
Abstract
Background
The SARS-CoV-2 (COVID-19) pandemic has the potential to evoke lasting changes in the delivery of care, and the utilization of telehealth. We sought associations between surgeon personal factors and greater use of telehealth to treat fractures relative to in-person care.
Methods
Seventy-five fracture surgeons participated in a survey-based experiment. All surgeons were asked about their preferences regarding remote compared to in-person communication. Participants rated the following items on slider scales: their degree of introversion, the importance of a hands-on/physical exam and surgeon preferences regarding telehealth. We identified factors associated with the use of, and comfort with, telehealth.
Results
The use of telehealth during the pandemic was associated with comfort evaluating wounds via telehealth. A greater proportion of remote visits was associated with comfort evaluating wounds and confidence teaching exercises via telehealth. There was consensus that telehealth did not alter utilization rates of radiographs or offer of discretionary surgery. The use of absorbable sutures to limit in-person visits was associated with a preference for working from home and greater comfort with evaluating wounds remotely. The use of 2- and 6-week post-operative telehealth visits and plans to use telehealth after the pandemic (52%) were associated with greater comfort in evaluating wounds through telehealth and greater confidence with video instruction of exercises.
Conclusions
The finding that personal factors are associated with utilization of telehealth helps target strategies for increased use of telehealth and other technologies as the pandemic wanes. Given that telehealth adds convenience for people with ambulatory difficulties or in remote areas, such efforts are warranted.
Level of Evidence
Not applicable.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The SARS-CoV-2 (COVID-19) pandemic has the potential to evoke lasting changes in the delivery of care. For instance, it has sparked surgeon interest in the use of telehealth, [1,2,3,4] and led to reimbursement of audio and video telehealth [3, 5]. These changes build on care delivery initiatives, such as virtual fracture care in the UK which has successfully omitted routine re-examination and radiographs in the care of many fractures [6,7,8,9,10].
Previous studies conducted in the US [11, 12], Europe[13, 14], and Australia [15] identified several potential advantages of telehealth in fracture care, including accessible care for remote patients, reduced travel and time spent actually experiencing care, and lower cost than in-person care, without compromising clinical outcomes or satisfaction with care [11,12,13,14,15]. On the other hand, both patients and clinicians have expressed reservations about telehealth [16], mostly related to concerns over suboptimal quality of care, inadequate relationship building between patient and clinician, and occurrence of technical issues and malfunctions.
We conducted a survey-based experiment during the height of the first wave of the COVID pandemic when most health systems prepared for a worst-case scenario. We tested the primary null hypothesis that there are no factors associated with the current (height of the pandemic) utilization rates of telehealth. Additionally, we tested the secondary null hypotheses that there were no factors associated with 1) surgeon perceived utilization rates of diagnostic and treatment modalities (e.g., radiographs, surgery, absorbable sutures) during the pandemic, and 2) expected future telehealth use.
Materials and methods
Study design and setting
This study was approved by our Institutional Review Board. We invited fracture surgeons from the Science of Variation Group (SOVG) to participate in a survey-based experiment. We used SurveyMonkey (Palo Alto, CA, USA) to create a questionnaire gauging surgeon preferences and habits regarding trauma care and telehealth during the pandemic (Appendix 1). The survey consisted of four sections: (a) surgeon personality and preferred work style; (b) general fracture care during the pandemic; (c) care for fractures with a good prognosis (e.g., proximal humerus, distal radius, and radial head fractures with limited displacement and metacarpal fractures suitable for non-operative treatment); and (d) post-operative care for patients with fractures treated operatively.
The SOVG [18,19,20,21,22,23,24,25,26,27] is an international collaborative of orthopedic, plastic, and trauma surgeons who participate in monthly experiments to study reliability and variation in care. Members receive no incentives besides potential group authorship. Because we measure associations rather than rates, diversity within the sample is more important than response rate (representation of the average surgeon). Previous studies showed sufficient variation in SOVG participant opinions for viable experiments [17,18,19].
Surgeon characteristics
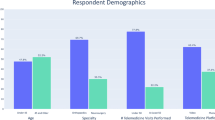
Seventy-five surgeons participated (Table 1). The majority of surgeons practice in Europe (29, 39%) or the United States (22, 29%). More than half of the surgeons had used telehealth in fracture care during the pandemic (52%), but most visits remained in person (82%).
Questions
The first set of questions was designed to gauge working styles and to collect surgeon characteristics. We asked participants about their preferred meeting type when meeting colleagues (remote or in person), their preferred contact style when contacting colleagues (phone calls or emails), and their thoughts on the preferred contact style of their patients (i.e., do surgeons think patients would rather be contacted through phone calls or through emails). Furthermore, we asked their preferences regarding their workplace (home vs. office), preferred type of conference (in-person vs self-directed or webinar), self-rated inversion (indicated on a Numeric Rating Scale [NRS], ranging from introverted to extroverted), and whether they have small children at home (“Do you have small children at home? Yes/ No”). Finally, we asked how essential they deemed the “hands-on” (physical examination) part of a visit (NRS), and whether they enjoy or dread their commute to and from work (NRS). “Do you enjoy your commute to and from work or dread it?”0 = I dread it, 50 = I don’t mind it, 100 = I enjoy it.
The next set of questions assessed how the pandemic has affected their practice. Participants were asked whether they used telehealth in the treatment of fractures and their estimated percentage of in-office vs. telehealth visits. We asked surgeons to what extent they missed not being able to do the hands-on physical exam (NRS), whether they could still adequately teach exercises, send a hand-out, or direct people to online resources (NRS), whether they ordered radiographs at different frequencies during recovery and two weeks after injury [− 50 = much less, 50 = much more (NRS)], and whether they offered discretionary surgery differently during the pandemic [(− 50 = much less, 50 = much more NRS)]. We also assessed whether surgeons considered a video visit at 2 weeks a viable option in the future for fractures where surgery may be an option, whether they offer a 6-week post-fracture review through telehealth, and whether they will continue to use telehealth in the future when treating patients recovering from fractures.
The third part of the survey focused on the treatment of fractures with a good prognosis without surgical intervention (e.g., proximal humerus, distal radius, and radial head fractures with limited displacement and metacarpal fractures). We asked to what extent surgeons missed performing a physical exam (NRS), whether they could treat these types of fractures without additional radiographs (− 50 = completely disagree, 50 = completely agree), whether a video evaluation is a viable option for these types of fractures, and whether surgeons will continue to use telehealth for care of these types of fractures.
The final part of the survey asked surgeons whether they had used absorbable sutures during the pandemic to minimize in-person visits after surgery and whether surgeons offered a 2-week wound review through telehealth after surgery. Finally, we assessed comfort levels of surgeons for evaluating wounds without an in-person visit (NRS).
Statistical analysis
We performed descriptive statistics, reporting non-normally distributed continuous variables as median (interquartile range) and categorical variables as numbers and percentages. In bivariate analysis, we sought factors associated with the use of telehealth (yes or no), the percentage of telehealth visits, and indicating that telehealth is viable in the future. Fisher exact tests and Chi-square tests were used to assess associations between categorical variables, where appropriate, and Spearman rank-order associations, Wilcoxon–Mann–Whitney tests, and Kruskal–Wallis H tests were used for continuous variables. Alpha was set at 0.05. Additionally, we sought factors associated with agreement with the following statements: (1) video visits are viable in the future (yes or no), (2) I feel comfortable evaluating wounds via telehealth (− 50 = completely disagree to 50 = completely agree), (3) I miss the physical examination part during a video visit (− 50 = completely disagree to 50 = completely agree), (4) I will continue to use telehealth to follow up on fractures (yes or no), (5) I offer a 6-week post-fracture visit via telehealth (yes or no), (6) I use absorbable sutures during the pandemic to minimize in-person visits (yes or no), (7) I use a 2-week post-surgery check-up for wound review via telehealth (yes or no), (8) A 2-week check-up via telehealth is a viable option (yes or no), and (9) it is possible to teach exercises, use hand-outs, and direct people to online resources through telehealth (− 50 = completely disagree to 50 = completely agree). We also sought factors associated with the frequency of (1) offering surgery through telehealth (− 50 = much less, 50 = much more) and (2) ordering X-rays through telehealth (− 50 = much less, 50 = much more). We accounted for the following independent variables: gender, location of practice, years in practice, supervising trainees, having young children, and self-rated inversion (introverted vs extroverted), indicating the physical exam is essential, enjoying the commute, surgeon thoughts on patient preference for emails (vs. phone calls) and surgeon preference for (1) remote meetings, (2) contacting colleagues by email, (3) working from home, and (4) webinars.
Results
Telehealth use for fracture care during COVID-19 pandemic
Fifty-two percent of surgeons used telehealth during the pandemic to treat fractures (Table 1) and greater use of telehealth was associated with greater surgeon comfort evaluating wounds via telehealth (Table 2).
Percent of visits via telehealth
Eighteen percent of visits were conducted through telehealth at the height of the pandemic. A greater percentage of telehealth visits (relative to in-person visits) was associated with both greater surgeon comfort of evaluating wounds through telehealth and greater confidence teaching exercises via telehealth (Table 2).
Use of radiographs for non-operative fractures with a good prognosis
We found consensus (median score 0, IQR -24 [less radiographs] to 20 [more radiographs]) among surgeons that additional radiographs are unnecessary when treating fractures with a good prognosis for natural healing, so we did not analyze this further (Table 3).
Offering surgery for fractures with the option of discretionary surgery via telehealth
Surgeons offered discretionary fracture surgery at the same rate (median score of 0; IQR -8 to 1) via telehealth as they did before the pandemic, so we did not analyze this further (Table 3).
Use of radiographs for fractures with the option of discretionary surgery
Overall, surgeons ordered radiographs with the same frequency median score of (0; IQR -21 to 0) through telehealth as in person, so we did not analyze this further (Table 3).
Belief that a 2-week telehealth check-up post-surgery is a viable option in the future
Forty-seven percent of surgeons consider a 2-week post-surgery check-up via telehealth a viable option (Table 3). This was associated with greater comfort in evaluating wounds through telehealth and greater confidence with video instruction of exercises (Table 4).
Offer of telehealth visit for 6-week post-fracture evaluation
Fifty-one percent of surgeons offered a 6-week post-fracture evaluation via telehealth. Offering a 6-week post-fracture visit via telehealth was associated with a more self-rated introverted personality and greater confidence with video instruction of exercises (Table 4).
Use of absorbable sutures during the pandemic to minimize return visits
Forty-two percent of the surgeons used absorbable sutures during the pandemic to minimize in-person visits after surgery (Table 3). The use of absorbable sutures was associated with a preference for working from home and greater comfort in evaluating wounds through telehealth (Table 4).
Plan to use telehealth in the future for follow-up during care of non-operative fractures with a good prognosis
Sixty-seven percent of surgeons plan to continue to use telehealth when treating non-operative fractures with a good prognosis (Table 3). Continued use of telehealth for treating these fractures was associated with a preference for self-directed learning and webinars as opposed to in-person conferences, greater comfort in evaluating wounds through telehealth, and greater confidence in teaching exercises via telehealth (Table 5).
Plan to use telehealth for second visit during care of fractures with the option of discretionary surgery
Fifty-two percent of the surgeons plan to continue to use telehealth when treating fractures with the option of discretionary surgery (Table 3). Continued use of telehealth for treating fractures with the option of discretionary surgery was associated with greater comfort in evaluating wounds through telehealth and greater confidence in teaching exercises via telehealth (Table 4).
Discussion
The pandemic resulted in a quantum leap in the use of telemedicine (Table 6). Until the pandemic, the uptake of virtual fracture care was limited, which may suggest that patients and surgeons tend to regard fracture care as something that needs to happen in-person. We measured factors associated with use of telehealth for fracture care during the pandemic to identify opportunities for accelerating adoption of new treatment strategies. We found that surgeon factors, such as confidence with teaching exercises and reviewing wounds through telehealth, were associated with utilization of telehealth.
This study has several limitations. First, most of our participants practice in Europe and the US, and the utilization rates may not generalize to other geographical regions. However, there was sufficient diversity within the sample to measure statistical associations, and we expect that the associations between personal factors and telemedicine utilization applies to other populations of surgeons. In the same vein, we periodically make efforts to expand and diversify (and anyone reading this is encouraged to join https://www.surveymonkey.com/r/XD7FMN5), but most participants in SOVG are white, men, academics from the United States and Europe, which reflects the limited diversity in orthopedic surgery. Other factors include recruitment largely from our home countries, use of English, and reliance on people that respond to emails and are willing to give us 15 min of their time each month. Third, the associations tested were based on opinions of surgeons, not actual utilization rates. We expect that the observations of actual practice are likely to reflect the opinions expressed. Finally, our study used a large number of variables and comparisons, and because of the exploratory nature of the study, no statistical correction was made for multiple comparisons. The consistency of related comparisons strengthens the conclusion that personal factors are important. We considered logistic regression and decided against it given the exploratory nature of the study. In a prior similar study, very few factors made it into the regression and we felt we had lost important information [36]. Although the bivariate associations were not always strong, they are meaningful and direct us towards new research questions and methods concerning telehealth use.
The finding that personal factors, such as confidence evaluating wounds and teachings exercises through telemedicine, were associated with both current utilization (greater use of telehealth and a greater percentage of telehealth visits) and future utilization (viability of a 2-week, and 6-week check-up via telehealth for both non-operatively and surgically treated fractures) of telehealth suggests adoption of telehealth in fracture care will depend largely on personal factors. This is also consistent with other lines of evidence demonstrating the influence of surgeon biases and preferences on variations in care [17, 32]. The use of telehealth has shown several benefits for both patients and clinicians (e.g., avoiding costs of transportation, time off work, and it may lower the barrier to receiving care, especially for patients who live in rural areas[16, 33,34,35]). Rethinking the role of telehealth in Orthopedic Trauma care has the potential to help design more efficient care pathways (e.g., video visits could be used as an effective method for triage) and has the potential to lower the costs and improve the convenience of care. It is possible that COVID-19 pandemic will accelerate the use of telehealth visits and evoke lasting changes in the delivery of care. This notion is consistent with our finding that most physicians believed telehealth to be a viable option for treating fractures with a good prognosis for natural healing and will continue to use telehealth to treat these fractures in the future.
The observation that surgeons felt that care through telehealth did not differ from care in person with respect to adequate instruction, directing people to online resources, use of radiographs, and decision-making supports the potential increased utilization of telehealth. These results are in line with results of study on general surgery patients that showed safe and effective management of common surgical conditions via telehealth [28]. Other similar studies suggest that telehealth is an effective method for general and pediatric [29] surgery consultations [30, 31].
Our study supports the notion that personal preferences play a considerable role in the utilization of and expressed comfort with telehealth. It is possible that COVID-19 pandemic will motivate surgeons to increase use of telehealth as an alternative to in-person visits. Expanded use of telehealth has the potential to assist with the design of more efficient care strategies, which might lower the costs of care. Our data demonstrate that efforts directed toward helping surgeons feel more confident about examination, decision-making, and instruction via video have the potential to increase utilization of telehealth in fracture care.
Availability of data and material
Not applicable.
Code availability
Not applicable.
References
Tanaka MJ, Oh LS, Martin SD, Berkson EM. Telemedicine in the era of COVID-19: the virtual orthopaedic examination. J Bone Jt Surg Am. 2020. https://doi.org/10.2106/JBJS.20.00609.
Pollock K, Setzen M, Svider PF. Embracing telemedicine into your otolaryngology practice amid the COVID-19 crisis: an invited commentary. Am J Otolaryngol. 2020;41(3): 102490.
Mann DM, Chen J, Chunara R, et al. COVID-19 transforms health care through telemedicine: evidence from the field. J Am Med Inform Assoc. 2020. https://doi.org/10.1093/jamia/ocaa072.
Luciani LG, Mattevi D, Cai T, et al. Teleurology in the time of Covid-19 pandemic: here to stay? Urology. 2020. https://doi.org/10.1016/j.urology.2020.04.004.
O’ Reilly MF, Merghani K, Sheehan E,. Virtualised care and COVID-19. Ir J Med Sci. 2020. https://doi.org/10.1007/s11845-020-02269-5.
Van Gerven P, El Moumni M, Zuidema WP, et al. Omitting routine radiography of traumatic distal radial fractures after initial 2-week follow-up does not affect outcomes. J Bone Jt Surg Am. 2019. https://doi.org/10.2106/JBJS.18.01160.
Van Gerven P, Van Dongen JM, Rubinstein SM, et al. Reduction of routine use of radiography in patients with ankle fractures leads to lower costs and has no impact on clinical outcome: an economic evaluation. BMC Health Serv Res. 2020. https://doi.org/10.1186/s12913-020-05725-1.
Rubin GD. Costing in radiology and health care: rationale, relativity, rudiments, and realities. Radiology. 2017;282:333–47.
Thaker S, Botchu R, Gupta H. Enhancing musculoskeletal radiology experience in the United Kingdom: a beginner’s guide for an Indian radiologist. Indian J Musculoskelet Radiol. 2019. https://doi.org/10.25259/ijmsr_42_2019.
Bellringer SF, Brogan K, Cassidy L, Gibbs J. Standardised virtual fracture clinic management of radiographically stable Weber B ankle fractures is safe, cost effective and reproducible. Injury. 2017. https://doi.org/10.1016/j.injury.2017.04.053.
Lese A, Sraj S. Rural orthopedics: providing orthopedic care in rural communities. Orthopedics. 2019. https://doi.org/10.3928/01477447-20190624-01.
Wongworawat MD, Capistrant G, Stephenson JM. The opportunity awaits to lead orthopaedic telehealth innovation. J Bone Jt Surg Am. 2017. https://doi.org/10.2106/JBJS.16.01095.
Holderried M, Schlipf M, Höper A, et al. Chances and risks of telemedicine in orthopaedics and trauma surgery. Z Orthop Unfall. 2018. https://doi.org/10.1055/s-0043-116941.
Buvik A, Bugge E, Knutsen G, et al. Patient reported outcomes with remote orthopaedic consultations by telemedicine: a randomised controlled trial. J Telemed Telecare. 2019. https://doi.org/10.1177/1357633X18783921.
Caffery LJ, Taylor M, North JB, Smith AC. Tele-orthopaedics: a snapshot of services in Australia. J Telemed Telecare. 2017. https://doi.org/10.1177/1357633X17732800.
Board on Health Care Services; Institute of Medicine. The role of telehealth in an evolving health care environment. Washington: National Academies Press; 2012.
Janssen SJ, Teunis T, Guitton TG, et al. Do surgeons treat their patients like they would treat themselves? Clin Orthop Relat Res. 2015. https://doi.org/10.1007/s11999-015-4304-z.
van Wulfften Palthe ODR, Neuhaus V, Janssen SJ, et al. Among musculoskeletal surgeons, job dissatisfaction is associated with burnout. Clin Orthop Relat Res. 2016. https://doi.org/10.1007/s11999-016-4848-6.
Teunis T, Janssen S, Guitton TG, et al. Do orthopaedic surgeons acknowledge uncertainty? Clin Orthop Relat Res. 2016. https://doi.org/10.1007/s11999-015-4623-0.
Bruinsma WE, Becker SJE, Guitton TG, et al. How prevalent are hazardous attitudes among orthopaedic surgeons? Clin Orthop Relat Res. 2015. https://doi.org/10.1007/s11999-014-3966-2.
Crijns TJ, Janssen SJ, Davis JT, et al. Reliability of the classification of proximal femur fractures: does clinical experience matter? Injury. 2018. https://doi.org/10.1016/j.injury.2018.02.023.
Farr S, Guitton T, Ring D. How reliable is the radiographic diagnosis of mild madelung deformity? J Wrist Surg. 2018. https://doi.org/10.1055/s-0037-1612636.
Beks R, Drijkoningen T, Claessen F, et al. Interobserver Variability of the diagnosis of scaphoid proximal pole fractures. J Wrist Surg. 2018. https://doi.org/10.1055/s-0038-1641716.
Crijns TJ, Mellema JJ, Özkan S, et al. Classification of tibial plateau fractures using 3DCT with and without subtraction of unfractured bones. Injury. 2020. https://doi.org/10.1016/j.injury.2020.07.038.
Zwiers R, Weel H, Mallee WH, et al. Large variation in use of patient-reported outcome measures: a survey of 188 foot and ankle surgeons. Foot Ankle Surg. 2018. https://doi.org/10.1016/j.fas.2017.02.013.
Wasterlain AS, Melamed E, Karia R, et al. The effect of price on surgeons’ choice of implants: a randomized controlled survey. J Hand Surg Am. 2017. https://doi.org/10.1016/j.jhsa.2017.05.005.
Mallee WH, Mellema JJ, Guitton TG, et al. 6-week radiographs unsuitable for diagnosis of suspected scaphoid fractures. Arch Orthop Trauma Surg. 2016. https://doi.org/10.1007/s00402-016-2438-4.
Cain SM, Moore R, Sturm L, et al. Clinical assessment and management of general surgery patients via synchronous telehealth. J Telemed Telecare. 2017. https://doi.org/10.1177/1357633X16636245.
Dean P, O’Donnell M, Zhou L, Skarsgard ED. Improving value and access to specialty medical care for families: a pediatric surgery telehealth program. Can J Surg. 2019. https://doi.org/10.1503/cjs.017318.
Postuma R, Loewen L. Telepediatric surgery: capturing clinical outcomes. J Pediatr Surg. 2005. https://doi.org/10.1016/j.jpedsurg.2005.01.049.
Nandra K, Koenig G, DelMastro A, et al. Telehealth provides a comprehensive approach to the surgical patient. Am J Surg. 2019. https://doi.org/10.1016/j.amjsurg.2018.09.020.
Hageman MGJS, Guitton TG, Ring D, et al. How surgeons make decisions when the evidence is inconclusive. J Hand Surg Am. 2013. https://doi.org/10.1016/j.jhsa.2013.02.032.
Pande RL, Morris M, Peters A, et al. Leveraging remote behavioral health interventions to improve medical outcomes and reduce costs. Am J Manag Care. 2015;21:e141–51.
Frick KD, Burton LC, Clark R, et al. Substitutive hospital at home for older persons: effects on costs. Am J Manag Care. 2009;15:49–56.
Leff B, Burton L, Mader SL, et al. Comparison of functional outcomes associated with hospital at home care and traditional acute hospital care. J Am Geriatr Soc. 2009. https://doi.org/10.1111/j.1532-5415.2008.02103.x.
Al Salman A, Ring D, Doornberg J, Crijns T. Personal factors and musculoskeletal telehealth. Arch Bone Jt Surg. 2021. https://doi.org/10.22038/abjs.2021.55263.2752.
Acknowledgements
The authors thank the Science of Variation Group: Henry Broekhuyse; Minos Tyllianakis; Brian J Cross; Reto H. Babst; Lob Guenter; Neil Wilson; Raymond Malcolm Smith; John Munyak; Jaimo Ahn; l marsh; Prof. Andreas Platz; Thomas Mittlmeier; Rodrigo Pesantez; Ole Brink; Antonio Barquet; Tomo Havliček; Prashanth Inna; Daniel C. Wascher; Mr Andrew John Powell; Jan Biert; Frede Frihagen; Emilia Stojkovska Pemovska; Richard Jenkinson; Robert Haverlag; Daphne Beingessner; Alan Kawaguchi; Matthew Mormino; Paul Appleton; Cyrus Klostermann; Yoram Weil; Kevin Eng; Christopher Vertullo; Quell M.; Matthew Menon; marc swiontkowski; Joseph M. Conflitti; amparo gomez gelvez; Lauren MacCormick; Nelson Elias; Harold Alonso Villamizar; Peter Schandelmaier; Ladislav Mica; Steven J Morgan; Jose Eduardo Grandi Ribeiro Filho; Richard Buckley; Franz Josef Seibert; L.W. van der Plaat; Nikolaos Kanakaris; Edward K Rodriguez; Kevin Rumball; James A Gillespie; Kyle Dickson; Michael Prayson; Maarten W.G.A. Bronkhorst; Christos Garnavos; T. Schepers; Thomas DeCoster; EFSTATHIOS G. BALLAS; Toni M McLaurin; Frank W Bloemers; Vincenzo Giordano; Boj Mirck; Rob Parisien; Max Talbot; Hans Goost; A.B. Spoor; Pradeep Choudhari; Clay Spitler; Gadbled G; P.V. van Eerten; Diederik O. Verbeek; Anze Kristan; Marinis Pirpiris; Tim Chesser; and Ralf Walbeehm.
Funding
The authors did not receive any form of funding for this research.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Each author certifies that he or she has no commercial associations (e.g., consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article.
Ethical approval
All authors certify that all procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000. Patients were invited to participate by researchers not involved in patient care. They were assured all participation was voluntary, anonymous, and did not affect their care. Accepting the invitation to enroll and answering the questionnaires implied consent. No identifying information about participants is included in the article. This study has been approved by our institute review board (IRB).
Informed consent
Informed consent was obtained from all patients participating in this study.
Consent for publication
Not applicable.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Al Salman, A., Fatehi, A., Crijns, T.J. et al. Surgeon preferences are associated with utilization of telehealth in fracture care. Eur J Trauma Emerg Surg 49, 261–272 (2023). https://doi.org/10.1007/s00068-022-02065-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00068-022-02065-z