
Abstract
Purpose
Laryngotracheobronchial injuries (LTBI) are serious injuries because of their consequences in terms of ventilation, coupled with the severity of other injuries associated with them. We share our experience in managing these patients perioperatively in our level 1 trauma centre.
Methods
A retrospective analysis of the records of 30 patients with LTBI who presented at Jai Prakash Narayan Apex Trauma Center (JPNATC) from December 2007 to February 2011 was done. The demographics, mechanism of injury, clinical presentation, diagnostic modalities, anaesthetic management and outcome in these patients were reviewed.
Results
Intrathoracic location of the injury and Injury Severity Score (ISS) had a direct correlation with the outcome of the patients. The overall mortality was 6.7 %.
Conclusion
Meticulous examination, details about the mechanism of injury, careful diagnostic evaluation, and skilful airway and surgical management are necessary for a better outcome in patients with airway injuries. A high degree of suspicion in occult injuries and liberal use of a fibreoptic bronchoscope aids diagnosis and management. Prompt airway management in the pre-hospital setting before transfer to a higher level trauma centre ensures better outcomes.
Similar content being viewed by others


Introduction
Laryngotracheobronchial injury (LTBI) can result from blunt or penetrating trauma to the laryngotracheobronchial tree [1]. The incidence of these injuries once thought to be rare is on a rise due to increasing motor vehicle collisions (MVC) and crime rates. These are serious injuries because of their consequences in terms of ventilation, coupled with the severity of the thoracic and extrathoracic injuries often associated with them. The diagnosis of LTBI after blunt injury is a challenge because of varied yet subtle presentations or because of associated injuries [2]. An early diagnosis and treatment is essential for successful outcome [3]. The increase in frequency and varied presentations of LTBI, and the limited literature on anaesthetic management led us to review our experience with such injuries over the past 3 years in our institute.
Materials and methods
Our level 1 trauma centre receives trauma patients brought directly from the accident site, in addition to referrals from other centres. All patients with injuries involving the airway between the larynx and second generation bronchus were identified from December 2007 to February 2011. The records of these patients were retrospectively reviewed and analysed. The mechanism of injury, demographical pattern, clinical presentation, diagnostic modalities, anaesthetic management and their outcome were studied. The results were statistically analysed using unpaired t-tests and Chi-square tests.
Results
Demography and mechanism
The total number of hospital admissions from December 2007 to February 2011 was 15,589, of which 30 patients (0.002 %) with LTBI were identified. The median age of presentation was 29 years (range 8–60 years) and 77 % of them were male. Blunt trauma due to MVC was the most common mechanism of injury, while history of fall from a height was present in two patients (Fig. 1). Twelve patients had penetrating injury, with the predominant mechanism being homicidal stab injury. In all, 24 patients had extrathoracic laryngotracheal injury, whereas six had intrathoracic tracheobronchial injury (TBI) (Fig. 2). The time of injury to the time of admission ranged from 1 h to 10 days, with a median of 37 h. This wide range was observed because 17 patients were referred from other centres.

Mechanism of injury among the study patients

Frequency of laryngotracheobronchial injuries (LTBI) in our level 1 trauma centre
Clinical features
The clinical features of patients who presented with LTBI are shown in Fig. 3. Subcutaneous emphysema involving the face, neck and chest and dyspnoea were the most consistent findings in the patients. A careful examination of the neck for the ligature mark was done in patients with a history of strangulation (chain snatching/entangling of scarf) to aid the diagnosis of occult airway injuries (Fig. 4a). The details of the mechanism of injury and a high index of clinical suspicion aided the diagnosis in such patients. Eleven patients with extrathoracic tracheal injuries presented with an air leak from the neck wound (Fig. 4b). In six patients with extrathoracic injury, there was no external wound in the neck. Two patients presented with haemorrhagic shock which was due to associated vascular injuries. Orthopaedic (seven) and oesophageal (five) injuries were most commonly associated with blunt and penetrating trauma, respectively. The other associated injuries involved maxillofacial trauma (three), spine injury (three) and vascular injury (two). The Injury Severity Score (ISS) ranged from 9 to 75, with a median of 18 and the Glasgow Coma Scale (GCS) score noted in the patients ranged from 9 to 15.

Clinical features among patients with blunt injuries (red bars) and penetrating injuries (purple bars)

a External bruise over the neck in a patient with occult laryngeal injury. b External wound seen over the anterior aspect of the neck
Diagnosis
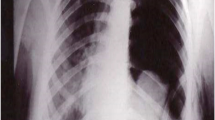
Despite the varied clinical presentation, a strong suspicion and careful examination aided the diagnosis in 14 patients. Air leak from the injury site was diagnostic of extrathoracic laryngotracheal injury in 11 patients. Surgical exploration further reaffirmed the presence of laryngotracheal injury (Fig. 5). A chest roentgenogram done in the emergency room (ER) as a part of the primary survey revealed abnormal findings in 25 patients. Subcutaneous emphysema was the most consistent finding (22), while pneumothorax and pneumomediastinum were commonly seen in intrathoracic tracheobronchial injuries (Fig. 6). Total collapse of the lung (fallen lung sign) with pneumothorax was observed in one patient with avulsion of the right bronchus (Fig. 7). Bronchoscopy was used as the diagnostic modality in 12 patients (eight extrathoracic, four intrathoracic) (Fig. 8). It enabled us to confirm the diagnosis and to localise the lesion (Figs. 9 and 10). Computed tomography (CT) imaging of the neck and thorax aided diagnosis in ten patients (Fig. 11). Ultrasound examination of the neck done in two patients with occult airway trauma revealed laryngotracheal injuries (Fig. 12).

Intraoperative picture of the tracheal rent with a tube in situ

Chest roentgenogram showing subcutaneous emphysema over the chest

a Chest roentgenogram showing a right bronchial injury with fallen lung sign. b Computed tomography (CT) scan of the same patient with a collapsed right bronchus

Bronchoscopy findings in the patients

Bronchoscopic view of a tracheal rent

Bronchoscopic image of a bronchopleural fistula seen adjacent to the right bronchus

CT scan showing the rent in the anterior wall of the trachea at the 12 o’clock position with pneumomediastinum

Ultrasound image (long-axis view) showing tracheal disruption
Airway management (Fig. 13)
In all patients with LTBI, airway control was given prime importance according to the ATLS® protocol. While securing the airway, care was taken to provide cervical immobilisation, either by using manual in-line stabilisation (MILS) or by applying a semi-rigid cervical collar. Supplemental oxygen was provided throughout evaluation and management.

Airway management of LTBI cases in the emergency room (ER) and the operating room (OR)
Extrathoracic trachea
Emergency room
Five patients with extrathoracic laryngotracheal injury were referred from other centres with a tracheostomy tube in situ. In seven other patients, the tracheostomy tube was inserted through the visible rent. Urgent tracheostomy was done in two patients, as they presented with stridor. Direct laryngoscopic-aided intubation was done in three patients.
Operating room
Seven patients with signs suggestive of LTBI presented to the ER in a stable condition. These patients were shifted to the operating room (OR) for further management. One patient had to undergo urgent tracheostomy as he developed respiratory distress on being moved to the OR. Six patients underwent fibreoptic bronchoscope (FOB)-aided intubation after examination of the airway. This was facilitated using the nebulisation/spray as you go (SAGO) technique. Bronchoscopic examination of the laryngotracheal tree was done under sevoflurane anaesthesia in a paediatric patient, followed by intubation.
Intrathoracic trachea
Emergency room
One patient with intrathoracic tracheal injury presented 6 h after injury. He was referred from a peripheral centre and was hypoxic on arrival to the ER, as he was moved while wearing a face mask. Direct laryngoscopic-assisted intubation was done on an emergent basis.
Operating room
The airway was secured in five patients with intrathoracic tracheobronchial injury in the OR. Fibreoptic bronchoscope-aided intubation was done in three of these patients after pre-oxygenation. In two patients, the airway was anaesthetised by nerve blocks, while the other patient was induced using sevoflurane with maintenance of spontaneous breathing. The endotracheal tube was passed distal to the rent in two patients, while in one, it was inserted in the contralateral bronchus. Direct laryngoscopic-assisted intubation on an emergent basis was done in two patients, as they developed hypoxia on arrival to the OR.
Anaesthetic management
Induction and ventilation
In patients who were shifted from the ER with the airway secured, anaesthesia was administered through the endotracheal tube/tracheostomy tube. In all the patients, we ensured that the chest tube drains were patent before the induction of anaesthesia. In patients whose trachea was intubated in the OR, spontaneous ventilation was maintained till the airway was secured and the position of the endotracheal tube checked. In patients who underwent tracheal reconstruction, the surgeon guided the orotracheal tube to the distal part of the trachea, followed by reconstruction of the trachea with the tube in situ. Air was used in all the patients instead of nitrous oxide. Balanced anaesthesia technique using inhalation agent, neuromuscular blocking agent and opioid was administered in all the patients.
Monitoring
Standard monitoring such as pulse oximeter, non-invasive blood pressure, electrocardiography and EtCO2 were used in all the patients. Invasive arterial/central venous pressure monitoring was done in patients with haemorrhagic shock (two) or those who were scheduled for major surgeries (three thoracotomy, two tracheal reconstructions, two laryngectomy).
Intraoperative complications
Two patients presented with haemorrhagic shock due to associated vascular injury. Aggressive fluid resuscitation and transfusion of blood products was done in these patients. One patient with intrathoracic tracheal rent presented with hypoxia and developed bradycardia and cardiac arrest while securing the airway. He was revived once the airway was secured. One patient in whom fibreoptic-aided endobronchial intubation was done experienced a decrease in oxygen saturation intraoperatively. The position of the tube was readjusted using FOB and adequate suctioning was done. The oxygen saturation improved thereafter.
Surgical management
In 16 patients with extrathoracic LTBI, debridement and primary repair of the wound with temporary tracheostomy was done. Seven patients underwent permanent tracheostomy, since it was not possible to restore the normal anatomy of the laryngotracheal tree. This was due to complete traumatic laryngeal disruption. Oesophageal injury was noted in four of these patients, which necessitated a feeding jejunostomy for nutritional support. Intrathoracic injury in three patients required thoracotomy and primary repair. In one patient who had presented with bronchopleural fistula (BPF), bronchoscopic-aided glue (cyanoacrylate) instillation of the fistulous track was done.
Conservative management
No surgical intervention was needed in three patients, owing to the small size of the rent which spontaneously healed as observed on repeat bronchoscopy (one extrathoracic, two intrathoracic). Prophylactic antibiotics and antitussives were given to these patients and they were closely monitored for any signs of sepsis.
Postoperative management
Postoperative intensive care monitoring was required in 16 (53 %) patients (5 intrathoracic, 11 extrathoracic), due to the critical preoperative status, the grievous associated injuries and eventful intraoperative course in these patients. In patients with intrathoracic injuries, the median ventilator days and intensive care unit (ICU) stay days were 15 and 19, respectively. Pressure-regulated volume control (PRVC)/pressure control ventilation (PCV) mode of ventilation was preferred in these patients to avoid barotrauma. Positive end expiratory pressure (PEEP) was avoided in these patients. Aggressive pain management was instituted to facilitate early weaning. Thoracic epidural analgesia was administered in two patients who underwent thoracotomy. In the other patient who had spine fracture and underwent thoracotomy, intravenous analgesics were administered. In patients with extrathoracic laryngotracheal injury, the median time on a ventilator and length of ICU stay were 2 and 5 days, respectively. The median stay in hospital was 11 days in patients with extrathoracic injury and 38 days in patients with intrathoracic injury.
Early nutritional support was instituted in all the patients. In patients who had undergone reconstruction, feeding was done in the sitting position with the neck flexed. We had a high index of suspicion of wound dehiscence in all these patients. They were continuously assessed for fresh air leaks, increasing subcutaneous emphysema and pneumomediastinum. In patients with oesophageal injury, feeding jejunostomy was done for nutritional support (n = 4). One patient developed a tracheoesophageal fistula, which was confirmed with endoscopy and surgical repair was performed.
Outcome
The mortality rate was 6.6 %. One of the two patients expired in the OR because of hypoxia as a consequence of delayed presentation. The other patient succumbed secondary to multiple associated injuries and postoperative sepsis (45 days after admission). Seven patients had to undergo permanent tracheostomy as the larynx was completely disrupted due to trauma. Five patients had postoperative sepsis, of which four recovered. One patient whose tracheostomy was decannulated presented a few months later on follow-up with dyspnoea and wheeze. Flexible bronchoscopy revealed tracheal stenosis distal to the site of injury. Laser fulguration with subsequent bougie dilatation was performed, with good results. One patient who had undergone bronchial repair had a failure of anastomosis due to delayed presentation and sepsis. The time interval to diagnosis, mechanism, anatomic location and associated injuries were all evaluated as possible risk factors for hospital stay and outcome. Intrathoracic location of the injury showed a significant increase in the length of stay in the ICU (p-value = 0.0230). Also, the ISS had a direct correlation with the length of ICU stay. There was no significant association between the time interval for diagnosis or the mechanism of injury to morbidity or to the length of hospital stay.
Discussion
The first case of a long-term human survivor with LTBI was reported by Krinitzki [4]. The first successful repair of bronchial injury was reported 20 years later in 1947 by Kinsella and Johnsrud [5]. Following this, it has been demonstrated that the early diagnosis and primary repair of these injuries lead to less morbidity and mortality [3]. Of the patients with TBI, 30–80 % die before reaching the hospital, hence, making it difficult to ascertain the true incidence of such injuries [6]. Some of the injuries are so small that they go unnoticed [7]. On the basis of autopsy reports, 2.5–3.2 % of patients who die as a result of trauma may have associated TBI [1]. However, with the improvement in pre-hospital care facilities and the implementation of ATLS® protocols, the outcome in these patients is improving [3].
The diagnosis of major airway injury depends on a thorough history and physical examination. Careful inspection of the site of injury is essential to aid the diagnosis of occult airway injuries. In case of penetrating neck trauma, air leak from the wound confirms laryngotracheal injury [8]. Eleven of our patients had air leak from their neck wound. Difficulty in breathing and subcutaneous emphysema are the most common findings [9]. The incidence of these symptoms in our patients was 70 %. Reports of laryngotracheal injury due to accidental strangulation (dupatta, scarf) have been described in the literature [10]. We encountered four patients with a similar mechanism of injury. In one patient, the presence of a ligature mark around the neck prompted us to be highly suspicious of airway injury. Gunshot injuries are associated with greater local area damage, as was evident in our series [11].
A correct interpretation of the chest roentgenogram is imperative to enable the early diagnosis of occult airway injuries. The preponderant findings on chest radiograph include subcutaneous emphysema, pneumomediastinum and pneumothorax [12]. Baumgartner et al. [13], in their series of nine patients, stated subcutaneous emphysema as being one of the most consistent findings of TBI. This is similar to our study wherein subcutaneous emphysema was found in more than 70 % of the patients.
Bronchoscopy is the most reliable method to diagnose, locate and determine the severity of TBI [1] and to confirm the placement of an endotracheal tube. Bronchoscopy was used in 12 patients in our series, aiding endotracheal tube positioning, for confirmation of the location and extent of injury, and for postoperative pulmonary toileting. Our study reinforced the findings of Rossbach et al. [8], who had stated that a high index of suspicion and liberal use of bronchoscopy were essential in diagnosing occult airway injuries. Air leak from the tear and visualisation of the tear itself were confirmatory findings. A bronchoscope was also used as a therapeutic modality in one of our patients to seal BPF using tissue glue. Low cost and convenience make FOB-guided glue instillation a good option in patients with poor general condition [14]. Bronchoscopy also proved to be useful as a diagnostic and therapeutic modality of long-term complications, such as stenosis. In our series, ultrasonography aided diagnosis in two patients.
The direct insertion of an endotracheal tube through the rent itself enabled us to secure the airway in seven patients. It has been suggested that it is the easiest way to secure the airway in patients with open laryngotracheal wounds [15]. Two of our patients underwent urgent tracheostomy since they presented with severe respiratory distress. Urgent tracheostomy has been recommended in patients presenting with respiratory distress or in those where unsuccessful attempts were made to secure the airway using a bronchoscope [16]. In one of our patients with bronchial injury, we inserted the endotracheal tube into the contralateral bronchus. Either of the techniques of one-lung isolation (endobronchial intubation/double-lumen tube) could be used to reduce air leak and provide effective ventilation and adequate surgical exposure [17]. The insertion and final placement of these tubes should be done under FOB guidance, as blind insertion can further traumatise the airway and cause obstruction [16].
Intraoperative management of these patients is challenging, as the anaesthesiologist shares the airway with the surgeons [18]. Successful outcome depends on the close cooperation between the two. Extubation of the trachea has been recommended as early as possible after tracheal reconstruction. In our series, we were able to extubate one patient immediately postoperatively, with the others within 24 h after surgery. In patients requiring postoperative ventilation, the PRVC/PCV mode of ventilation was used to limit high-pressure/volume-induced damage of the lung. Several authors recommend the avoidance of high airway pressures and PEEP, as there is a chance of wound dehiscence [19]. In patients with persistent air leak, the use of a cuirass ventilator or high-frequency ventilation has been used to achieve a low airway pressure [20]. Effective pain relief in patients undergoing thoracotomy is mandatory to ensure adequate ventilation and secretion clearance [15]. An epidural catheter was inserted in two patients who underwent thoracotomy. Prophylactic broad-spectrum antibiotics were used to prevent wound infection [16].
Associated injuries related to the mechanism of injury were common in our series. The most common injury related to penetrating trauma in our series was oesophageal perforation, which is consistent with other reports [21]. Associated injuries play an important role in the outcome [22]. This was evident in our series wherein the ISS had a direct correlation with the morbidity. In our series, delay in presentation was not associated with poorer outcomes. This is contradictory to other reports, wherein early diagnosis leads to less mortality and morbidity [23]. This can probably be attributed to more than 60 % of our patients being referrals from other centres, where primary treatment had already been provided in the majority of them prior to transportation to our centre. Richardson [24], in his study, highlighted the long-term outcomes of patients with LTBI over a period of 26 years. In our data, only one patient presented with tracheal stenosis few months after the injury. This could be due to the limited period (3 years) taken into account in our study.
In summary, major surgery on the trachea and airway is an anaesthetic challenge which necessitates the simultaneous control of the airway and maintenance of gas exchange. Advance planning, good communication and teamwork among anaesthesiologists, surgeons and operating theatre personnel are important. Despite improvements in the specialised services for trauma patients and progress in respiratory resuscitation, LTBI remains a serious problem. Subcutaneous emphysema, pneumothorax and pneumomediastinum should raise the suspicion of airway injuries. Endotracheal tube insertion through the rent is the simplest and quickest way to provide oxygenation and ventilation. Bronchoscopic-assisted intubation, whenever possible, is recommended in airway trauma. One-lung ventilation should be achieved and maintained in bronchial injuries. Small-sized leaks in the trachea can be managed conservatively. Ventilator adjustment strategies should be adopted in intrathoracic airway injuries to limit airway pressures for better outcomes. A good team comprising experienced anaesthesiologists and surgeons is essential for a successful outcome.
References
Johnson SB. Tracheobronchial injury. Semin Thorac Cardiovasc Surg. 2008;20:52–7.
Hancock BJ, Wiseman NE. Tracheobronchial injuries in children. J Pediatr Surg. 1991;26:1316–9.
Cassada DC, Munyikwa MP, Moniz MP, Dieter RA Jr, Schuchmann GF, Enderson BL. Acute injuries of the trachea and major bronchi: importance of early diagnosis. Ann Thorac Surg. 2000;69:1563–7.
Krinitzki SI. Zur Kasuistik einer vollstandigen Zerreissung des rechten Luftrohrenastes. Virchows Arch. 1928;266:815–9.
Kinsella TJ, Johnsrud LW. Traumatic rupture of the bronchus. J Thorac Surg. 1947;16:571–83.
Burke JF. Early diagnosis of traumatic rupture of the bronchus. JAMA. 1962;181:682–6.
Glazer ES, Meyerson SL. Delayed presentation and treatment of tracheobronchial injuries due to blunt trauma. J Surg Educ. 2008;65:302–8.
Rossbach MM, Johnson SB, Gomez MA, Sako EY, Miller OL, Calhoon JH. Management of major tracheobronchial injuries: a 28-year experience. Ann Thorac Surg. 1998;65:182–6.
Barmada H, Gibbons JR. Tracheobronchial injury in blunt and penetrating chest trauma. Chest. 1994;106:74–8.
Gowens PA, Davenport RJ, Kerr J, Sanderson RJ, Marsden AK. Survival from accidental strangulation from a scarf resulting in laryngeal rupture and carotid artery stenosis: the “Isadora Duncan Syndrome”. A case report and review of literature. Emerg Med J. 2003;20:391–3.
Sulek M, Miller RH, Mattox KL. The management of gunshot and stab injuries of the trachea. Arch Otolaryngol. 1983;109:56–9.
Unger JM, Schuchmann GG, Grossman JE, Pellett JR. Tears of the trachea and main bronchi caused by blunt trauma: radiologic findings. Am J Roentgenol. 1989;153:1175–80.
Baumgartner F, Sheppard B, de Virgilio C, Esrig B, Harrier D, Nelson RJ, Robertson JM. Tracheal and main bronchial disruptions after blunt chest trauma: presentation and management. Ann Thorac Surg. 1990;50:569–74.
McManigle JE, Fletcher GL, Tenholder MF. Bronchoscopy in the management of bronchopleural fistula. Chest. 1990;97:1235–8.
Pate JW. Tracheobronchial and esophageal injuries. Surg Clinic North Am. 1989;69:111–23.
Devitt JH, Boulanger BR. Lower airway injuries and anaesthesia. Can J Anaesth. 1996;43:148–59.
Ramzy AI, Rodriguez A, Turney SZ. Management of major tracheobronchial ruptures in patients with multiple system trauma. J Trauma. 1988;28:1353–7.
Huang J, Needs RE, Miller HAB, Devitt JH. Unsuspected tracheal rupture in blunt thoracic trauma. Can J Anaesth. 1994;41:1208–10.
Ishikawa S, Onizuka M, Matsumaru Y, Yamada T, Tsukada A, Mitsui K, Hori M. Successful reconstruction for combined tracheal and bronchial disruption. Ann Thorac Surg. 1993;56:160–1.
Chu CPW, Chen PP. Tracheobronchial injury secondary to blunt chest trauma: diagnosis and management. Anaesth Intensive Care. 2002;30:145–52.
Feliciano DV, Bitondo CG, Mattox KL, Romo T, Burch JM, Beall AC Jr, Jordan GL Jr. Combined tracheoesophageal injuries. Am J Surg. 1985;150:710–5.
Karmy-Jones R, Wood DE. Traumatic injury to the trachea and bronchus. Thorac Surg Clin. 2007;17:35–46.
Cassada DC, Munyikwa MP, Moniz MP, Dieter RA Jr, Schuchmann GF, Enderson BL. Acute injuries of the trachea and major bronchi: importance of early diagnosis. Ann Thorac Surg. 2000;69:1563–7.
Richardson JD. Outcome of tracheobronchial injuries: a long-term perspective. J Trauma. 2004;56:30–6.
Acknowledgments
Our sincere thanks go to Dr. Sanjeev Bhoi, Associate Professor, Medicine and ER In-charge, for his invaluable contribution to this study. We acknowledge Chaman Singh, Narayan Singh and Naresh Kumar for their technical support and help.
Conflict of interest
No external funding and no competing interests are declared.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Gupta, B., Sinha, C., Kumar, A. et al. Perioperative management of laryngotracheobronchial injury: our experience in a level 1 trauma centre. Eur J Trauma Emerg Surg 38, 553–561 (2012). https://doi.org/10.1007/s00068-012-0199-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00068-012-0199-5