
Abstract
Introduction
Hip fracture patients, who are often frail, continue to be a challenge for healthcare systems with a high postoperative mortality rate. While beta-blocker therapy (BBt) has shown a strong association with reduced postoperative mortality, its effect in frail patients has yet to be determined. This study’s aim is to investigate how frailty, measured using the Orthopedic Hip Frailty Score (OFS), modifies the effect of preadmission beta-blocker therapy on mortality in hip fracture patients.
Methods
This retrospective register-based study included all adult patients in Sweden who suffered a traumatic hip fracture and subsequently underwent surgery between 2008 and 2017. Treatment effect was evaluated using the absolute risk reduction (ARR) in 30-day postoperative mortality when comparing patients with (BBt+) and without (BBt-) ongoing BBt. Inverse probability of treatment weighting (IPTW) was used to reduce potential confounding when examining the treatment effect. Patients were stratified based on their OFS (0, 1, 2, 3, 4 and 5) and the treatment effect was also assessed within each stratum.
Results
A total of 127,305 patients were included, of whom 39% had BBt. When IPTW was performed, there were no residual differences in observed baseline characteristics between the BBt+ and BBt- groups, across all strata. This analysis found that there was a stepwise increase in the ARRs for each additional point on the OFS. Non-frail BBt+ patients (OFS 0) exhibited an ARR of 2.2% [95% confidence interval (CI) 2.0–2.4%, p < 0.001], while the most frail BBt+ patients (OFS 5) had an ARR of 24% [95% CI 18–30%, p < 0.001], compared to BBt- patients within the same stratum.
Conclusion
Beta-blocker therapy is associated with a reduced risk of 30-day postoperative mortality in frail hip fracture patients, with a greater effect being observed with higher Orthopedic Hip Frailty Scores.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Hip fracture patients comprise a significant challenge for health care systems globally. Owing to the high degree of frailty and considerable comorbidity burden in this population, they demand a substantial amount of resources both during their hospital stay and post discharge [1,2,3]. In 2010, an estimated 2.7 million people suffered a hip fracture, accounting for approximately 20% of all osteoporotic fractures in those who were 50 years or older [4,5,6]. This number is projected to continue to rise as the global population ages and life expectancy increases [7, 8]. With 6.3 million hip fractures yearly being predicted by 2050 [9], an even greater strain will be placed on hospital and public resources, necessitating a robust strategy to manage this increased demand [1, 10,11,12,13]. However, hip fracture patients are a heterogenous population, wherein specific subgroups are disproportionately culpable for the high mortality rates observed [14,15,16,17].
Frailty plays a particular role in the high rates of postoperative mortality observed in hip fracture patients, with up to 27% of patients dying within the first year after surgery [15, 17]. Frailty, defined as a reduced ability to adapt to external stressors due to a reduced physiological reserve [18,19,20,21], is relatively common in hip fracture patients; rates vary between one fifth and half of hip fracture patients depending on the method used for measuring it [22,23,24,25,26]. Nevertheless, there is a distinct lack of tools tailored to helping this vulnerable cohort, once a patient has been identified as frail [27, 28]. Besides selection of operative technique, when fracture morphology allows for it [29, 30], the chief potential intervention has been orthogeriatric care models [31,32,33]. However, these models tend to include patients based on chronological age, rather than biological age or degree of frailty, which might not always be optimal [34,35,36,37]. Consequently, more options are required in order to adapt care to those who are most frail.
Beta-blocker therapy (BBt) has previously been associated with reduced mortality in hip fracture patients, both in the short and long term [38,39,40,41,42]. The proposed mechanism of action being that BBt inhibits pathways that otherwise mediate the hyperadrenergic response that stems from the initial trauma and subsequent surgical interventions [43, 44]. Given the inherent nature of frailty, it can be suspected that frail patients may be more susceptible to the adverse effects of this hyperadrenergic state, considering their reduced physiologic reserve compared to more robust patients. Subsequently, BBt should also be associated with a greater reduction in mortality the more frail a hip fracture patient is. The aim of the current study was therefore to investigate how frailty, measured using the Orthopedic Hip Frailty Score (OFS), modifies the effect of preadmission beta-blocker therapy on mortality in hip fracture patients.
Methods
Data for this retrospective cohort study were obtained from the prospectively collected Swedish National Quality Register for Hip Fractures, Rikshöft [45]. All patients who underwent primary emergency hip fracture surgery in Sweden between 2008 and 2017 were eligible for inclusion. Conservatively managed and pathological hip fracture were excluded from the original data retrieval. Patients were also excluded if they were missing data required to calculate the OFS. Rikshöft provided information relating to patient demographics, admission and discharge, as well as perioperative and operative data. Using the patients’ social security numbers, this dataset was cross-referenced with the Swedish National Board of Health and Welfare’s Patient, Cause of Death, and Prescribed Drugs registers. The National Patient Register is comprised of all ICD-10 code recorded during all periods of in-patient and out-patient care, for each patient [46]. The Cause of Death Register contains the time and cause of death for anyone who dies in Sweden, irrespective of country of residence [47]. The National Prescribed Drug Register records all prescriptions issued by physicians in Sweden at primary and secondary care facilities [48]. This investigation in its entirety adheres to the strengthening the reporting of observational studies in epidemiology (STROBE) guidelines as well as the principles of the Declaration of Helsinki [49]. Ethical approval was secured from the Swedish Ethical Review Authority (reference 2022-03107-02).
Beta-blocker therapy
The Prescribed Drugs Register is a national Swedish database that logs all drug prescriptions issued by physicians within both primary and secondary care facilities. A retrieval request was made for all beta-blocker prescriptions (ATC codes C07AA, C07AB, C07AG) issued for the previously specified patients registered in Rikshöft. Ongoing BBt was defined as having filled a prescription within the 12-month period prior to, as well as subsequent to, hip fracture surgery. To avoid immortal time bias, patients who filled a prescription preoperatively, but died prior to filling a prescription postoperatively, were counted as having ongoing BBt. This 12-month period was decided on as beta-blockers are rarely discontinued once prescribed and therefore generally prescribed on a long-term basis, often covering up to a one-year period with a single prescription. Preoperative discontinuation of BBt is also rare, with no such events being found when assessing the electronic medical records of 2443 consecutive hip fracture patients operated over a 5-year period in Orebro County, Sweden [38].
Calculating the Orthopedic Hip Frailty Score
The Orthopedic Hip Frailty Score is a recently validated score for measuring frailty in hip fracture patients [50]. The OFS was determined based on the presence of the five binary variables: an age ≥ 85 years old, congestive heart failure, a history of malignancy (local or metastatic, excluding non-invasive neoplasms of the skin), institutionalization, and a non-independent functional status (i.e., requiring assistance with activities of daily life). A patient received 1 point for each variable present, with the maximum possible score being 5 [50].
Statistical analysis
Cases were stratified according to their OFS; OFS 0, OFS 1, OFS 2, OFS 3, OFS 4, and OFS 5. Within each stratum, cases were further partitioned based on if they had ongoing beta-blocker therapy (BBt+), or no ongoing beta-blocker therapy (BBt-) at the time of admission. As continuous variables were non-normally distributed, they were summarized as medians and interquartile ranges (IQRs), with the Kruskall–Wallis test being used as an omnibus test. Categorical variables were instead presented as counts and percentages. Either the Chi-squared test or Fisher’s exact test was used, as appropriate, to compare the distribution of categorical variables within the cohorts. The primary outcome of interest was 30-day postoperative mortality.
To account for potential confounding, inverse probability of treatment weighting (IPTW) was used to balance the cohorts within each stratum. The probability of treatment was assessed using a logistic regression model; BBt was set as the dependent variable while the predictors consisted of age, sex, American Society of Anesthesiologists (ASA) classification, type of fracture, type of surgery, previous myocardial infarction, peripheral vascular disease, cerebrovascular disease, diabetes mellitus, dementia, chronic obstructive pulmonary disease, connective tissue disease, liver disease, and chronic kidney disease. The weights were calculated as \(\frac{1}{\mathrm{probability \; of \; BBt}+}\) for BBt + patients and \(\frac{1}{1-\mathrm{probability \; of \; BBt}+}\) for BBt- patients. After IPTW, balance between the cohorts within each stratum was evaluated by employing absolute standardized differences (ASDs), where an ASD < 0.1 was considered balanced. The absolute risk reduction (ARR) between the BBt+ and BBt- patients, as well as the corresponding confidence interval (CI), were then calculated within each stratum [51]. A sensitivity analysis was also performed where the individual components of the OFS were included in the logistic regression model, to account for differences in the distribution of the component variables of the OFS between the BBt- and BBt+ patients.
Statistical significance was defined as a two-sided p value less than 0.05. Among cases included in the analyses, less than two percent had any form of missing data. Data that were missing were consequently assumed to be missing at random. To handle missing data, multiple imputation by chained equations was employed; logistic regression was used for sex, a proportional odds model for ASA classification, as well as Bayesian polytomous regression for type of fracture and type of surgery. Analyses were performed using the tidyverse, haven, parallel, mice, survey, tableone, and writexl packages in the statistical software R 4.0.5 (R Foundation for Statistical Computing, Vienna, Austria) [52].
Results
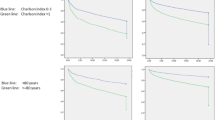
After applying the inclusion and exclusion criteria, 127,305 cases remained. In this population, 39% of the patients were in the BBt+ cohorts (N = 49,743). Metoprolol was consistently the most common beta-blocker prescribed (BBt+ , OFS 0 vs OFS 5: 56.1% vs 56.6%); however, the proportion who filled a prescription for bisoprolol increased stepwise with the OFS (BBt+ , OFS 0 vs OFS 5: 15.2% vs 26.4%). Patients with a higher OFS were generally older (BBt-, OFS 0 vs OFS 5: 90 years vs 74 years), less fit for surgery according to their ASA classification (BBt-, OFS 0 vs OFS 5: ASA ≥ 3, 26.9% vs 91.9%), and had a higher comorbidity burden according to their Charlson Comorbidity Index (CCI) (BBt-, OFS 0 vs OFS 5: CCI ≥ 7, 1.9% vs 100%). All comorbidities, except for liver disease, increased along with the OFS. The use of all types of arthroplasty decreased as patients became more frail (BBt-, OFS 0 vs OFS 5: 31.9% vs 26.2%), while the proportion of these patients managed using of hemiarthroplasty significantly increased (BBt-, OFS 0 vs OFS 5: 43.9% vs 98.1%) (Table 1).
The unadjusted 30-day postoperative mortality rate also increased as patients became more frail (BBt-, OFS 0 to 5: 1.8%, 6.2%, 12.2%, 18.4%, 30.8%, and 41.9%). Concurrently, despite generally being less fit for surgery as well as displaying a higher incidence of almost all comorbidities, BBt+ patients consistently exhibited a significantly lower postoperative mortality rate, compared to BBt- patients (BBt+ vs BBt-: OFS 0, 0.3% vs 1.8%; OFS 5, 17% vs 41.9%). This difference between the groups remained irrespective of the specific cause of mortality or stratum. Across all strata, the most common cause of mortality was cardiovascular events. This was also the mortality cause that exhibited the largest absolute reduction in all strata. However, all cause-specific mortality rates were lower in the BBt+ group compared to the BBt- group (Table 2).
After IPTW, all included potential confounders were balanced with an ASD < 0.1 (Supplemental Tables 1–6). BBt+ was associated with a reduced 30-day postoperative mortality rate, regardless of the degree of frailty. However, the adjusted ARR was larger in patients with higher frailty scores, increasing stepwise along with the OFS. Compared to BBt- patients, the mortality rate in BBt+ patients with OFS 0 was 2.2 percentage points lower [adjusted ARR (95% CI) 2.2 (2.0–2.4), p < 0.001], corresponding to a number needed to treat (NNT) of 45. Among BBt+ patients with OFS 5, the 30-day postoperative mortality rate was instead 24.1 percentage points lower [adjusted ARR (95% CI) 24.1 (18.3–30.0), p < 0.001] compared to BBt- patients, resulting in an NNT of 4. The sensitivity analysis, which also adjusted for the individual components of the OFS, resulted in virtually identical ARRs (Table 3).
Discussion
This Swedish nationwide cohort study, based on 127,305 cases, demonstrated an association between BBt and a reduction in postoperative mortality for all hip fracture patients. Using the OFS to stratify patients by the degree of frailty, a stepwise increase in the ARR associated with BBt was observed in conjunction with an increasing OFS. In effect, BBt was associated with a greater reduction in 30-day postoperative mortality rate the more frail a patient was, even after adjusting for differences in age, sex, fitness for surgery, fracture and surgery type, as well as comorbidity burden.
Hip fracture patients are one of the greatest challenges facing the orthopedic community and the postoperative mortality rates remain high despite efforts made during the past decade to reduce them [17, 53]. This has widely been attributed to old age, a significant comorbidity burden, and particularly the high degree of frailty present in this population [14,15,16,17]. However, in order to study frailty a clinically feasible tool that adequately measures frailty is required. The OFS is a parsimonious integral frailty model developed and validated for use in hip fracture patients [50, 54]. The inclusion of institutionalization and non-independent functional status allows for the consideration of the social, psychological, as well as cognitive aspects of frailty and are broadly accepted markers of frailty [55,56,57]. A history of malignancy and congestive heart failure on the other hand constitute comorbidities that reduce the patient’s physiological reserve and have therefore also been used as indicators of frailty [56,57,58,59]. Finally, while frailty and aging represent independent processes, the prevalence of frailty is recognized as increasing with age [35, 60, 61]. Moreover, an age ≥ 85 years on its own is insufficient for classifying a patient as frail with the OFS [50].
Frail patients, by definition, suffer from a disproportionately increased risk of morbidity and mortality due to external stressors [18,19,20,21]. Following hip fracture, the physiological stress response to this trauma, known as the hyperadrenergic state, is characterized by the activation of the sympathetic nervous system and mediated by a surge in catecholamines and cortisol. Despite being necessary for injury healing, this response can also have harmful side effects that can be disastrous in frail patients.These patients have a smaller margin for maintaining homeostasis as well as a reduced resistance to the catabolic state that is induced by the release of growth hormone, antidiuretic hormone, and glucagon [44, 62, 63].
It has been postulated that BBt could mitigate the hyperadrenergic state, through the binding of the active substance to adrenoreceptors, which inhibits the activation of adrenoreceptors by circulating catecholamines. Consequently, BBt is thought to reduce the negative effects caused by the physiological stress response [64]. Several studies have shown strong associations between BBt and reduced mortality in a wide range of patient populations [38,39,40,41,42, 65,66,67,68,69,70,71]. A nationwide Swedish retrospective cohort study of patients undergoing elective colon cancer surgery, with an average patient age of 72, demonstrated an association between BBt and a 70% reduction in the 90-day postoperative mortality rate [adjusted Incident Rate Ratio (IRR) (95% CI) 0.29 (0.24–0.35), p < 0.001] [70]. Maghami et al. investigated this relationship in geriatric patients undergoing emergency laparotomies and found that patients with BBt exhibited a 35% reduction in their mortality rate [adjusted IRR (95% CI) 0.65 (0.44–0.98), p = 0.04] [71]. Furthermore, a randomized controlled trial found that postadmission administration of propranolol reduces in-hospital mortality and improves long-term functional outcomes in isolated severe traumatic brain injury [65]. All these studies claim the positive effects seen are due to downregulation of the toxic effects of the catecholamine surge.
The majority of the aforementioned studies include elderly and frail patients with multiple comorbidities, which mirrors the hip fracture population. Unsurprisingly, the same patterns have been seen in studies published during the last few years on hip fracture patients. A publication from 2021, demonstrated that BBt was associated with a 72% reduced mortality rate within 30 days after hip fracture surgery [adjusted IRR (95% CI) 0.28 (0.26–0.29), p < 0.001], where BBt+ was independently associated with a reduced risk of death due to cardiovascular, respiratory, and cerebrovascular events, as well as deaths due to sepsis or multiorgan failure [39]. These associations remained up to one year postoperatively [adjusted Hazard Ratio (95% CI) 0.58 (0.57–0.60), p < 0.001]. However, the largest effect appeared to be during the initial postoperative period, when the physiological stress response is most pronounced [40].
Considering that the chief causes of postoperative mortality after hip fracture surgery are of cardiovascular origin, in a previous study the authors investigated how the Revised Cardiac Risk Index (RCRI) affects the association between BBt and postoperative mortality. This study observed a stepwise reduction in mortality with a higher RCRI score for BBt+ patients, with the greatest reduction being observed in patients with the highest cardiac risk [41]. In a similar vein, the current results also found a stepwise relationship between BBt and frailty, where BBt was associated with a larger ARR in patients with a higher frailty score. Potentially because frail patients have a greater difficulty maintaining homeostasis when subjected to the posttraumatic hyperadrenergic state. Of note, while the prevalence of cardiovascular comorbidities does increase along with the OFS, Spearman’s rank correlation coefficient between the OFS and RCRI was < 0.3 in the current dataset. This negligible correlation indicates that the OFS correctly identifies frail cohorts that may derive an additional benefit of BBt rather than merely stratifying patients by cardiovascular risk [72].
Among these frail hip fracture patients, those with dementia can generally be considered to comprise a special subgroup [16, 73]. This disease can impede definitive diagnosis, hinder preoperative management and optimization, as well as reduce or eliminate compliance with postoperative treatment regiments. Approximately 20% of all hip fracture patients in Sweden have a diagnosis of dementia prior to suffering a hip fracture [16, 42]. An earlier study, based on a Swedish national sample population, observed that patients with dementia die from the same causes as other hip fracture patients, but to a much greater extent [16]. On the other hand, when investigating the association between BBt and mortality in patients with dementia undergoing hip fracture surgery, the 30-day postoperative mortality rate was reduced by 50% in those who had BBt at admission [adjusted IRR (95% CI) 0.50 (0.45–0.54), p < 0.001] [42]. Consequently, even this particularly vulnerable subgroup may benefit from BBt; however, a randomized controlled trial will be required to ascertain this definitively.
Strengths and limitations
This analysis makes use of a large, national dataset consisting of over 127,000 consecutive hip fracture patients operated at a hospital in Sweden. The Rikshöft register this dataset is based on has a high case coverage, ranging between 80 and 90%, with 85% of hospitals that operate hip fractures contributing [74]. Accordingly, the register has received the highest certification level from the Swedish Association of Local Authorities and Regions [75, 76]. Loss to follow-up was also avoided through the use of the Swedish Cause of Death Register, which records all deaths within Sweden. Nevertheless, the usual caveats that limit the interpretability of all retrospective cohort studies, such as residual confounding and misclassification, must also be considered. It is also important to note that the BBt+ patients in the current study likely had a relatively well-adjusted BBt at admission. This does not automatically translate to a survival benefit when initiating BBt following admission due to hip fracture.
Conclusion
Beta-blocker therapy is associated with a reduced 30-day postoperative mortality rate in frail hip fracture patients, with a greater effect being observed with higher Orthopedic Hip Frailty Scores.
References
Williamson S, Landeiro F, McConnell T, Fulford-Smith L, Javaid MK, Judge A, et al. Costs of fragility hip fractures globally: a systematic review and meta-regression analysis. Osteoporos Int. 2017;28:2791–800.
Ferris H, Brent L, Sorensen J. Cost of hospitalisation for hip fracture—findings from the Irish hip fracture database. Osteoporos Int. 2022;33:1057–65.
Wong BLL, Chan YH, O’Neill GK, Murphy D, Merchant RA. Frailty, length of stay and cost in hip fracture patients. Osteoporos Int. 2022. https://doi.org/10.1007/s00198-022-06553-1.
Odén A, McCloskey EV, Johansson H, Kanis JA. Assessing the impact of osteoporosis on the burden of hip fractures. Calcif Tissue Int. 2013;92:42–9.
Johnell O, Kanis JA. An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos Int. 2006;17:1726–33.
Rapp K, Büchele G, Dreinhöfer K, Bücking B, Becker C, Benzinger P. Epidemiology of hip fractures. Z Für Gerontol Geriatr. 2019;52:10–6.
Rosengren BE, Björk J, Cooper C, Abrahamsen B. Recent hip fracture trends in Sweden and Denmark with age-period-cohort effects. Osteoporos Int. 2017;28:139–49.
Reginster J-Y, Burlet N. Osteoporosis: a still increasing prevalence. Bone. 2006;38:S4-9.
Cooper C, Campion G, Melton LJ. Hip fractures in the elderly: a world-wide projection. Osteoporos Int. 1992;2:285–9.
Cortez KA, Lai JGL, Tabu IA. Economic burden and the effects of early versus delayed hospitalization on the treatment cost of patients with acute fragility hip fractures under the UPM-PGH Orthogeriatric Multidisciplinary Fracture Management Model and Fracture Liaison Service. Osteoporos Sarcopenia. 2021;7:63–8.
Kanters TA, van de Ree CLP, de Jongh MAC, Gosens T, Hakkaart-van RL. Burden of illness of hip fractures in elderly Dutch patients. Arch Osteoporos. 2020;15:11.
Adeyemi A, Delhougne G. Incidence and economic burden of intertrochanteric fracture: a medicare claims database analysis. JBJS Open Access. 2019;4: e0045.
Wiktorowicz ME, Goeree R, Papaioannou A, Adachi JD, Papadimitropoulos E. Economic implications of hip fracture: health service use, institutional care and cost in Canada. Osteoporos Int. 2001;12:271–8.
Forssten MP, Mohammad Ismail A, Sjolin G, Ahl R, Wretenberg P, Borg T, et al. The association between the Revised Cardiac Risk Index and short-term mortality after hip fracture surgery. Eur J Trauma Emerg Surg. 2020. https://doi.org/10.1007/s00068-020-01488-w.
Forssten MP, Mohammad Ismail A, Borg T, Ahl R, Wretenberg P, Cao Y, et al. Postoperative mortality in hip fracture patients stratified by the Revised Cardiac Risk Index: a Swedish nationwide retrospective cohort study. Trauma Surg Acute Care Open. 2021;6: e000778.
Ioannidis I, Mohammad Ismail A, Forssten MP, Ahl R, Cao Y, Borg T, et al. The mortality burden in patients with hip fractures and dementia. Eur J Trauma Emerg Surg. 2021. https://doi.org/10.1007/s00068-021-01612-4.
Gundel O, Thygesen LC, Gögenur I, Ekeloef S. Postoperative mortality after a hip fracture over a 15-year period in Denmark: a national register study. Acta Orthop. 2020;91:58–62.
Fried LP, Tangen CM, Walston J, Newman AB, Hirsch C, Gottdiener J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci. 2001;56:M146-156.
Clegg A, Young J, Iliffe S, Rikkert MO, Rockwood K. Frailty in elderly people. Lancet Lond Engl. 2013;381:752–62.
Joseph B, Pandit V, Sadoun M, Zangbar B, Fain MJ, Friese RS, et al. Frailty in surgery. J Trauma Acute Care Surg. 2014;76:1151–6.
Robinson TN, Eiseman B, Wallace JI, Church SD, McFann KK, Pfister SM, et al. Redefining geriatric preoperative assessment using frailty, disability and co-morbidity. Ann Surg. 2009;250:449–55.
Sonny A, Kurz A, Skolaris LA, Boehm L, Reynolds A, Cummings KC III, et al. Deficit accumulation and phenotype assessments of frailty both poorly predict duration of hospitalization and serious complications after noncardiac surgery. Anesthesiology. 2020;132:82–94.
Cooper Z, Rogers SO, Ngo L, Guess J, Schmitt E, Jones RN, et al. A comparison of frailty measures as predictors of outcomes after orthopedic surgery. J Am Geriatr Soc. 2016;64:2464–71.
van de Ree CLP, Landers MJF, Kruithof N, de Munter L, Slaets JPJ, Gosens T, et al. Effect of frailty on quality of life in elderly patients after hip fracture: a longitudinal study. BMJ Open. 2019;9: e025941.
Kim Y-P, Choe Y-R, Park J-H, Kim S, Won C-W, Hwang H-S. Frailty index associated with all-cause mortality, long-term institutionalization, and hip fracture. Eur Geriatr Med. 2019;10:403–11.
Kwak MJ, Digbeu BD, Des Bordes J, Rianon N. The association of frailty with clinical and economic outcomes among hospitalized older adults with hip fracture surgery. Osteoporos Int J. 2022;33:1477–84.
Song Y, Wu Z, Huo H, Zhao P. The impact of frailty on adverse outcomes in geriatric hip fracture patients: a systematic review and meta-analysis. Front Public Health. 2022. https://www.frontiersin.org/articles/10.3389/fpubh.2022.890652
Amata O, Panella L, Incorvaia C, Tomba A, Gervasoni F, Caserta AV, et al. Role of frailty in functional recovery after hip fracture, the variable impact in restoring autonomy. Acta Bio Medica Atenei Parm. 2022;92:e2021387
The HEALTH Investigators. Total hip arthroplasty or hemiarthroplasty for hip fracture. N Engl J Med. 2019;381:2199–208.
Ioannidis I, Mohammad Ismail A, Forssten MP, Ahl R, Cao Y, Borg T, et al. Surgical management of displaced femoral neck fractures in patients with dementia: a comparison in mortality between hemiarthroplasty and pins/screws. Eur J Trauma Emerg Surg. 2021. https://doi.org/10.1007/s00068-021-01640-0.
Moyet J, Deschasse G, Marquant B, Mertl P, Bloch F. Which is the optimal orthogeriatric care model to prevent mortality of elderly subjects post hip fractures? A systematic review and meta-analysis based on current clinical practice. Int Orthop. 2019;43:1449–54.
Van Heghe A, Mordant G, Dupont J, Dejaeger M, Laurent MR, Gielen E. Effects of orthogeriatric care models on outcomes of hip fracture patients: a systematic review and meta-analysis. Calcif Tissue Int. 2022;110:162–84.
Sabharwal S, Wilson H. Orthogeriatrics in the management of frail older patients with a fragility fracture. Osteoporos Int. 2015;26:2387–99.
Joseph B, Zangbar B, Pandit V, Fain M, Mohler MJ, Kulvatunyou N, et al. Emergency general surgery in the elderly: too old or too frail? J Am Coll Surg. 2016;222:805–13.
Topinková E. Aging, disability and frailty. Ann Nutr Metab. 2008;52:6–11.
Goeteyn J, Evans LA, De Cleyn S, Fauconnier S, Damen C, Hewitt J, et al. Frailty as a predictor of mortality in the elderly emergency general surgery patient. Acta Chir Belg. 2017;117:370–5.
Murphy PB, Savage SA, Zarzaur BL. Impact of patient frailty on morbidity and mortality after common emergency general surgery operations. J Surg Res. 2020;247:95–102.
Mohammad Ismail A, Borg T, Sjolin G, Pourlotfi A, Holm S, Cao Y, et al. β-adrenergic blockade is associated with a reduced risk of 90-day mortality after surgery for hip fractures. Trauma Surg Acute Care Open. 2020;5: e000533.
Ahl R, Mohammad Ismail A, Borg T, Sjölin G, Forssten MP, Cao Y, et al. A nationwide observational cohort study of the relationship between beta-blockade and survival after hip fracture surgery. Eur J Trauma Emerg Surg. 2021. https://doi.org/10.1007/s00068-020-01588-7.
Mohammad Ismail A, Ahl R, Forssten MP, Cao Y, Wretenberg P, Borg T, et al. Beta-blocker therapy is associated with increased 1-year survival after hip fracture surgery: a retrospective cohort study. Anesth Analg. 2021;133:1225–34.
Mohammad Ismail A, Ahl R, Forssten MP, Cao Y, Wretenberg P, Borg T, et al. The interaction between pre-admission β-blocker therapy, the Revised Cardiac Risk Index, and mortality in geriatric hip fracture patients. J Trauma Acute Care Surg. 2022;92:49–56.
Ioannidis I, Mohammad Ismail A, Forssten MP, Cao Y, Bass GA, Borg T, et al. β-Adrenergic blockade in patients with dementia and hip fracture is associated with decreased postoperative mortality. Eur J Trauma Emerg Surg. 2022;48:1463–9.
Ley EJ, Clond MA, Bukur M, Park R, Chervonski M, Dagliyan G, et al. β-adrenergic receptor inhibition affects cerebral glucose metabolism, motor performance, and inflammatory response after traumatic brain injury. J Trauma Acute Care Surg. 2012;73:33–40.
Loftus TJ, Efron PA, Moldawer LL, Mohr AM. β-blockade use for traumatic injuries and immunomodulation: a review of proposed mechanisms and clinical evidence. Shock. 2016;46:341–51.
Om Rikshöft – RIKSHÖFT [Internet]. [cited 2021 Apr 20]. https://www.xn--rikshft-e1a.se/om-oss
The National Patient Register [Internet]. Socialstyrelsen. [cited 2021 Sep 10]. https://www.socialstyrelsen.se/en/statistics-and-data/registers/register-information/the-national-patient-register/
Dödsorsaksregistret [Internet]. Socialstyrelsen. [cited 2022 Nov 13]. https://www.socialstyrelsen.se/statistik-och-data/register/dodsorsaksregistret/
National Prescribed Drug Register [Internet]. Socialstyrelsen. [cited 2022 Oct 11]. https://www.socialstyrelsen.se/en/statistics-and-data/registers/national-prescribed-drug-register/
WMA - The World Medical Association-WMA Declaration of Helsinki – Ethical Principles for Medical Research Involving Human Subjects [Internet]. [cited 2020 Sep 21]. https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/
Forssten MP, Cao Y, Trivedi DJ, Ekestubbe L, Borg T, Bass GA, et al. Developing and validating a scoring system for measuring frailty in patients with hip fracture: a novel model for predicting short-term postoperative mortality. Trauma Surg Acute Care Open. 2022;7: e000962.
Hildebrandt M, Bender R, Gehrmann U, Blettner M. Calculating confidence intervals for impact numbers. BMC Med Res Methodol. 2006;6:32.
R Development Core Team. R: A Language and Environment for Statistical Computing [Internet]. Vienna, Austria: R Foundation for Statistical Computing; 2008. http://www.R-project.org/
Kates SL. Hip fracture programs: are they effective? Injury. 2016;47(Suppl 1):S25-27.
Gobbens RJJ, Luijkx KG, Wijnen-Sponselee MT, Schols JMGA. Towards an integral conceptual model of frailty. J Nutr Health Aging. 2010;14:175–81.
Roopsawang I, Zaslavsky O, Thompson H, Aree-Ue S, Kwan RYC, Belza B. Frailty measurements in hospitalised orthopaedic populations age 65 and older: a scoping review. J Clin Nurs. 2021. https://onlinelibrary.wiley.com/doi/abs/10.1111/jocn.16035
Joseph B, Pandit V, Zangbar B, Kulvatunyou N, Tang A, O’Keeffe T, et al. Validating trauma-specific frailty index for geriatric trauma patients: a prospective analysis. J Am Coll Surg. 2014;219:10-17.e1.
Subramaniam S, Aalberg JJ, Soriano RP, Divino CM. New 5-factor modified frailty index using American College of Surgeons NSQIP data. J Am Coll Surg. 2018;226:173-181.e8.
Malik A, Brito D, Vaqar S, Chhabra L. Congestive Heart Failure. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 [cited 2021 Dec 28]. http://www.ncbi.nlm.nih.gov/books/NBK430873/
McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Böhm M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2021;42:3599–726.
Fried LP, Xue Q-L, Cappola AR, Ferrucci L, Chaves P, Varadhan R, et al. Nonlinear multisystem physiological dysregulation associated with frailty in older women: implications for etiology and treatment. J Gerontol A Biol Sci Med Sci. 2009;64A:1049–57.
Raîche M, Hébert R, Dubois M-F. PRISMA-7: a case-finding tool to identify older adults with moderate to severe disabilities. Arch Gerontol Geriatr. 2008;47:9–18.
Desborough JP. The stress response to trauma and surgery. Br J Anaesth. 2000;85:109–17.
Moor D, Aggarwal G, Quiney N. Systemic response to surgery. Surg Oxf. 2017;35:220–3.
Mohseni S, Joseph B, Peden CJ. Mitigating the stress response to improve outcomes for older patients undergoing emergency surgery with the addition of beta-adrenergic blockade. Eur J Trauma Emerg Surg. 2021. https://doi.org/10.1007/s00068-021-01647-7.
Khalili H, Ahl R, Paydar S, Sjolin G, Cao Y, Abdolrahimzadeh Fard H, et al. Beta-blocker therapy in severe traumatic brain injury: a prospective randomized controlled trial. World J Surg. 2020;44:1844–53.
Nan Y, Jia F, Du X, Mei Z. Beta-blocker exposure for short-term outcomes following non-cardiac surgery: a meta-analysis of observational studies. Int J Surg Lond Engl. 2020;76:153–62.
Tan K, Harazim M, Tang B, Mclean A, Nalos M. The association between premorbid beta blocker exposure and mortality in sepsis-a systematic review. Crit Care Lond Engl. 2019;23:298.
Lee YR, Seth MS, Soney D, Dai H. Benefits of beta-blockade in sepsis and septic shock: a systematic review. Clin Drug Investig. 2019;39:429–40.
Sanfilippo F, Santonocito C, Morelli A, Foex P. Beta-blocker use in severe sepsis and septic shock: a systematic review. Curr Med Res Opin. 2015;31:1817–25.
Ahl R, Matthiessen P, Sjölin G, Cao Y, Wallin G, Ljungqvist O, et al. Effects of beta-blocker therapy on mortality after elective colon cancer surgery: a Swedish nationwide cohort study. BMJ Open. 2020;10: e036164.
Maghami S, Cao Y, Ahl R, Detlofsson E, Matthiessen P, Sarani B, et al. Beta-blocker therapy is associated with decreased 1-year mortality after emergency laparotomy in geriatric patients. Scand J Surg. 2019. https://doi.org/10.1177/1457496919877582.
Mukaka M. A guide to appropriate use of correlation coefficient in medical research. Malawi Med J. 2012;24:69–71.
Forssten MP, Ioannidis I, Mohammad Ismail A, Bass GA, Borg T, Cao Y, et al. Dementia is a surrogate for frailty in hip fracture mortality prediction. Eur J Trauma Emerg Surg. 2022;48:4157–67.
Rikshoft Arsrapport 2020 [Internet]. Lund, Sweden: Rikshoft; https://04e8d8b0-c67b-4aa0-a7e7-d272a37c2285.filesusr.com/ugd/3ac01b_2ce2105ebca7495c800465396dadaf89.pdf
Sveriges Kommuner och Regioner. Hip fracture | Kvalitetsregister | SKR [Internet]. 2021 [cited 2022 Oct 9]. https://web.archive.org/web/20210731033535/https://skr.se/en/kvalitetsregister/hittaregister/registerarkiv/hoftfraktur.44212.html
Sveriges Kommuner och Regioner. Certification levels [Internet]. Nationella Kvalitetsregister. [cited 2022 Feb 11]. https://skr.se/kvalitetsregister/drivaregister/attsokaochredovisamedel/certifieringsnivaer.54492.html
Funding
Open access funding provided by Örebro University.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflicts of interest to disclose.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Forssten, M.P., Mohammad Ismail, A., Ioannidis, I. et al. A nationwide analysis on the interaction between frailty and beta-blocker therapy in hip fracture patients. Eur J Trauma Emerg Surg 49, 1485–1497 (2023). https://doi.org/10.1007/s00068-023-02219-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00068-023-02219-7