
Abstract
Purpose
We evaluated the short-term and long-term outcomes of emergency operations for peptic ulcer (PUD) complications in a period of time in which the need for surgery is infrequent.
Methods
Retrospective review of operated patients (2007–2015) in one medical center.
Results
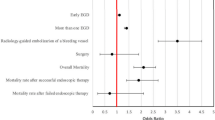
81 patients were included (8.9 patients/year): 70 (86.4%) male; 11 (13.6%) female. Indications for operation were hemorrhage in 18 (22.2%), perforation in 62 (76.5%) and gastric-outlet obstruction in one (1.2%). Only 16 (19.8%) operations included a procedure to reduce gastric acid secretion. Six (7.4%) patients had a second operation for recurrent or persistent complication. Of these, two had a procedure to reduce gastric acid secretion in their first operation. 16 (19.8%) patients died during the index hospitalization. Three (3.7%) patients were rehospitalized for a PUD complication following 3–24 months. One patient, who had surgery for a second perforation 3 months following the first operation, was treated empirically for Helicobacter Pylori (HP) between the two operations. In comparison to perforation, patients with hemorrhage were older (69.9 ± 20.3 vs. 52.1 ± 19.9 years; p = 0.0015), more commonly had a history of PUD or treatment by nonsteroidal anti-inflammotry drugs (55.6 vs. 19.4%; p = 0.0054), more commonly had a procedure to reduce gastric acid secretion during their index operation (61.1 vs. 6.5%; p < 0.0001), and had a higher mortality (38.9 vs. 14.5%; p = 0.0406).
Conclusions
Mortality is high following surgery for the complications of PUD, moreso in patients undergoing surgery for hemorrhage. Reoperations and repeated hospitalizations for complications are not uncommon, even in patients who have had procedures to reduce gastric acid secretion and HP eradication.

Similar content being viewed by others


References
Aro P, Storskrubb T, Ronkainen J, Bolling-Sternevald E, Engstrand L, Vieth M, Stolte M, Talley NJ, Agreus L. Peptic ulcer disease in a general adult population. The Kalixanda study: a random population-based study. Am J Epidemiol. 2006;163(11):1025–34.
Millat B, Fingerhut A, Borie F. Surgical treatment of complicated duodenal ulcers: controlled trials. World J Surg. 2000;24(3):299–306.
Billing A, Frohlich D, Schildberge FW, Peritonitis Study Group. Prediction of outcome using the Mannheim peritonitis index in 2003 patients. Br J Surg 1994; 81(2):209–13.
Dindo D, Demartines N, Clavien PA. Classification of surgical complications. A new proposal with evaluation cohort of 6336 patients and results of a survey. Ann Surg. 2004;240(2):205–13.
Boey J, Choi SK, Alagaratnam TT, Poon A. Risk stratification in perforated duodenal ulcer. A prospective validation of predictive factors. Ann Surg. 1987;205(1):22–6.
Bilimoria KY, Liu Y, Paruch JL, Zhou L, Kmiecik TE, Ko CY, Cohen ME. Development and evaluation of the universal ACS NSQIP Surgical Risk Calculator: a decision aid and informed consent tool for patients and surgeons. J Am Coll Surg 2013;217(5):833–42.
McEntee G, Ryan W, Peel AL, Rosenberg IL, Devlin HB. A district general hospital experience of surgical treatment of gastric and duodenal ulcer from 1970 to 1982. Surg Gynecol Obstet. 1988;167(1):53–60.
McConnell DB, Baba GC, Deveney CW. Changes in surgical treatment of peptic ulcer disease within a veterans hospital in the 1970s and the 1980s. Arch Surg. 1989;124(10):1164–7.
Ohmann C, Imhof M, Roher HD. Trends in pepticlulcer bleeding and surgical treatment. World J Surg 2000;24:284–93.
Egberts JH, Summa B, Schultz U, Schafmayer C, Hinz S, Tepel J. Impact of preoperative physiological risk profile on postoperative morbidity and mortality after emergency operation of complicated peptic ulcer disease. World J Surg. 2007;31:1449–57.
NIH Consensus Conference. Therapeutic endoscopy and bleeding ulcers. JAMA 1989;262(10):1369–72.
Loffroy R, Guiu B. Role of transcatheter arterial embolization for massive bleeding from gastroduodenal ulcers. World J Gastroenterol. 2009;15(47):5889–97.
Toyoda H, Nakano S, Takeda I, Kumada T, Sugiyama K, Osada T, Kiriyama S, Suga T. Transcatheter arterial embolization for massive bleeding fro duodenal ulcers not controlled by endoscopic hemostasis. Endoscopy. 1995;27(4):303–7.
Venclauskas L, Bratlie SO, Zachrisson K, Maleckas A, Puduzius J, Jonson C. Is transcatheter arterial embolization a safer alternative than surgery when endoscopic therapy fails in bleeding duodenal ulcer. Scand J Gastroenterol. 2010;45(3):299–304.
Jamieson GG. Current status of indications for sugery in peptic ulcer disease. World J Surg. 2000;24(3):256–8.
Cherian PT, Cherian S. Singh P. Long-term follow-up of patients with gastric outlet obstruction related to peptic ulcer disease treated with endoscopic balloon dilatation and drug therapy. Gastrointest Endosc. 2007;66(3):491–7.
Heo J, Jung MK. Safety and efficacy of a partially covered self-expandable metal stent in benign pyloric obstruction. World J Gastroenterol. 2014;20(44):16721–5.
Lagoo J, Pappas TN, Perez A. A relic or still relevant: the narrowing role for vagotomy in the treatment of peptic ulcer disease. Am J Surg. 2014;207(1):120–6.
Scroder VT, Pappas TN, Vaslef SN, De La Fuente SB, Scarborough JE. Vagotomy/drainage is superior to local oversew in patients who require emergency surgery for bleeding peptic ulcers. Ann Surg. 2014;259:1111–8.
Satoh K, Yoshino J, Akamatsu T, Itoh T, Kato M, Kamada T, Tagaki A, Chiba T, Nomura A, Mizokami Y, Murakami K, Sakamoto C, Hiraishi H, Ichinose M, Uemura N, Goto H, Joh T, Miwa H, Sugano K, Shimosegawa T. Evidence-based clinical practice guidelines for peptic ulcer disease 2015. J Gastroenterol 2016;51:177–94.
Ng EK, Chung SC, Lau JT, Sung JJ, Leung JW, Raimes SA, Chan AC, Li AK. Risk of further ulcer complications after an episode of peptic ulcer bleeding. Br J Surg. 1996;83(6):840–4.
Jensen DM, Cheng S, Kovacs TOG, Randall G, Jensen ME, Reedy T, Frankl H, Machicado G, Smith J, Silpa M, van Deventer G. A controlled study of ranitidine for the prevention of recurrent hemorrhage from duodenal ulcer. NEJM. 1994;330(6):382–6.
Graham DY, Hepps KS, Ramirez FC, Lew GM, Saeed ZA. Treatement of Helicobacter pylori reduces the rate of rebleeding in peptic ulcer disease. Scan J Gastroenterol. 1993;28(1):939–42.
Ng EK, Lam YH, Sung JJ, Yung MY, TO KF, Chan AC, Lee DW, Law BK, Lau JY, Lau WY, Chung SC. Eradication of Helicobacter pylori prevents recurrence of ulcer after simple closure of duodenal ulcer perforation. Ann Surg. 2000;231(2):153–8.
Cowles RA, Mulholland MW. Surgical management of peptic ulcer disease in the helicobacter era—management of bleeding peptic ulcer. Surg Laparosc Percutan Tech. 2001;11(1):2–8.
Søreide K, Thorsen K, Harrison EM, Bingener J, Møller MH, Ohene-Yeboah M, Søreide JA. Perforated peptic ulcer. Lancet. 2015;386:1288–98.
Koskensalo S, Leppaniemi A. Perforated duodenal ulcer: has anything changed. Eur J Trauma Emerg Surg. 2010;36(2):145–50.
Kauffman GL Jr. Duodeanl ulcer disease: treatment by surgery, antibiotics, or both. Adv Surg. 2000;34:121–35.
Rokkas T, Karameris A, Mavrogerogis A, Rallis E, Giannikos N. Eradication of Helicobacter pylori reduces the possibility of rebleeding in peptic ulcer disease. Gastrointest Endosc. 1995;41(1):1–4.
Japsersen D, Koerner T, Schorr W, Brennenstuhl M, Raschka C, Hammar CH. Helicobacter pylori eradication reduces the rate of rebleeding. Gastrointest Endosc. 1995;41(1):5–7.
Møller MH, Adamsen S, Wøjdemann M, Møller AM. Perforated peptic ulcer: how to improve outcome? Scand J Gastroenterol. 2009;44(1):15–22.
Rockall TA, Logan RF, Devlin HB, Norfield TC. National audit of upper gastrointestinal hemorrhage. Risk assessment after acute upper gastrointestinal hemorrhage. Gut. 1996;38(3):316–21.
Vreeburg EM, Terwee CB, Snel P, Rauws EA, Bartelsman JF, Meulen JH, Tytgat GN. Validation of the Rockall risk scoring system in upper gastrointestinal bleeding. Gut. 1999;44(3):331–5.
Hussain H, Lapin S, Cappell MS. Clinical scoring systems for determining the prognosis of gastrointestinal bleeding. Gastroenterol Clin North Am. 2000;29(2):445–64.
Lanza FL. Ad Hoc Committee on Practice Parameters of the American College of Gastroenterology. A guideline fo the treatment and prevention of NSAID-induced ulcers. Am J Gastroenterol. 1998;93(11):2037–46.
Gabriel SE, Jaakkimainen L, Bombardier C. Risk for serious gastrointestinal complications related to use of nonsteroidal anti-inflammatory drugs. A meta-analysis. Ann Intern Med. 1991;115(10):787–96.
Davis A. The dangers of NSAIDs: look both ways. Br J Gen Pract. 2016;66(645):172–3.
Chung CS. Surgery and gastrointestinal bleeding. Gastrointest Endoscp. 1997;46(1):33–6.
Morris DL, Hawker PC, Brearley S, Simms M, Dykes PW, Keighley MRB. Timing of operation for bleeding peptic ulcer: prospective randomized trial. BMJ. 1984;288:1277–80.
Wheatley KE, Snyman JH, Brearley S, Keighley MRB, Dykes PW. Mortality in patients with bleeding peptic ulcer when those aged 60 or over are operated on early. BMJ. 1990;301:272.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Rabea Hasadia, Yael Kopelman, Oded Olsha, Ricardo Aflici and Itamar Ashkenazi declare that they have no conflict of interest.
Research involving human participants and/or animals
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable standards. This article does not contain any studies with animals performed by any of the authors.
Ethical approval
This study was performed following approval of the Hillel Yaffe Medical Center’s institutional review board (Helsinki Committee).
Informed consent
This was a retrospective study and formal informed consent was not required.
Additional information
Preliminary results of this study were presented in the following conferences: 18th European Congress of Trauma and Emergency Surgery, Bucharest, Romania (May 7–9, 2017); 32nd Bi-annual meeting for the Israeli Surgical Association. Hotel Pastoral, Kfar Blum, Israel (May 10–12, 2017).
Rights and permissions
About this article

Cite this article
Hasadia, R., Kopelman, Y., Olsha, O. et al. Short- and long-term outcomes of surgical management of peptic ulcer complications in the era of proton pump inhibitors. Eur J Trauma Emerg Surg 44, 795–801 (2018). https://doi.org/10.1007/s00068-017-0898-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00068-017-0898-z