a growth period with the offset term, log (person-years), accounting for different lengths of follow-up. Models were adjusted for sex, birth date and maternal diabetes. For each growth period, weight z score mean and weight z score velocity were analysed in separate models (to estimate their individual associations) and then jointly in the same model (to estimate their joint associations). In some models (particularly those estimating the IRR for weight z score means), associations of the weight z score mean or weight z score velocity with diabetes IRR were non-proportional (i.e. non-constant) over time. Therefore, time was split into follow-up intervals of 5 years and IRRs were estimated for increasing 5 year intervals of follow-up (e.g. a participant who was censored at the 18th year of follow-up was included in the analysis for <5 years, <10 years, <15 years and <20 years).
All models were tested for potential interactions of the exposure variables with sex, birth date or maternal diabetes by including product terms. Models were also tested for any quadratic (non-linear) associations of the weight variables with type 2 diabetes incidence.
A bootstrap analysis was performed to account for the partial overlap of participants representing the growth periods, for any potential imbalance of covariates between groups and for any correlation arising from using some of the same measures to calculate the weight z score mean or weight z score velocity for the growth periods. Briefly, we drew 10,000 random samples of participants in the longitudinal analysis with replacement to obtain a bootstrapped estimate of the SE of the difference in risk estimates between the growth periods; this SE was used to assess the significance of the difference. This approach assumes that the bootstrapped statistic approximates a normal distribution [31].
Some sensitivity analyses were performed. To use all available data points in childhood, we estimated weight z score velocities using the linear spline mixed-effects model [32]. This multilevel approach involved using piecewise linear splines with knots at age 9 years (at the last birthday) and 14 years (at the last birthday). The positions of the knots were selected to obtain linear slopes of log10 weight z scores corresponding to the growth periods analysed in the initial (simple) growth modelling approach (i.e. birth–9 years, 9–14 years and 14–19 years). The estimated slopes, which varied between participants, were standardised to mean = 0 and SD = 1 and were subsequently used as continuous variables in Poisson regression models to estimate diabetes IRRs. The slope in each growth period was adjusted for the weight z score mean in that period and for other covariates (sex, birth date and maternal diabetes). For more details on these analyses, please see the SAS syntax in electronic supplementary material (ESM) Methods.
To test whether risk estimates were influenced by exposure to maternal diabetes, models were restricted to participants without such exposure. Similarly, models were also restricted to participants without functional mutations in MC4R to test any influence of such mutations. Finally, models were adjusted for birthweight in analyses restricted to participants with data on birthweight.
All analyses were performed using SAS version 9.4 (SAS Institute, NC, USA). A two-sided p < 0.05 was considered statistically significant.
Results
Characteristics of participants
This study involved children representing growth periods of pre-adolescence (n = 2100), early adolescence (n = 1558) and late adolescence (n = 1418). Overall, the present analysis included 3107 participants (some representing more than one growth period). Participants representing late adolescence were more often female sex (63.3%) than those representing pre-adolescence (52.2%) or early adolescence (55.2%) (Table 1). The proportion exposed to maternal diabetes was similar among participants representing each growth period. Although there was balance in the median follow-up period to the endpoint for this analysis, participants representing pre-adolescence had a greater median number of follow-up visits (n = 6) than those representing later growth periods (n = 3) (Table 1). The percentage of diabetes diagnoses made during follow-up research examinations (as opposed to diagnoses from clinical data) was comparable for the different growth periods (59.3% for pre-adolescence, 56.8% for early adolescence and 54.2% for late adolescence).
Among participants representing more than one growth period, there were significant correlations in the weight z score means between successive periods (i.e. r = 0.67 between weight z scores in pre-adolescence and early adolescence, r = 0.92 between early adolescence and late adolescence and r = 0.49 between pre-adolescence and late adolescence) (Fig. 2). By contrast, only weight z score velocities in early and late adolescence showed significant but weak negative correlation (r = −0.19).

Correlations of age-, sex- and height-standardised weight z score mean (a–c) and weight z score velocity (d–f) in pre-adolescence, early adolescence and late adolescence. No. of participants analysed: 1244 for pre-adolescence (birth to age ~8 years, a, d); 725 for early adolescence (age ~8 years to ~13 years, b, e); and 595 for late adolescence (age ~13 years to ~18 years, c, f). See Methods for precise definitions of the three growth periods
Diabetes incidence
During up to 25 years of follow-up from the end of the growth periods, the number of incident cases of diabetes among participants representative of each growth period was 290 for pre-adolescence (10.1 per 1000 person-years), 315 for early adolescence (15.2 per 1000 person-years) and 380 for late adolescence (22.0 per 1000 person-years) (Table 2). Overall, there were 607 unique incident diabetes cases, 63% occurring in the female sex. At the first research examination with diabetes, the mean age of participants was 28 years and 89% were obese (BMI ≥30 kg/m2; ESM Table 1). Incidence rate estimates became less precise when analyses were extended beyond 25 years of follow-up because fewer participants had >25 years of follow-up (ESM Table 2).
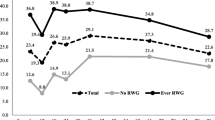
When adjusted for sex, birth date and maternal diabetes, greater weight z score mean in each growth period associated with increased diabetes incidence during the first 10 years of follow-up (Fig. 3a and ESM Table 3). The IRR (95% CI) was 1.72 (1.40, 2.11)/SD of log10 weight z score mean in pre-adolescence, 2.09 (1.68, 2.60)/SD of log10 weight z score mean in early adolescence and 1.85 (1.58, 2.17)/SD of log10 weight z score mean in late adolescence. Although these associations declined over time (ESM Fig. 1a–c), they persisted for up to 25 years of follow-up (Fig. 3b). Comparing associations across the growth periods, there was no significant difference in the association of the weight z score mean with diabetes incidence (p ≥ 0.05).

Sex-, date of birth- and maternal diabetes-adjusted individual association by growth period of weight z score mean with type 2 diabetes incidence during the first 10 years (a) and up to 25 years of follow-up (b) and of weight z score velocity with type 2 diabetes incidence during the first 10 years (c) and up to 25 years of follow-up (d). Pre-adolescence (Pre) is birth to age ~8 years, early adolescence (Early) is age ~8 years to ~13 years and late adolescence (Late) is age ~13 years to ~18 years. See Methods for precise definitions of the three growth periods
Weight z score velocity during pre-adolescence significantly associated with diabetes incidence during the first 10 years of follow-up (IRR [95% CI]/SD of log10 weight z score velocity 1.79 [1.49, 2.17]) (Fig. 3c and ESM Table 3), with this significant association persisting for up to 25 years of follow-up (Fig. 3d and ESM Fig. 1d). Weight z score velocity in early adolescence had no significant effect on subsequent diabetes incidence during the first 10 years of follow-up (IRR [95% CI]/SD of log10 weight z score velocity 1.13 [0.91, 1.41]) (Fig. 3c) but had a significant, albeit relatively weak, association when follow-up was extended to up to 25 years (IRR [95% CI]/SD of log10 weight z score velocity 1.16 [1.05, 1.30]) (Fig. 3d and ESM Fig. 1e). Similarly, compared with pre-adolescence, the cumulative association of weight z score velocity in late adolescence with diabetes incidence was weak during the first 10 years of follow-up and up to 25 years of follow-up (IRR [95% CI]/SD of log10 weight z score velocity 1.29 [1.09, 1.51] and 1.19 [1.07, 1.32], respectively) (Fig. 3c,d and ESM Fig. 1f). Overall, weight z score velocity had a significantly greater association with diabetes incidence in pre-adolescence than in early adolescence (p < 0.001) and late adolescence (p = 0.016).
For each growth period, the pattern and magnitude of the joint association of weight z score mean and weight z score velocity with diabetes incidence (ESM Table 4) were similar to those of the individual associations. There were no significant interactions of sex, birth date or maternal diabetes with either the weight z score mean or weight z score velocity in any analyses. Neither was there any significant non-linear association between the weight variables and type 2 diabetes incidence.
Sensitivity analysis
Findings from the linear spline mixed-effects model, adjusted for weight z score mean, sex, birth date and maternal diabetes, were generally similar to those of the initial (simple) modelling approach: weight z score velocity more strongly associated with type 2 diabetes incidence in pre-adolescence than in early and late adolescence (ESM Table 5). However, unlike the simple model, the linear spline mixed-effects model showed a significant association between weight z score velocity in early adolescence and type 2 diabetes incidence during the first 10 years of follow-up and up to 25 years of follow-up (IRR [95% CI]/SD of log10 weight z score 1.34 [1.07, 1.68] and 1.25 [1.07, 1.37], respectively).
Results were similar when models were restricted to participants without exposure to maternal diabetes (ESM Table 6) or when models were restricted to participants with no known MC4R deficiency (data not shown). Similar results were obtained when comparing analyses using models adjusted for birthweight vs models not adjusted for this covariate (ESM Table 7) and models comprising weight z scores (Fig. 3) vs models comprising BMI z scores (ESM Fig. 2).
Discussion
Statement of principal findings
In this longitudinal analysis, higher weight in all growth periods significantly associated with greater type 2 diabetes incidence, as did accelerated weight gain in pre-adolescence and late adolescence. Importantly, higher weight and greater weight velocity pre-adolescence jointly associated with the highest type 2 diabetes risk; these associations were similar, but weaker, for higher weights and greater weight velocities in early and late adolescence.
Strengths and weaknesses of the study
The strength of this study is the prospective ascertainment of diabetes using OGTTs. In addition, all anthropometric and biochemical measurements were performed at the same centre and laboratory for the entire 43 year study. Importantly, our longitudinal data permit the identification of critical and clinically meaningful growth periods.
Our study did not adjust birthweight for length at birth and gestational age or adjust analyses for age at puberty, diet, physical activity or socioeconomic status because of insufficient data on these variables. Due to limited serial research examination in childhood, growth was modelled using a simple approach that used weight measures from selected data points rather than all available data points. However, conclusions were not substantially affected when all available data were used in a linear spline mixed-effects model. We were unable to use other analytical approaches such as growth curve modelling (requiring more data) or age-period-cohort analysis (requiring larger sample sizes at age intervals). There is potential for selection bias given the greater proportion of female sex among participants representing the late adolescence period, although there is no evidence that risk was modified by sex. However, our estimates should be interpreted in the context that administrative censoring limited the proportion of participants completing all growth periods (i.e. children who were younger in the early years of the longitudinal study had longer potential follow-up than those who entered the study later). Pima Indians have a high prevalence of obesity and early-onset type 2 diabetes [19, 20]. However, prior findings on childhood obesity and type 2 diabetes in this population have generally been replicated in other populations.
Strengths and weaknesses in relation to other studies
Our findings on the association between childhood weight and type 2 diabetes incidence agree largely with results of previous studies, although direct comparisons are difficult given the inconsistencies in the growth periods examined, lack of longitudinal data on type 2 diabetes incidence, and differences in analytical approach. Similar to our findings, greater BMI z score at age 4–19 years consistently associated with higher prevalence of prediabetes or type 2 diabetes in adulthood in the Bogalusa Heart study [12]. Moreover, being overweight at age 13 years (BMI ≥21.8 kg/m2) and persistently overweight at ages 7 years (BMI ≥17.4 kg/m2) and 13 years associated with greater type 2 diabetes among adult Danish men (age 30–60 years) [6]. However, contrary to our findings, being overweight at 7 years (unadjusted for subsequent weight) was not associated with type 2 diabetes incidence in the Danish study. The contrasting results may be due to differences in the analytical method as BMI was categorised and diabetes incidence was assessed from age ≥30 years in the Danish study. In our study, weight was analysed as a continuous variable while diabetes incidence was assessed from childhood. In a larger and sex-diverse Danish study [13], although there were no significant interactions of childhood BMI with covariates, analyses were stratified by BMI, sex, birth cohort and age at diagnosis, thereby complicating the interpretation of findings. We showed previously the additive effects of postnatal BMI, birthweight, maternal diabetes and genotype on type 2 diabetes incidence [33]. In the present analysis, birthweight, maternal diabetes, and genotype did not significantly add to or modify the association between the child weight variables and type 2 diabetes incidence. Similarly, no such interactions were reported in other studies [6, 12, 13].
The observed association between faster weight gain in childhood and type 2 diabetes risk, especially the relatively stronger association in early childhood, agrees with findings from a study of female nurses in the USA, although in that study childhood adiposity was assessed by recall of somatotypes or pictorial diagrams [14]. By contrast, our findings differ from those of the Bogalusa Heart study in which weight gain in adolescence (age 10–19 years) and not in pre-adolescence (5–9 years) significantly associated with the prevalence of prediabetes or type 2 diabetes in adulthood [12]. In a Swedish study, weight change from ages 2–11 years significantly associated with type 2 diabetes (OR 1.20) but not impaired glucose tolerance in adulthood (1.06), and the association was weaker when these outcomes were combined (1.12) [15]. Similarly, there was no significant association between weight gain in early childhood and the prevalence of hyperglycaemia in other studies [16, 17]. The contrasting results may be due to the difference in analytical approach. In our study, risk was evaluated from childhood based on the time at risk of diabetes whereas in other studies [16, 17] risk was evaluated based on diabetes prevalence in adulthood. Given that individuals with faster weight gain in early childhood are more likely to develop type 2 diabetes before adulthood, the association between weight gain in childhood and type 2 diabetes risk is more efficiently estimated if based on time at risk. In some studies [15, 17,18,19], weight was adjusted for, or weight gain was calculated from, adult weight obtained close to the time of type 2 diabetes ascertainment rather than measures that clearly preceded type 2 diabetes onset, thereby making reliable comparison with our estimates difficult. Concurrent weight, being closer to diabetes diagnosis, usually accounts for most of the variability in type 2 diabetes incidence thereby weakening the association of weight variables preceding diabetes incidence.
Implications for clinicians, policy makers and future research
This study identifies higher weight and faster weight change in pre-adolescence to be associated with the greatest type 2 diabetes incidence. A possible explanation for this finding might be that children who attained a higher weight, or gained weight excessively during pre-adolescence, are exposed to an adiposity-induced chronic inflammatory state for a longer duration, thereby increasing their metabolic risk. Indeed, for participants representing more than one growth period, the high correlations in their longitudinal weights suggests that participants who were heavier in pre-adolescence were also heavier in adolescence (i.e. weight tracked from younger to older ages), in agreement with a previous report [21]. Longer duration of obesity increases type 2 diabetes incidence both in the current study population [34] and in a nationally representative sample [35]. Therefore, the strong association of excess weight, regardless of the period attained, with greater type 2 diabetes incidence, coupled with the weaker association of weight velocities in early and late adolescence with later type 2 diabetes risk, suggests that excess weight-related type 2 diabetes risk is driven largely by greater weight velocity pre-adolescence and the effect of continuing weight gain thereafter.
Physiological ‘adiposity rebound’ (a second rise in BMI) occurs during pre-adolescence. Although we did not assess the age at which this occurred in the current participants, others have shown an association between early onset of adiposity rebound and metabolic dysfunction including diabetes [36, 37]. Pre-pubertal adiposity could elicit an early rise in insulin resistance before the expression of physical and biochemical changes typically associated with puberty, thereby increasing the risk for type 2 diabetes [38].
Pre-adolescence is an important growth period for preventing and managing obesity and reducing the incidence of type 2 diabetes. Lifestyle interventions aimed at weight loss and increased physical activity reduce the incidence of type 2 diabetes in adults [39]. Similar interventions for weight management in children and adolescents might be effective in preventing type 2 diabetes, although this hypothesis has not yet, to our knowledge, been tested.
Data availability
Owing to privacy concerns of the small population of volunteers, data are not available for distribution.
Abbreviations
- IRR:
-
Incidence rate ratio
References
Cunningham SA, Kramer MR, Narayan KMV (2014) Incidence of childhood obesity in the United States. N Engl J Med 370(5):403–411. https://doi.org/10.1056/NEJMoa1309753
Skinner AC, Skelton JA (2014) Prevalence and trends in obesity and severe obesity among children in the United States, 1999-2012. JAMA Pediatr 168(6):561–566. https://doi.org/10.1001/jamapediatrics.2014.21
Skinner AC, Perrin EM, Moss LA, Skelton JA (2015) Cardiometabolic risks and severity of obesity in children and young adults. N Engl J Med 373(14):1307–1317. https://doi.org/10.1056/NEJMoa1502821
Mayer-Davis EJ, Lawrence JM, Dabelea D et al (2017) Incidence trends of type 1 and type 2 diabetes among youths, 2002–2012. N Engl J Med 376(15):1419–1429. https://doi.org/10.1056/NEJMoa1610187
Guo SS, Wu W, Chumlea WC, Roche AF (2002) Predicting overweight and obesity in adulthood from body mass index values in childhood and adolescence. Am J Clin Nutr 76(3):653–658. https://doi.org/10.1093/ajcn/76.3.653
Bjerregaard LG, Jensen BW, Angquist L, Osler M, Sorensen TIA, Baker JL (2018) Change in overweight from childhood to early adulthood and risk of type 2 diabetes. N Engl J Med 378(14):1302–1312. https://doi.org/10.1056/NEJMoa1713231
Tanamas SK, Reddy SP, Chambers MA et al (2018) Effect of severe obesity in childhood and adolescence on risk of type 2 diabetes in youth and early adulthood in an American Indian population. Pediatr Diabetes 19(4):622–629. https://doi.org/10.1111/pedi.12627
Constantino MI, Molyneaux L, Limacher-Gisler F et al (2013) Long-term complications and mortality in young-onset diabetes: type 2 diabetes is more hazardous and lethal than type 1 diabetes. Diabetes Care 36(12):3863–3869. https://doi.org/10.2337/dc12-2455
Al-Saeed AH, Constantino MI, Molyneaux L et al (2016) An inverse relationship between age of type 2 diabetes onset and complication risk and mortality: the impact of youth-onset type 2 diabetes. Diabetes Care 39(5):823–829. https://doi.org/10.2337/dc15-0991
Crowther NJ, Cameron N, Trusler J, Gray IP (1998) Association between poor glucose tolerance and rapid post natal weight gain in seven-year-old children. Diabetologia 41(10):1163–1167. https://doi.org/10.1007/s001250051046
Bhargava SK, Sachdev HS, Fall CH et al (2004) Relation of serial changes in childhood body-mass index to impaired glucose tolerance in young adulthood. N Engl J Med 350(9):865–875. https://doi.org/10.1056/NEJMoa035698
Zhang T, Xu J, Li S et al (2019) Trajectories of childhood BMI and adult diabetes: the Bogalusa Heart Study. Diabetologia 62(1):70–77. https://doi.org/10.1007/s00125-018-4753-5
Zimmermann E, Bjerregaard LG, Gamborg M, Vaag AA, Sorensen TIA, Baker JL (2017) Childhood body mass index and development of type 2 diabetes throughout adult life-a large-scale danish cohort study. Obesity 25(5):965–971. https://doi.org/10.1002/oby.21820
Yeung EH, Zhang C, Louis GM, Willett WC, Hu FB (2010) Childhood size and life course weight characteristics in association with the risk of incident type 2 diabetes. Diabetes Care 33(6):1364–1369. https://doi.org/10.2337/dc10-0100
Eriksson JG, Osmond C, Kajantie E, Forsen TJ, Barker DJ (2006) Patterns of growth among children who later develop type 2 diabetes or its risk factors. Diabetologia 49(12):2853–2858. https://doi.org/10.1007/s00125-006-0459-1
Wibaek R, Vistisen D, Girma T et al (2019) Body mass index trajectories in early childhood in relation to cardiometabolic risk profile and body composition at 5 years of age. Am J Clin Nutr 110(5):1175–1185. https://doi.org/10.1093/ajcn/nqz170
Norris SA, Osmond C, Gigante D et al (2012) Size at birth, weight gain in infancy and childhood, and adult diabetes risk in five low- or middle-income country birth cohorts. Diabetes Care 35(1):72–79. https://doi.org/10.2337/dc11-0456
Park MH, Sovio U, Viner RM, Hardy RJ, Kinra S (2013) Overweight in childhood, adolescence and adulthood and cardiovascular risk in later life: pooled analysis of three british birth cohorts. PLoS One 8(7):e70684. https://doi.org/10.1371/journal.pone.0070684
Juonala M, Magnussen CG, Berenson GS et al (2011) Childhood adiposity, adult adiposity, and cardiovascular risk factors. N Engl J Med 365(20):1876–1185. https://doi.org/10.1056/NEJMoa1010112
Pavkov ME, Hanson RL, Knowler WC, Bennett PH, Krakoff J, Nelson RG (2007) Changing patterns of type 2 diabetes incidence among Pima Indians. Diabetes Care 30(7):1758–1763. https://doi.org/10.2337/dc06-2010
Vijayakumar P, Wheelock KM, Kobes S et al (2018) Secular changes in physical growth and obesity among southwestern American Indian children over four decades. Pediatr Obes 13(2):94–102. https://doi.org/10.1111/ijpo.12199
Pavkov ME, Bennett PH, Knowler WC, Krakoff J, Sievers ML, Nelson RG (2006) Effect of youth-onset type 2 diabetes mellitus on incidence of end-stage renal disease and mortality in young and middle-aged Pima Indians. JAMA 296(4):421–426. https://doi.org/10.1001/jama.296.4.421
Dabelea D, Palmer JP, Bennett PH, Pettitt DJ, Knowler WC (1999) Absence of glutamic acid decarboxylase antibodies in Pima Indian children with diabetes mellitus. Diabetologia 42(10):1265–1266. https://doi.org/10.1007/s001250051303
Knowler WC, Bennett PH, Bottazzo GF, Doniach D (1979) Islet cell antibodies and diabetes mellitus in Pima Indians. Diabetologia 17(3):161–164. https://doi.org/10.1007/BF01219743
Sawyer SM, Azzopardi PS, Wickremarathne D, Patton GC (2018) The age of adolescence. Lancet Child Adolesc Health 2(3):223–228. https://doi.org/10.1016/S2352-4642(18)30022-1
Thearle MS, Muller YL, Hanson RL et al (2012) Greater impact of melanocortin-4 receptor deficiency on rates of growth and risk of type 2 diabetes during childhood compared with adulthood in Pima Indians. Diabetes 61(1):250–257. https://doi.org/10.2337/db11-0708
WHO Study Group on Diabetes Mellitus, World Health Organization (1985) Diabetes mellitus: report of a WHO study group: diabetes mellitus. World Health Organization, Geneva
Araujo J, Ramos E, Mishra GD, Severo M (2019) The use of weight adjusted for height rather than body mass index to assess growth trajectory: results from a population-based cohort. Stat Med 38(5):855–865. https://doi.org/10.1002/sim.8007
Oldham PD (1962) A note on the analysis of repeated measurements of the same subjects. J Chronic Dis 15(10):969–977. https://doi.org/10.1016/0021-9681(62)90116-9
Blomqvist N (1977) On the relation between change and initial value. J Am Stat Assoc 72:746–749
Puth M-T, Neuhauser M, Ruxton GD (2015) On the variety of methods for calculating confidence intervals by bootstrapping. J Anim Ecol 84(4):892–897. https://doi.org/10.1111/1365-2656.12382
Howe LD, Tilling K, Matijasevich A et al (2016) Linear spline multilevel models for summarising childhood growth trajectories: a guide to their application using examples from five birth cohorts. Stat Methods Med Res 25(5):1854–1874. https://doi.org/10.1177/0962280213503925
Olaiya MT, Wedekind LE, Hanson RL et al (2019) Birthweight and early-onset type 2 diabetes in American Indians: differential effects in adolescents and young adults and additive effects of genotype, BMI and maternal diabetes. Diabetologia 62(9):1628–1637. https://doi.org/10.1007/s00125-019-4899-9
Everhart JE, Pettitt DJ, Bennett PH, Knowler WC (1992) Duration of obesity increases the incidence of NIDDM. Diabetes 41(2):235–240. https://doi.org/10.2337/diab.41.2.235
The NS, Richardson AS, Gordon-Larsen P (2013) Timing and duration of obesity in relation to diabetes: findings from an ethnically diverse, nationally representative sample. Diabetes Care 36(4):865–872. https://doi.org/10.2337/dc12-0536
Eriksson JG, Forsén T, Tuomilehto J, Osmond C, Barker DJ (2003) Early adiposity rebound in childhood and risk of type 2 diabetes in adult life. Diabetologia 46(2):190–194. https://doi.org/10.1007/s00125-002-1012-5
Rolland-Cachera MF, Deheeger M, Maillot M, Bellisle F (2006) Early adiposity rebound: causes and consequences for obesity in children and adults. Int J Obes 30(S4):S11–S17. https://doi.org/10.1038/sj.ijo.0803514
Jeffery AN, Metcalf BS, Hosking J, Streeter AJ, Voss LD, Wilkin TJ (2012) Age before stage: insulin resistance rises before the onset of puberty: a 9-year longitudinal study (EarlyBird 26). Diabetes Care 3:536–541
Knowler WC, Barrett-Connor E, Fowler SE et al (2002) Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med 346(6):393–403. https://doi.org/10.1056/NEJMoa012512
Acknowledgements
We are grateful to the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) Phoenix clinic staff and to the residents of the Gila River Indian Community in Arizona for their participation in the study.
Authors’ relationships and activities
The authors declare that there are no relationships or activities that might bias, or be perceived to bias, this work.
Funding
This work was supported by the Intramural Research Program of the National Institute of Diabetes and Digestive and Kidney Diseases.
Author information
Authors and Affiliations
Contributions
MTO contributed to the conception and design of the study, analysed and interpreted data and prepared the first draft of the manuscript. WCK contributed to the conception and design of the study and acquisition, analysis and interpretation of data. RLH contributed to the acquisition, analysis and interpretation of data. SK contributed to the analysis and interpretation of data. RGN, LJB and YLM contributed to the acquisition and interpretation of data. MS contributed to the conception and design of the study and interpretation of data. All authors have read the manuscript, revised it for intellectual content and approved the final version. WCK is the guarantor of this work.
Corresponding author
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
ESM
(PDF 306 kb)
Rights and permissions
About this article

Cite this article
Olaiya, M.T., Knowler, W.C., Sinha, M. et al. Weight tracking in childhood and adolescence and type 2 diabetes risk. Diabetologia 63, 1753–1763 (2020). https://doi.org/10.1007/s00125-020-05165-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00125-020-05165-w