
Abstract
Aims/hypothesis
ANKRD26 is a newly described gene located at 10p12 in humans, a locus that has been identified with some forms of hereditary obesity. Previous studies have shown that partial inactivation of Ankrd26 in mice causes hyperphagia, obesity and gigantism. Hypothesising that Ankrd26 mutant (MT) mice could develop diabetes, we sought to establish whether the observed phenotype could be (1) solely related to the development of obesity or (2) caused by a direct action of ankyrin repeat domain 26 (ANKRD26) in peripheral tissues.
Methods
To test the hypothesis, we did a full metabolic characterisation of Ankrd26 MT mice that had free access to chow or were placed under two different energy-restricted dietary regimens.
Results
Highly obese Ankrd26 MT mice developed an unusual form of diabetes in which white adipose tissue is insulin-sensitive, while other tissues are insulin-resistant. When obese MT mice were placed on a food-restricted diet, their weight and glucose homeostasis returned to normal. In addition, when young MT mice were placed on a pair-feeding diet with normal mice, they maintained normal body weight, but showed better glucose tolerance than normal mice, an increased responsiveness of white adipose tissue to insulin and enhanced phosphorylation of the insulin receptor.
Conclusions/interpretation
These findings show that the ANKRD26 protein has at least two functions in mice. One is to control the response of white adipose tissue to insulin; the other is to control appetite, which when Ankrd26 is mutated, leads to hyperphagia and diabetes in an obesity-dependent manner.
Similar content being viewed by others


Introduction
Type 2 diabetes is the most common type of diabetes and accounts for 90% of all forms of the disease. It is a heterogeneous syndrome that is due to the interaction of environmental factors with genetic susceptibility to the disease [1] and is characterised by insulin resistance and/or abnormal insulin secretion, either of which may predominate [2]. The prevalence of type 2 diabetes is rapidly increasing worldwide and is expected to affect approximately 366 million people by 2030 [1]. Obesity is a major risk factor for the development of type 2 diabetes. Indeed, type 2 diabetes is most common in people who are older than 45 and overweight; as a consequence of increased obesity among young people, it is also becoming more common in children and young adults [3]. The term ‘diabesity’ has been coined to denote diabetes occurring in the context of obesity [4] and describes one of the main threats to human health in the twenty-first century [5].
We recently described a new model of obesity resulting from partial inactivation of Ankrd26 gene [6], which is located at 10p12 in humans, a genetic locus related to some forms of hereditary obesity [7]. The gene encodes a ~190 kDa protein that is highly abundant in the hypothalamus and other regions of the brain, as well as in many tissues and organs, including liver, skeletal muscle and white adipose tissue (WAT) (T.K. Bera and I. Pastan, unpublished data). The ankyrin repeat domain 26 (ANKRD26) protein is associated with the inner aspect of the cell membrane, and contains ankyrin repeats and spectrin helices, motifs known to interact with signalling proteins [6]. Mice with inactivation of Ankrd26 have marked hyperphagia, which results in extreme obesity and an increase in body length [6]. They also have high leptin levels, suggesting a defect in the feeding centres in the brain.
In the present work, we sought to establish whether these Ankrd26 mutant (MT) mice develop diabetes and whether the observed phenotype is solely related to the development of obesity or is caused by a direct action of ANKRD26 in peripheral tissues.
Methods
Mouse models and energy restriction diets
Ankrd26 MT mice were backcrossed for eight generations on the C57/Bl6 background in the animal facility of the National Cancer Institute (NCI). Male Ankrd26 homozygous MT mice and their normal littermates (wild-type) were used for all studies. All procedures were conducted in accordance with National Institutes of Health (NIH) guidelines, as approved by the Animal Care and Use Committees of the NCI and the National Institute of Diabetes, Digestive and Kidney Diseases (NIDDK). Mice were housed one per cage on a 12 h light/dark cycle (lights on 06:00–18:00 hours) and had free access to water and food (FA) (NIH-07 diet, 11% energy from fat; Zeigler Brothers, Gardners, PA, USA) when not under energy restriction dietary regimens. For the food restriction (FR) diet experiment, 4-month-old wild-type (n = 12) and Ankrd26 MT (n = 12) mice were randomly assigned to two groups: FA and FR. We determined baseline daily food consumption by weighing the food provided and correcting for food not eaten, including spillage. FR was performed for 15 weeks, with each FR mouse receiving an allocation of food equal to 33% of the FA (baseline) daily consumption of MT mice (3 g of food). For the pair-feeding (PF) diet experiment, 4-week-old wild-type (n = 12) and Ankrd26 MT (n = 12) mice were randomly assigned to two groups: FA and PF. The PF was performed for a period of 6 months and each PF mouse received an allocation of food equal to the amount of food eaten the day before by the control FA group. For both diets, food was supplied twice a day from Monday to Friday, and once on Saturdays and Sundays. Weight gain and body length of individual mice were measured as described [6]. Biochemical assays were measured as reported in electronic supplementary material (ESM) Methods.
Glucose and insulin tolerance, assessment of insulin and glucagon secretion, hyperinsulinaemic–euglycaemic clamps
The glucose tolerance test (GTT), insulin tolerance test (ITT) and insulin secretion were performed or measured as described [8], as was measurement of glucagon secretion [9]. Hyperinsulinaemic–euglycaemic clamps were also performed as previously described [10] and reported in the ESM Methods.
In vivo analysis of insulin signalling
Mice were fasted overnight, anaesthetised and injected i.p. with saline or insulin (10 U/kg body weight). At 10 min after injection, muscle, adipose tissue and liver were removed and frozen in dry ice. Tissues, homogenates and cell lysates were separated by SDS-PAGE and analysed by western blot as previously described [8,11,12]. Membranes were probed with antibodies to phospho-IGF-I receptor beta (Tyr1135/1136)/insulin receptor beta (Tyr1150/1151), insulin receptor beta, phospho-Akt (Ser473) and Akt (Cell Signaling Technology, Danvers, MA, USA).
Statistical analysis
Data are expressed as means ± SEM and statistical significance between groups was analysed by two-tailed Student’s t test or ANOVA as appropriate. Values of p < 0.05 were considered statistically significant. The total AUC and the inverse AUC for glucose response during GTT and ITT were calculated using the following equations [13]:
Results
Ankrd26 MT mice develop diabetes
To investigate the role of Ankrd26 in the regulation of glucose homeostasis in vivo, we did a full metabolic characterisation of the Ankrd26 MT mice. As reported previously [6], male Ankrd26 MT mice were heavier and longer than age-matched controls (wild-type) at 2, 4 and 6 months (Table 1), and their daily food intake was 40% higher (wild-type 3.5 ± 0.1 g/day; Ankrd26 MT 5.0 ± 0.1 g/day; p < 0.001). At 2 months of age, Ankrd26 MT mice exhibited a slight increase of fasting and random fed blood glucose levels (Table 1), but with normal GTT (Fig. 1a, b). By contrast, fasting and random fed blood glucose levels rose in the following months reaching a fasting level of 11.1 mmol/l at 6 months (Table 1). At 4 months of age, glucose loading (2 g/kg body weight) made Ankrd26 MT mice significantly more hyperglycaemic than control mice during the following 120 min (Fig. 1e, f), with glucose tolerance in the former being severely deteriorated at 6 months (Fig. 1i, j). This shows that partial inactivation of Ankrd26 can lead to diabetes. Interestingly, the obese MT mice had elevated fasting insulin and leptin levels, yet there were no significant differences in fasting NEFA and triacylglycerol concentrations at 2, 4 and 6 months (Table 1).

Glucose tolerance, insulin sensitivity, and insulin and glucagon secretion in Ankrd26 MT mice. Ankrd26 MT (grey squares/lines) and wild-type (black circles/lines) mice were subjected to GTT at (a, b) 2 months, (e, f) 4 months and (i, j) 6 months. Mice were fasted for 16 h and subjected to i.p. glucose loading (2 g/kg body weight). Blood glucose levels were determined at various times. b, f, j Mean AUC glucose from GTT. c, d Mice as above underwent ITT at 2 months, (g, h) 4 months and (k, l) 6 months. Random fed mice were injected i.p. with insulin (0.75 U/kg body weight), followed by determination of blood glucose levels at the indicated times. d, h, l Mean AUC insulin from ITT. m Glucose-induced insulin secretion was evaluated in 6-month-old MT and wild-type mice. Mice were fasted overnight and then injected i.p. with glucose (3 g/kg body weight). Serum insulin concentrations were measured at the indicated times by ELISA. For experiments (a–m) values are expressed as means ± SEM of determinations in at least ten mice per group. n Glucagon secretion was evaluated in 6-month-old random fed mice as above (m). Mice were injected i.p. with insulin (0.75 U/kg body weight). Plasma glucagon concentrations were measured by RIA before and 30 min after the insulin injection. Bars represent the means ± SEM of determinations in five MT and six control mice. *p < 0.05, **p < 0.01 and ***p < 0.001 vs wild-type
Ankrd26 MT mice show impaired insulin sensitivity and pancreatic function
To verify whether Ankrd26 inactivation is accompanied by reduced insulin sensitivity, we performed an ITT. Following i.p. injection of insulin (0.75 U/kg body weight) a slight reduction of the hypoglycaemic response was observed in Ankrd26 MT mice at 2 and 4 months (Fig. 1c, d, g, h), and this response was almost abolished in 6-month-old Ankrd26 MT mice (Fig. 1k, l). This shows that a time-dependent deterioration of insulin sensitivity occurred in the MT mice.
To assess pancreatic function, we evaluated glucose-induced insulin secretion and insulin-induced glucagon secretion. In control mice, a threefold increase in insulin secretion was observed 3 min after glucose injection (3 g/kg body weight), with levels remaining higher than baseline for up to 30 min, indicating a second-phase response (Fig. 1m). Plasma glucagon levels in control mice were also significantly increased by the hypoglycaemic response induced by insulin (0.75 U/kg body weight; Fig. 1n). In contrast, the acute first-phase insulin secretory response to glucose and the late second-phase response were completely abolished in Ankrd26 MT mice (Fig. 1m). In addition, a defective glucagon response to hypoglycaemia was observed (Fig. 1n), indicating the concomitant presence of impaired insulin and glucagon secretion.
Hyperinsulinaemic–euglycaemic clamp in Ankrd26 MT mice
To analyse glucose metabolism and insulin sensitivity of Ankrd26 MT mice in more detail, we performed a hyperinsulinaemic–euglycaemic clamp. In the basal state, Ankrd26 MT mice had significantly increased plasma glucose (Fig. 2a). During the clamp, the glucose infusion rate (GIR) needed to maintain euglycaemia and also the whole-body glucose disposal rate (R d) were significantly decreased in Ankrd26 MT mice, indicating the presence of whole-body insulin resistance (Fig. 2b–d). We also evaluated endogenous glucose production (EGP) and glucose uptake in the peripheral tissues. Insulin was not able to suppress EGP in Ankrd26 MT mice (Fig. 2e), indicating hepatic insulin resistance. In addition, glucose uptake in skeletal muscle and brown adipose tissue (BAT) was significantly decreased (Fig. 2f, g), but surprisingly there was no significant difference in glucose uptake by WAT (Fig. 2h).

Hyperinsulinaemic–euglycaemic clamp studies in 7-month-old Ankrd26 MT (grey squares/columns) and wild-type (WT; black squares/columns) mice were performed as described. a Glucose levels, (b, c) GIR and (d) R d during the clamp procedure. e Basal EGP (monotone bars) and EGP (hatched bars) during the clamp. f Glucose uptake into skeletal muscle, (g) BAT and (h) WAT during the clamp. Values are expressed as means ± SEM of determinations in at least eight mice per group. **p < 0.01 and ***p < 0.001 vs wild-type. BW, body weight
In vivo insulin signalling in Ankrd26 MT mice
To evaluate at the signalling level whether the progression of whole-body insulin resistance is related to the age of the mice, we injected i.p. insulin (10 U/kg body weight) into 2- and 6-month-old fasted Ankrd26 MT and control mice, and assessed activation of the insulin signalling pathway in liver, skeletal muscle and WAT by western blot. In 2-month-old MT mice the insulin-stimulated phosphorylation of insulin receptor beta on Tyr 1150/1151 and of Akt on Ser473 was comparable to that in wild-type mice in liver and skeletal muscle, and increased vs wild-type in WAT (Fig. 3a–f), indicating that insulin signalling in MT mice was generically intact. On the other hand, in 6-month-old Ankrd26 MT mice, the insulin-induced phosphorylation of insulin receptor beta and Akt was markedly reduced in liver and skeletal muscle (Fig. 3g, h, j, k). However, in WAT the insulin response was still slightly increased compared with normal mice (Fig. 3i, l), confirming the observation in clamp studies that WAT remained insulin-responsive.

Insulin signalling in Ankrd26 MT mice. In vivo insulin signalling in liver (a, d, g, j), tibialis skeletal muscle (b, e, h, k) and epididymal WAT (c, f, i, l) of 2-month-old (a–f) and 6-month-old (g–l) overnight-fasted MT mice that had been i.p. injected (+, dark grey) or not (−, light grey) with insulin (10 U/kg body weight) 10 min before determination along with wild-type (WT) counterparts; black, injected wild-type (WT); white, non-injected WT. The corresponding blots show levels of total and tyrosine (Tyr 1150/1151) phosphorylated forms of insulin receptor (IR), and of total and serine (Ser473) phosphorylated forms of Akt in mice as indicated. Each blot is representative of three independent experiments. Bars in graphs are expressed as means ± SEM in at least six mice per group. *p < 0.05 and ***p < 0.001 for MT + insulin vs wild-type + insulin
Food restriction diet normalises body weight and glucose tolerance in Ankrd26 MT mice
To determine whether the insulin resistance and impairment of insulin secretion that led to the onset of diabetes in Ankrd26 MT mice were secondary to the development of obesity, we analysed glucose homeostasis of MT mice under two different energy-restricted feeding regimens (FR diet, PF diet).
First, to observe whether the impairment of glucose tolerance could be reversed by the dietary treatment, FR was performed for 15 weeks in 4-month-old obese and glucose-intolerant Ankrd26 MT and in age-matched lean wild-type mice, all of which received 3 g food daily. After 1 month, Ankrd26 MT mice on the FR diet showed a 15% reduction of body weight and a 60% reduction of fasting leptin levels compared with starting values (ESM Table 1, ESM Fig. 1a). This decrease in body weight in Ankrd26 MT mice was accompanied by a significant decrease of fasting and random fed blood glucose levels, as well as of fasting insulin and NEFA levels, with values comparable to those of wild-type mice (ESM Table 1). Glucose levels during GTT performed after 2 months of diet were significantly lower in Ankrd26 MT mice than before FR; indeed, glycaemia was even lower than in controls, indicating higher glucose disposal (ESM Fig. 1b–e). In addition, FR Ankrd26 MT mice had a near normal response to insulin with values comparable to those of wild-type mice (ESM Fig. 1f–i), while their insulin response to glucose injection became the same as that of normal mice (ESM Fig. 1j).
Pair-feeding diet maintains normal body weight and improves glucose tolerance in Ankrd26 MT mice
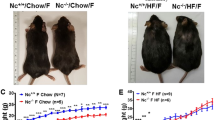
To determine whether an impairment of glucose tolerance could occur in lean Ankrd26 MT mice, PF was performed for 6 months in 4-week-old Ankrd26 MT and wild-type mice; the former were fed daily the amount of food eaten on the previous day by the control group. At 2 and 4 months, PF Ankrd26 MT mice were slightly heavier than PF age-matched control mice, but no significant differences in body weight and fasting leptin were observed at 6 months (Table 2, Fig. 4a). Interestingly, these MT mice with normal body weight had the same body length as the corresponding wild-type mice, indicating that the change in length is dependent on some factor that is present only in obese MT mice (Table 2, ESM Fig. 2). At the age of 2, 4 and 6 months, PF Ankrd26 MT mice had fasting and random fed blood glucose levels, as well as fasting insulin levels within the normal range of control mice (Table 2). In contrast, they had a slight decrease of NEFA and triacylglycerol levels compared with wild-type mice (Table 2). Glucose levels during GTT performed in 2-month-old mice were significantly decreased in PF Ankrd26 MT mice compared with those in wild-type mice. This decrease was also present in 4- and 6-month-old MT mice, indicating the presence of improved glucose tolerance (Fig. 4b–g). Injection of insulin evoked a comparable reduction of hypoglycaemic responses in PF Ankrd26 MT and wild-type mice at 2, 4 and 6 months (Fig. 4h–m); in addition, the glucose-induced insulin secretion profile was comparable between PF MT and control mice (Fig. 4n). All these data from both energy-restricted feeding regimens demonstrate that the severe impairment of glucose tolerance induced by partial inactivation of Ankrd26 is secondary to obesity. Thus, in mice on an energy-restricted diet the inactivation of this gene does not impair glucose homeostasis, but, instead, seems to improve it.

Body weight, glucose tolerance, insulin sensitivity and insulin secretion in PF Ankrd26 MT mice. a Growth curve of MT mice subjected to FA diet (dark grey squares) and PF diet (light grey squares), and of wild-type mice subjected to FA (black circles) PF (grey circles). b GTT with (c) AUC glucose in 2-month-old, 4-month-old (d, e) and 6-month-old (f, g) PF MT and PF wild-type mice. c, e, g MT, grey columns; wild-type, black columns. h ITT with (i) AUC insulin in 2-month-old, (j, k) 4-month-old and (l, m) 6-month-old random fed PF MT and PF wild-type mice. i, k, m MT, grey columns; wild-type, black columns. For each experiment, values are expressed as means ± SEM of determinations in at least six mice per group. n Glucose-induced insulin secretion in 6-month-old PF MT (grey) and PF wild-type mice (black). Data points represent the means ± SEM of determinations in four MT and five control mice. *p < 0.05, **p < 0.01 and ***p < 0.001 vs PF wild-type
Improved WAT insulin sensitivity in Ankrd26 MT mice on energy-restricted diet
We performed hyperinsulinaemic–euglycaemic clamps in Ankrd26 MT mice under the two different food-intake regimens. During the clamp, FR and PF Ankrd26 MT mice had glucose levels, GIR, R d and insulin suppression of EGP comparable to the values of their respective controls (Fig. 5a–e, ESM Fig. 3a–e). In addition, insulin-stimulated glucose uptake in skeletal muscle and in BAT in MT mice on the energy-restricted diet was similar to that in controls (Fig. 5f, g, ESM Fig. 3f, g); interestingly, insulin-stimulated glucose uptake was increased in WAT (Fig. 5h, ESM Fig. 3h).

Hyperinsulinaemic–euglycaemic clamp studies were performed in 7-month-old MT (grey squares/grey columns) and wild-type (WT; grey circles/black column) mice on PF. a Glucose levels, (b, c) GIR and (d) during the clamp procedure. e Basal EGP (monotone columns) and EGP during the clamp (hatched columns). f Glucose uptake into skeletal muscle, (g) BAT and (h) WAT during the clamp. Values are expressed as means ± SEM of determinations in at least five mice per group. *p < 0.05 and ***p < 0.001 vs PF wild-type. BW, body weight
Improved WAT insulin signalling in Ankrd26 MT mice on energy-restricted diet
Consistent with these data was our finding that, in PF Ankrd26 MT mice, phosphorylated insulin receptor beta and Akt levels in response to insulin were comparable to those of wild-type mice in the liver and skeletal muscle and higher than those of wild-type mice in WAT (Fig. 6a–f). Similar data were obtained in FR Ankrd26 MT mice (ESM Fig. 4a–e). Altogether these data identify WAT as the site responsible for the improvement of glucose tolerance in lean Ankrd26 MT mice, indicating a role for this gene in the regulation of insulin sensitivity in adipocytes, as well as in control of appetite in the brain.

In vivo insulin-signalling in liver (a, d), tibialis skeletal muscle (b, e) and epididymal WAT (c, f) of 6-month-old overnight-fasted MT and wild-type (WT) mice under PF feeding regimens that had been i.p. injected (+, dark grey and black columns) or not (−, light grey and white columns) with insulin (10 U/kg body weight) 10 min before determination. The corresponding blots show the levels of total and tyrosine (Tyr 1150/1151) phosphorylated forms of the insulin receptor, and levels of total and serine (Ser473) phosphorylated forms of Akt in mice as indicated. The lanes were run on the same gel but were non-contiguous. Blots are representative of three independent experiments. Bars in graphs are expressed as means ± SEM in at least six mice per group. *p < 0.05 for MT + insulin vs wild-type + insulin
Discussion
In the present work, we report that MT mice with partial inactivation of Ankrd26 exhibited elevated fasting and random fed blood glucose levels, and developed diabetes when severely obese. MT mice were also markedly hyperinsulinaemic in the basal state, showed a poor insulin response to a glucose challenge and a defective glucagon response to hypoglycaemia, and were also severely insulin-resistant upon ITT. These findings show that impaired insulin action and secretion contribute to the abnormal glucose tolerance produced by partial inactivation of Ankrd26. Further, hyperinsulinaemic–euglycaemic clamps and studies of insulin signalling in obese Ankrd26 MT mice demonstrated the onset of an unusual form of whole-body insulin resistance, in which WAT remained insulin-sensitive, while the other insulin target tissues became insulin-resistant. These results suggest that Ankrd26 has a role in the control of insulin sensitivity in WAT.
The pathogenesis of type 2 diabetes is known to be complex, involving not only heightened genetic susceptibility in certain ethnic groups, but also environmental and behavioural factors such as a sedentary lifestyle, nutrition and obesity [14]. To establish the role of obesity in the glycaemic disorders observed in Ankrd26 MT mice, we used two different restricted energy intake feeding strategies. In one approach mature obese MT mice were placed on a FR diet, since chronic moderate reduction in energy intake (~20–40%) results in weight loss and improves whole-body glucose homeostasis in humans, rats and mice by increasing peripheral insulin sensitivity and decreasing glycaemia, insulinaemia and leptinaemia [15–18]. We found that FR completely restored normal body weight in MT mice and improved glucose metabolism by normalising whole-body insulin sensitivity and preserving insulin secretion. FR MT mice also had increased insulin sensitivity in WAT.
In the other study, young MT mice were placed on a PF diet to prevent the onset of obesity and maintain body weight in a normal range [19]. We found that PF was sufficient to maintain normal body weight in MT mice; PF MT mice, moreover, had improved glucose tolerance, and normal insulin secretion and whole-body insulin sensitivity. Like the FR mice, they also showed increased glucose uptake in WAT. The onset of extreme obesity resulting from the marked hyperphagia of Ankrd26 MT mice therefore seems to be essential for the derangement of glucose homeostasis and for the development of diabetes, since impairment of glucose homeostasis was reversed by dietary regimen and did not occur in MT mice when their food intake and body weight were similar to those of control mice. Thus, Ankrd26 MT mice should be regarded as a good mouse model of obesity-induced diabetes. However, in marked contrast to other models of obesity and diabetes, such as leptin-deficient ob/ob mice, leptin receptor deficient db/db mice and yellow agouti MT mice [20], Ankrd26 MT mice have whole-body insulin resistance in the presence of normal insulin sensitivity in WAT, indicating that peripheral insulin resistance in liver, skeletal muscle and BAT, together with a dysfunction of beta cell function, is sufficient to impair glucose homeostasis in these mice when obese. Additionally, Ankrd26 MT mice under restricted energy intake regimens show better glucose tolerance than control mice, probably due to their increased insulin sensitivity in WAT. Indeed, during clamp experiments, insulin-stimulated glucose uptake was slightly higher in WAT of MT mice on an energy-restricted diet. An enhancement of glucose tolerance associated with increased glucose disposal in WAT has been described in several adipose tissue-specific transgenic mice [21–23]. For example, overproduction of the insulin-responsive glucose transporter, GLUT4, in WAT causes enhanced glucose tolerance and increased glucose uptake in adipose tissue and leads to an increase in fat cell number [21]. In these transgenic mice and, as with our mice, despite these marked effects at the adipose cell level, obesity induced by high fat feeding leads to a decrease in glucose tolerance due to insulin resistance in skeletal muscle and liver, where the Glut4 (also known as Slc2a4) transgene is not expressed [22]. An additional example is the overabundance of liver glucokinase in WAT, where the increase of glucose phosphorylation in adipocytes leads to enhanced glucose uptake and metabolism in WAT, thus improving glucose tolerance in vivo [23]. Therefore, an increase of glucose disposal in WAT could in itself be sufficient to improve glucose tolerance in MT mice on an energy-restricted diet.
In addition to improved glucose tolerance, Ankrd26 MT mice under both energy restriction regimens showed decreased levels of NEFA and triacylglycerol, while these lipid concentrations were in the normal range in obese Ankrd26 MT mice. WAT plays a crucial role in buffering the flux of fatty acids in the bloodstream. Insulin modulates this process, suppressing the release of NEFA into the circulation and increasing triacylglycerol storage in WAT [24]. Increased NEFA release by WAT and subsequent lipid abnormalities in type 2 diabetes are strongly associated with insulin resistance [24,25]. Thus, the observed decrease in NEFA and triacylglycerol concentrations in Ankrd26 MT mice on an energy-restricted diet could be explained by their increased insulin sensitivity in WAT.
We also observed an improvement of insulin signalling in WAT from these mice. Indeed, an evaluation of the insulin signalling cascade in WAT from FR and PF Ankrd26 MT mice showed increased tyrosine phosphorylation of the beta subunit of the insulin receptor [26] and increased phosphorylation of Akt, a serine/threonine kinase involved downstream of the insulin signalling [27]. We recently demonstrated that mouse embryonic fibroblast cells from Ankrd26 MT mice have a higher rate of spontaneous adipogenesis than wild-type mouse embryonic fibroblasts and that their adipogenesis is greatly increased when exposed to a mixture of inducers [28]. These findings indicate that Ankrd26 plays a prominent role in fat cells, regulating their differentiation and insulin sensitivity. Unfortunately, we do not yet know how ANKRD26 modulates insulin signalling and/or adipogenesis in fat cells. To detect proteins that interact with ANKRD26, we are now doing a yeast two hybrid screen.
In addition to obesity, Ankrd26 MT mice showed a 10% increase in linear growth even though circulating growth hormone and IGF1 are in the normal range [6]. Differences in body length were not detected in 4-week-old MT mice (ESM Fig. 2a), but were detected at 2 months of age in parallel with an increase in body weight and serum leptin levels. It is well established that longitudinal growth is regulated by growth hormone and its tissue mediator IGFI [29]. However, recent evidence indicates that signals regulating energy balance also regulate the somatotrophic axis. For example leptin can promote longitudinal growth, since impairment of leptin signalling causes reduced linear growth in ob/ob and db/db mice [30], and leptin administration is a potent stimulator of bone growth in ob/ob mice [31]. The hypothesis that leptin can play a crucial role in the increase of longitudinal growth in Ankrd26 MT mice is supported by our finding that PF MT mice with normal body weight and leptin levels had longitudinal growth comparable to controls at 2, 4 and 6 months of age (ESM Fig. 2a, b).
Defects in Ankrd26 expression or function play a critical role in controlling obesity in Ankrd26 MT mice, since its partial inactivation causes hyperphagia and extreme obesity, and does not cause a reduction in energy expenditure or activity [6]. The important role of hyperphagia is supported by our finding that MT mice with a post-weaning limitation of food intake had normal body composition (fat and lean mass; Table 2). ANKRD26 is highly abundant in several regions of the brain, including the arcuate, paraventricular and ventromedial nuclei of the hypothalamus [6], a region known to play a key role in regulation of feeding behaviour [32]. Moreover, obese Ankrd26 MT mice did not show decreased food intake and body weight in response to leptin (3 mg/kg body weight; data not shown), indicating the presence of a central leptin resistance. Therefore the obese phenotype of Ankrd26 MT mice is very likely to be due to a prominent role of ANKRD26 in the regulation of food intake in the brain. In support of this conclusion are the microarray analysis results obtained by Ko et al. [33], who found that Ankrd26 mRNA levels are increased in the hypothalamus of C57BL/6 mice after administration of three anti-obesity drugs (sibutramine, phendimetrazine, methamphetamine) that are known to suppress appetite by activating catecholaminergic neurotransmission [34–36]. These findings led the authors to suggest that Ankrd26 probably accounts for the biological effects of these drugs. However, the precise mechanism by which Ankrd26 controls food intake in MT mice is still not clear and is currently under investigation in our laboratory.
In summary, our results identify Ankrd26 MT mice as a new model of obesity-induced diabetes, since the inactivation of this gene in vivo can lead to diabetes by impairing insulin action and secretion in an obesity-dependent manner. Our results also identify Ankrd26 as a novel gene involved not only in the regulation of food intake, but also in the regulation of insulin responses in WAT. We propose that ANKRD26 could be an attractive molecular target for the generation of new anti-obesity and insulin-sensitising drugs.
Abbreviations
- ANKRD26:
-
Ankyrin repeat domain 26
- BAT:
-
Brown adipose tissue
- EGP:
-
Endogenous glucose production
- FA:
-
Free access to water and food
- FR:
-
Food restriction
- GIR:
-
Glucose infusion rate
- GTT:
-
Glucose tolerance test
- ITT:
-
Insulin tolerance test
- MT:
-
Mutant
- NCI:
-
National Cancer Institute
- NIDDK:
-
National Institute of Diabetes Digestive and Kidney Diseases
- NIH:
-
National Institutes of Health
- PF:
-
Pair-feeding
- R d :
-
Whole-body glucose disposal rate
- WAT:
-
White adipose tissue
References
No authors listed (2006) Diabetes Atlas 2006, 3rd edn. International Diabetes Federation, Brussels
Zimmet P, Alberti KG, Shaw J (2001) Global and societal implications of the diabetes epidemic. Nature 414:782–787
Fagot-Campagna A, Narayan K (2001) Type 2 diabetes in children. BMJ 322:377–387
Astrup A, Finer N (2000) Redefining type 2 diabetes: 'diabesity' or 'obesity dependent diabetes mellitus'? Obes Rev 1:57–59
Farag YM, Gaballa MR (2011) Diabesity: an overview of a rising epidemic. Nephrol Dial Transplant 26:28–35
Bera TK, Liu XF, Yamada M et al (2008) A model for obesity and gigantism due to disruption of the Ankrd26 gene. Proc Natl Acad Sci USA 105:270–275
Dong C, Li WD, Geller F et al (2005) Possible genomic imprinting of three human obesity-related genetic loci. Am J Hum Genet 76:427–437
Miele C, Raciti GA, Cassese A et al (2007) PED/PEA-15 regulates glucose-induced insulin secretion by restraining potassium channel expression in pancreatic beta-cells. Diabetes 56:622–633
Kawamori D, Kurpad AJ, Hu J et al (2009) Insulin signaling in alpha cells modulates glucagon secretion in vivo. Cell Metab 9:350–361
Ozcan U, Yilmaz E, Ozcan L et al (2006) Chemical chaperones reduce ER stress and restore glucose homeostasis in a mouse model of type 2 diabetes. Science 313:1137–1140
Guo T, Jou W, Chanturiya T, Portas J, Gavrilova O, McPherron AC (2009) Myostatin inhibition in muscle, but not adipose tissue, decreases fat mass and improves insulin sensitivity. PLoS One 4:e4937
Laemmli UK (1970) Cleavage of structural proteins during the assembly of the head of bacteriophage T4. Nature 227:680–685
Heikkinen S, Argmann CA, Champy MF, Auwerx J (2007) Evaluation of glucose homeostasis. Curr Protoc Mol Biol 29:Unit 29B.3
Zimmet P (1992) Kelly West Lecture 1991. Challenges in diabetes epidemiology—from West to the rest. Diabetes Care 15:232–252
Friedman JE, Dohm GL, Leggett-Frazier N et al (1992) Restoration of insulin responsiveness in skeletal muscle of morbidly obese patients after weight loss. Effect on muscle glucose transport and glucose transporter GLUT4. J Clin Invest 89:701–705
Kelley DE, Wing R, Buonocore C, Sturis J, Polonsky K, Fitzsimmons M (1993) Relative effects of calorie restriction and weight loss in noninsulin-dependent diabetes mellitus. J Clin Endocrinol Metab 77:1287–1293
Dean DJ, Gazdag AC, Wetter TJ, Cartee GD (1998) Comparison of the effects of 20 days and 15 months of calorie restriction on male Fischer 344 rats. Aging 10:303–307
Harris SB, Gunion MW, Rosenthal MJ, Walford RL (1994) Serum glucose, glucose tolerance, corticosterone and free fatty acids during aging in energy restricted mice. Mech Ageing Dev 73:209–221
Cleary MP, Vasselli JR, Greenwood MR (1980) Development of obesity in Zucker obese (fafa) rat in absence of hyperphagia. Am J Physiol 238:E284–E292
Carrolla L, Voisey J, van Daal A (2004) Mouse models of obesity. Clin Dermatol 22:345–349
Shepherd PR, Gnudi L, Tozzo E, Yang H, Leach F, Kahn BB (1993) Adipose cell hyperplasia and enhanced glucose disposal in transgenic mice overexpressing GLUT4 selectively in adipose tissue. J Biol Chem 268:22243–22246
Gnudi L, Tozzo E, Shepherd PR, Bliss JL, Kahn BB (1995) High level overexpression of glucose transporter-4 driven by an adipose-specific promoter is maintained in transgenic mice on a high fat diet, but does not prevent impaired glucose tolerance. Endocrinology 136:995–1002
Muñoz S, Franckhauser S, Elias I et al (2010) Chronically increased glucose uptake by adipose tissue leads to lactate production and improved insulin sensitivity rather than obesity in the mouse. Diabetologia 53:2417–2430
Howard B (1987) Lipoprotein metabolism in diabetes mellitus. J Lipid Res 28:613–628
Zoratti R, Godsland I, Chaturvedi N, Crook D, Stevenson J, McKeigue P (2000) Relation of plasma lipids to insulin resistance, non-esterified fatty acid levels and body fat in men from three ethnic groups: relevance to variation in risk of diabetes and coronary disease. Metabolism 49:245–252
Patti ME, Kahn CR (1998) The insulin receptor—a critical link in glucose homeostasis and insulin action. J Basic Clin Physiol Pharmacol 9:89–109
Farese RV, Sajan MP, Standaert ML (2005) Insulin-sensitive protein kinases (atypical protein kinase C and protein kinase B/Akt): actions and defects in obesity and type II diabetes. Exp Biol Med 230:593–605
Fei Z, Bera TK, Liu X, Xiang L, Pastan I (2011) ANKRD26 gene disruption enhances adipogenesis of mouse embryonic fibroblasts. J Biol Chem. doi:10.1074/jbc.M111.248435
Le Roith D, Bondy C, Yakar S, Liu JL, Butler A (2001) The somatomedin hypothesis: 2001. Endocr Rev 22:53–74
Erickson JC, Hollopeter G, Palmiter RD (1996) Attenuation of the obesity syndrome of ob/ob mice by the loss of neuropeptide Y. Science 274:1704–1707
Steppan CM, Crawford DT, Chidsey-Frink KL, Ke H, Swick AG (2000) Leptin is a potent stimulator of bone growth in ob/ob mice. Regul Pept 92:73–78
King BM (2006) The rise, fall, and resurrection of the ventromedial hypothalamus in the regulation of feeding behavior and body weight. Physiol Behav 87:221–244
Ko MJ, Choi HS, Ahn JI, Kim SY, Jeong HS, Chung HJ (2008) Gene expression profiling in C57BL/6 mice treated with the anorectic drugs Sibutramine and Phendimetrazine and their mechanistic implications. Genom Informat 6:117–125
Chen TY, Duh SL, Huang CC, Lin TB, Kuo DY (2001) Evidence for the involvement of dopamine D(1) and D(2) receptors in mediating the decrease of food intake during repeated treatment with amphetamine. J Biomed Sci 8:462–466
Seiden LS, Sabol KE, Ricaurte GA (1993) Amphetamine: effects on catecholamine systems and behavior. Annu Rev Pharmacol Toxicol 33:639–677
Stock MJ (1997) Sibutramine: a review of the pharmacology of a novel anti-obesity agent. Int J Obes Relat Metab Disord 21(Suppl 1):S25–S29
Acknowledgements
We thank W. Jou and T. Chanturiya (Mouse Metabolism Core, NIDDK) for invaluable technical support with the hyperinsulinaemic–euglycaemic clamp procedures. This research was supported in part by the Intramural Research Program of the NIH, the NCI, the Center for Cancer Research and in part by the NIDDK.
Contribution statement
GAR designed the study, researched data, contributed to the discussion, wrote the manuscript and gave the final approval of the version to be published. TKB researched data, contributed to the discussion and gave the final approval of the version to be published. OG researched data, contributed to the discussion and gave the final approval of the version to be published. IP designed the study, wrote the manuscript and gave the final approval of the version to be published.
Duality of interest
The authors declare that there is no duality of interest associated with this manuscript.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
ESM Methods
(PDF 74 kb)
ESM Table 1
Metabolic characteristics of food restricted Ankrd26 mutant mice (PDF 68 kb)
ESM Fig. 1
Body weight, glucose tolerance, insulin sensitivity and insulin secretion in FR Ankrd26 MT mice. a Growth curve of MT mice subjected to FA diet (dark grey squares) and FR diet (white squares), and of wild-type mice subjected to FA (black circles) and FR (white circles). b GTT with (c) AUC glucose in MT and wild-type mice before FR and 2 months after FR (d, e). c, e MT, grey columns; wild-type, black columns. f ITT with (g) AUC insulin in MT and wild-type mice before FR and 2 months after FR (h, i). g, i MT, grey columns; wild-type, black columns. For each experiment, values are expressed as means ± SEM of determinations in at least six mice per group. j Glucose-induced insulin secretion in 6-month-old FR MT (grey) and FR wild-type mice (black). Data points represent the means ± SEM of determinations in four MT and five control mice. *p < 0.05, **p < 0.01 and ***p < 0.001 vs FR wild-type (PDF 77 kb)
ESM Fig. 2
Body length and body weight in FA and PF Ankrd26 MT mice. Body length (a) and body weight (b) curve of MT and wild-type (WT) mice with free access to food (dark grey squares and black circles) and under PF (light grey squares and light gray circles). For each experiment, values are expressed as means ± SEM of determinations in at least six mice per group. Data points represent the means ± SEM of determinations in four MT and six control mice. *P < 0.05, ***P < 0.001 vs. PF wild-type (PDF 40 kb)
ESM Fig. 3
Hyperinsulinaemic-euglycaemic clamp studies were performed in 7-month-old MT (white squares/grey columns) and wild-type (WT; white circles/black column) mice on FR. a Glucose levels, (b, c) GIR and (d) during the clamp procedure e Basal EGP (monotone columns) and EGP during the clamp (hatched columns). f Glucose uptake into skeletal muscle, (g) BAT and (h) WAT during the clamp. Values are expressed as means ± SEM of determinations in at least five mice per group. *p < 0.05 and ***p < 0.001 vs FR wild-type. BW, body weight (PDF 46 kb)
ESM Fig. 4
In vivo insulin-signalling in liver (a, c), tibialis skeletal muscle (d) and epididymal WAT (b, e) of 6-month-old overnight-fasted MT and wild-type (WT) mice under FR feeding regimens that had been i.p. injected (+, dark grey and black columns) or not (−, light grey and white columns) with insulin (10 U/kg body weight) 10 min before determination. The corresponding blots show the levels of total and tyrosine (Tyr 1150/1151) phosphorylated forms of the insulin receptor, and levels of total and serine (Ser473) phosphorylated forms of Akt in mice as indicated. The lanes were run on the same gel but were non-contiguous. Blots are representative of three independent experiments. Bars in graphs are expressed as means ± SEM in at least six mice per group. *p < 0.05 for MT + insulin vs wild-type + insulin (PDF 350 kb)
Rights and permissions
About this article
Cite this article
Raciti, G.A., Bera, T.K., Gavrilova, O. et al. Partial inactivation of Ankrd26 causes diabetes with enhanced insulin responsiveness of adipose tissue in mice. Diabetologia 54, 2911–2922 (2011). https://doi.org/10.1007/s00125-011-2263-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00125-011-2263-9