
Abstract
Background
There is sparse research reporting effective interventions for preventing nausea and emesis caused by concurrent chemoradiotherapy (CCRT) in locally advanced head and neck squamous cell carcinoma (LA-HNSCC).
Methods
Treatment-naïve LA-HNSCC patients received intensity-modulated radiotherapy with concomitant cisplatin 100 mg/m2 (33 mg/m2/days [d]1–3) every 3 weeks for two cycles. All patients were given oral aprepitant 125 mg once on d1, then 80 mg once on d2–5; ondansetron 8 mg once on d1; and dexamethasone 12 mg once on d1, then 8 mg on d2–5. The primary endpoint was complete response (CR). Pursuant to δ = 0.2 and α = 0.05, the expected CR rate was 80%.
Results
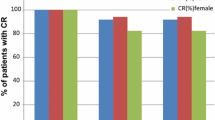
A total of 43 patients with LA-HNSCC were enrolled. The median age was 53 years, and 86.0% were male. All patients received radiotherapy and 86.0% of patients completed both cycles as planned. The overall CR rate was 86.0% (95% confidence interval [CI]: 72.1–94.7). The CR rates for cycles 1 and 2 were 88.4% (95% CI: 74.9–96.1) and 89.2% (95% CI: 74.6–97.0). The complete protection rate in the overall phase was 72.1% (95% CI: 56.3–84.7). The emesis-free and nausea-free responses in the overall phase were 88.4% (95% CI: 74.9–96.1) and 60.5% (95% CI: 44.4–75.0), respectively. The adverse events related to antiemetics were constipation (65.1%) and hiccups (16.3%), but both were grade 1–2. There was no grade 4 or 5 treatment-related toxicity with antiemetic usage.
Conclusion
The addition of aprepitant into ondansetron and dexamethasone provided effective protection from nausea and emesis in patients with LA-HNSCC receiving radiotherapy and concomitant high-dose cisplatin chemotherapy.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Against the background of advances in new antiemetic agents, the efficacy of antiemetics in preventing chemotherapy-induced nausea and vomiting (CINV) has been substantially improved [1]. Aprepitant was the first neurokinin‑1 receptor antagonist (NK1RA) that blocks the binding of substance P to prevent emesis. The addition of NK1RA improved complete response (no emesis and no rescue medication) by 8–20% after highly emetogenic chemotherapy (HEC) [2]. The current Multinational Association of Supportive Care in Cancer/European Society for Medical Oncology (MASCC/ESMO) and National Comprehensive Cancer Network (NCCN) guidelines also recommend a triple regimen consisting of 5-hydroxytryptamine (HT)3 receptor antagonist (5-HT3RA), dexamethasone, and NK1RA to prevent nausea and vomiting induced by HEC, e.g., cisplatin [3]. Conversely, little focus has centered on antiemetic prophylaxis in radiotherapy. As a result, radiation-induced nausea and vomiting (RINV) is often underestimated by clinicians [4]. A cross-sectional study demonstrated that one third of patients experiencing RINV would like additional treatment [5]. Nevertheless, evidence for the guideline recommendations is scarce, and little is known about the combination and optimal duration of antiemetic agents [6]. In the chemoradiotherapy setting, RINV can be exacerbated by concomitant chemotherapy to higher levels, which has been confirmed by prior studies, though the pathophysiological mechanism is not well understood [7,8,9].
With regard to locally advanced head and neck squamous cell carcinoma (LA-HNSCC), cisplatin-based concurrent chemoradiotherapy (CCRT) remains the standard treatment modality. However, nausea and vomiting induced by CCRT are common toxicities, with deleterious effects on treatment compliance and quality of life. Several prospective studies have demonstrated that the incidences of nausea and vomiting during cisplatin-based CCRT are 48–66% and 30–47%, respectively [10,11,12,13]. Thus, there is a pressing need for optimization of antiemetic treatment to address chemoradiotherapy-induced nausea and vomiting (C-RINV). Recent evidence has emerged that NK1RAs improve the control of C‑RINV in certain tumors. To date, only five published prospective studies have reported the efficacy and safety of NK1RAs for the prophylaxis of C‑RINV, two of which focused on cervical cancer and the remainder included multiple-site tumors [14,15,16,17,18]. The above mentioned studies demonstrated the superiority of NK1RAs in the prevention of nausea and vomiting as well as their high tolerability, yet whether different tumors, various chemotherapy regimens, and different radiation schedules would yield similar results remains unknown.
In our preliminary trial, 13 patients with LA-HNSCC receiving CCRT with triweekly cisplatin were administrated with triple antiemetic regimen consisting of NK1RA (aprepitant), 5‑HT3RA (ondansetron), and dexamethasone. The results showed that only 1 patient developed vomiting and 2 patients required rescue antiemetic treatment. No significant adverse event was observed. On the basis of the above results, a prospective trial was conducted to explore whether the addition of aprepitant could provide effective protection against C‑RINV in patients with LA-HNSCC.
Materials and methods
Study design and participants
This study (ClinicalTrials.gov, number NCT03572829) was investigator initiated and designed as a prospective single-arm, open-label phase II trial to evaluate the efficacy and safety of aprepitant combined with ondansetron and dexamethasone for the prevention of nausea and vomiting induced by concurrent chemoradiotherapy in LA-HNSCC. All patients were fully informed about the study and signed informed consent. The study was conducted in accordance with the Declaration of Helsinki and the international standards of Good Clinical Practice and approved by the local ethics committee.
The eligible patients were aged 18 to 70 years with histologically confirmed squamous cell carcinoma of the head and neck (nasopharynx, oral cavity, oropharynx, hypopharynx, larynx, nasal cavity, and paranasal sinuses), and were stage II-IVB for a nasopharyngeal site or stage III-IVB for other sites based on the American Joint Committee on Cancer 7th Edition (AJCC 7th). Patients had the Eastern Cooperative Oncology Group (ECOG) performance status 0–1; had adequate organ and bone marrow function; were able to swallow tablets; had a life expectancy of at least 12 weeks; and would receive CCRT as planned after multidisciplinary team (MDT) discussion. Fertile male and female patients volunteered to use effective contraception during the study and within 90 days of the last medication. The exclusion criteria included other medical histories of malignancy apart from non-melanoma skin cancer, cervical carcinoma in situ, and early-stage cured prostate cancer; nausea and emesis occurred 24 h before the start of CCRT; corticosteroid or benzodiazepines used; any medicine which affected metabolism through drug-metabolizing enzymes CPY3A4 and CYP2D6 except for nighttime sedatives; severe cardiovascular, pulmonary, diabetic, mental, and other diseases; perinatal women or rejection of taking contraception during treatment; drug and/or alcohol addiction; symptomatic brain metastasis; gastrointestinal obstruction; hypocalcemia or any other conditions that could provoke emesis.
Procedures
Intensity-modulated radiotherapy (IMRT) using simultaneously integrated boost was administered to all patients. Target delineation and dose prescription followed the principles of radiotherapy for head and neck cancer at our center [19]. The delineation of normal organs adhered to the international consensus on delineation of organs at risk in the head and neck regions [20], and the standard of dose limitation referred to the Quantitative Analyses of Normal Tissue Effects in the Clinic (QUANTEC). Concurrent chemotherapy was administrated with cisplatin 100 mg/m2 (33 mg/m2/days 1–3) every 3 weeks for two cycles. All patients received hydration and diuretic therapy during the administration of cisplatin. The chemotherapy-induced toxicities had to be restored to grade 0–2 prior to the start of the subsequent cycle. Chemotherapy was terminated if the toxicities were not restored to grade 0–2 within 14 days of the beginning of the next cycle. If grade 4 hematological toxicities or ≥ grade 3 non-hematological toxicities occurred in the previous cycle, the dose of the subsequent cycle was reduced by 25%.
The recruited patients were subjected to unified antiemetic treatment (Fig. 1). The doses, duration, and scheduling of antiemetics in our study basically followed the MASCC/ESMO guidelines for multiple-day cisplatin chemotherapy and high-emetic-risk chemotherapy [2, 21]. A combination of ondansetron, dexamethasone, and aprepitant was applied for acute nausea and vomiting, and dexamethasone and aprepitant for delayed nausea and vomiting. All patients were given oral aprepitant 125 mg once on day 1, then 80 mg once on days 2–5; intravenous ondansetron 8 mg once on day 1; and oral dexamethasone 12 mg once on day 1, then 8 mg on days 2–5. The antiemetic regimen was maintained in the subsequent cycle until chemotherapy was stopped or severe drug-related side effects occurred. Rescue antiemetic therapy was permitted for grade 3 nausea (National Cancer Institute Common Toxicity Criteria for Adverse Events, NCI CTCAE, version 4.0) or poor antiemetic effects (criteria: emesis > 2 times/24 h, and continuous vomiting within 5 min is regarded as one time).

The trial procedure. IMRT intensity-modulated radiotherapy, QOL quality of life
Assessment
Patients were asked to complete daily diaries per cycle that recorded nausea, vomiting, or dry retches, including the time, frequency, degree, or score, and application of rescue medication. The treatment-related toxicities were evaluated according to NCI CTCAE version 4.0. To assess the degree of nausea and vomiting, the MASCC Antiemesis Tool (MAT) scale was completed respectively by patients during chemotherapy and during the period from the second day to the fourth day after the last administration of cisplatin. At baseline and on day 7 of the first cycle and the second cycle, the Functional Living Index—Emesis (FLIE) questionnaire was employed to evaluate the effect of nausea and emesis on quality of life. The overall quality of life was assessed each week during treatment (week 1–7) using the questionnaires of the European Organisation for Research and Treatment of Cancer (EORTC), Quality of Life Core 30 items (QLQ-C30) version 3.0 and Quality of Life Head and Neck 35 items (QLQ-H&N35) version 1.0.
Outcomes
The primary endpoint was complete response (CR), defined as no emesis and no use of rescue therapy during concurrent chemoradiotherapy. The secondary endpoints were as follows: CR for each cycle; complete protection (CP), denoted as no emesis, no rescue medication, and no more than mild nausea (grade 1 premised on CTCAE 4.0); emesis-free response, which refers to no vomiting or dry retches during treatment; nausea-free response, signified as no nausea during treatment; and treatment-related toxicities. Other secondary endpoints consisted of the degree of nausea and vomiting evaluated by the MAT scale, as well as the quality of life using the FLIE, EORTC QLQ-C30, and QLQ-H&N35 questionnaires (results not reported here).
Statistical analysis
The Simon two-stage design was adopted to estimate the sample size [22]. Pursuant to δ = 0.2 and α = 0.05, the expected CR rate was 80%. If the CR was less than 60%, the study protocol was declared invalid. In the first stage, 17 patients were enrolled. If more than 13 patients achieved CR, 26 patients would remain enrolled.
Demographic and clinical characteristics were outlined using the median (range) for continuous variables and frequency (percentage) for categorical variables. The percentages of patients with CR or CP, emesis-free response, and nausea-free response for every cycle and the overall phase were estimated along with 95% confidence intervals (CIs). The corresponding 95% CIs were calculated using the binomial test of one-sample nonparametric tests. The treatment-related toxicities and adverse events were summarized as frequency (percentage). Statistical analyses were conducted using SPSS software (version 26.0; IBM Corp., Armonk, NY, USA).
Results
Between January 2018 and January 2020, 16 of 17 patients recruited in stage 1 achieved CR and, thereafter, 26 patients were further enrolled in stage 2. Baseline characteristics are reported in Table 1. The median age was 53 years (range 18–66) and 86.0% were male. 40 patients in total were treated with definitive CCRT, while the remaining 3 patients who were to receive planned definitive CCRT were re-examined and the efficacy thereof evaluated when the cumulative radiation dose reached around 50 Gy, followed by conversion to surgery after MDT discussion. The median radiation dose was 69.96 Gy (range 53–73.92 Gy). All patients received radiotherapy and the first cycle of cisplatin, while 6 patients did not receive the second cycle of chemotherapy (stopped chemotherapy early). Among the 37 patients who received the second cycle of chemotherapy, different degrees of delayed chemotherapy occurred in 21 (56.8%) patients (median 7 days; range 2–14 days). The reasons for delay or discontinuation are displayed in Table 2. Cisplatin dose changes were reported in 11 (29.7%) of 38 patients during the second cycle. All patients completed antiemetic treatment as planned.
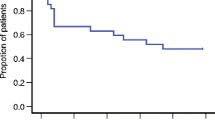
The overall CR rate of this study was 86.0% (95% CI: 72.1–94.7%), exceeding the expected CR rate. Table 3 lists the secondary efficacy endpoints. The CR rate for cycle 1 was 88.4% (95% CI: 74.9–96.1%), while there was a slightly higher CR rate (89.2%, 95% CI: 74.6–97.0%) for cycle 2. The CP rate in the overall phase was 72.1% (95% CI: 56.3–84.7%), while the data of cycle 1 and cycle 2 were 76.7% (95% CI: 61.4–88.2%) and 86.5% (95% CI: 71.2–95.5%), respectively.
The emesis-free response in the overall phase was 88.4% (95% CI: 74.9–96.1%). The emesis-free response rates for cycle 1 and 2 were 90.7% (95% CI: 77.9–97.4%) and 91.9% (95% CI: 78.1–98.3%), respectively. Out of the 5 patients with emesis, grade 2 emesis occurred in 3 patients, the remaining 2 patients experienced grade 1 emesis, and all patients did not receive rescue antiemetics. The distribution of patients with different grades of emesis is depicted in Fig. 2. The median time from cisplatin administration to emesis was 3 days (day 1–day 6), while the median duration time of emesis was 2 days (1–6 days).

The distribution of patients with different grades of emesis
The nausea-free response in the overall phase was 60.5% (95% CI: 44.4–75.0%). The nausea-free response rate for cycle 1 was also 60.5% (95% CI: 44.4–75.0%), whereas the incidence of no nausea for cycle 2 increased by nearly 18% (78.4%; 95% CI: 61.8–90.2%). The distribution of patients with different grades of nausea appertaining to the nausea visual analog scale (NVAS) is reported in Fig. 3 (1–3 points: 7 cases; 4–6 points: 7 cases; 7–10 points: 3 cases). The median score of nausea founded on the NVAS was 4 points (range 1–10). Regarding the patients with nausea, the same one patient developed severe nausea (NVAS score up to 10 points) in both cycles and was administrated rescue treatment. The median time of the nausea episode was 2 days (day 1–day 6), while the median duration time of nausea was 3 days (1–7 days).

The distribution of patients with different grades of nausea based on the NVAS score
Table 4 depicts all treatment-related toxicities during the entire treatment time. Grade 1–2 toxicities that presented in at least 10% of patients included dermatitis, mucositis, dry mouth, leucopenia, anemia, hepatic dysfunction, fatigue, and appetite loss. The most frequent grade 3 toxicities were mucositis (20.9%) and leucopenia (14.0%). Grade 3 dermatitis, hepatic dysfunction, fatigue, and appetite loss were less than 5%, and no grade 4 or 5 adverse event was observed. The toxicities presumably related to antiemetics were constipation (65.1%) and hiccups (16.3%), but both were grade 1–2. The percentages and grades of toxicities related to the antiemetics per cycle are depicted in Fig. 4. Further, no infusion site infection or allergic reaction emerged during treatment.

The percentages and grades of toxicities related to the antiemetics
Discussion
To the best of our knowledge, this is the first prospective trial to evaluate the efficacy and safety of an NK1 receptor antagonist (aprepitant) combined with ondansetron and dexamethasone to prevent nausea and vomiting for patients with head and neck squamous cell carcinoma (HNSCC) receiving triweekly cisplatin chemoradiotherapy. The primary endpoint met the target, with the overall CR rate reaching 86.0%, revealing that the triple antiemetic regimen provided effective protection against chemoradiotherapy-induced nausea and vomiting in patients with LA-HNSCC. Prior research has indicated that the addition of an NK1RA to 5‑HT3RA and dexamethasone improves antiemetic efficacy in patients with cervical cancer receiving radiotherapy with weekly cisplatin chemotherapy [17, 23]. Similar results have now been found in patients with HNSCC receiving IMRT and triweekly cisplatin chemotherapy.
In the context of the concurrent chemotherapy regimen, two cycles of cisplatin rather than three cycles were not adopted in this study, mainly based on increased treatment-related toxicities, decreased compliance, and uncertainty of the benefit of the third dose of cisplatin in the high-dose triweekly concurrent regimen [24,25,26]. The 3‑day administration of cisplatin was primarily due to the naïve population tolerance and the recommendation of the local ethics committee, which had already been used in another large prospective trial [27].
The primary endpoint of the present trial was complete response, which has been used in most clinical antiemetic trials. “No emesis” represented the control of emesis, while “no use of rescue therapy” as an alternative marker also reflected control of nausea to a certain degree. In the present trial, only 5 patients experienced grade 1 to 2 emesis, and 1 patient with severe nausea received rescue treatment. Prior prospective studies on NK1RAs for prophylaxis of C‑RINV observed that the CR rate was between 48 and 76% [14,15,16, 18]. Contrary to the data of the above studies, our results exhibit that the triple antiemetic regimen achieved excellent antiemetic efficacy. One possible explanation is that the 5‑day antiemetic administration increased the cumulative dose of aprepitant and dexamethasone under the premise of multiple-day cisplatin chemotherapy, potentially having a stronger antiemetic effect. With regard to the secondary endpoints, CP is also a reliable endpoint to evaluate the overall control of nausea and vomiting, often being employed in clinical trials of CINV. The CP rate of this study reached 72%, which is higher than the data reported in several trials on aprepitant for prevention of CINV [28, 29]. However, the concept of “mild nausea” is not objective enough, whether it is based on grade 1 of CTCAE or NVAS < 25 mm [30]. Conversely, “no vomiting” and “no nausea” are relatively objective indicators, being adopted as secondary endpoints in our study. In the overall phase, 88.4% of patients developed no emesis, higher than the 66–73% reported in previous studies on NK1RAs for prevention of C‑RINV [15, 17, 18, 31]. Although the overall nausea-free response rate was only 60.5%, this is approximately consistent with the 40–61.5% reported in preceding research on NK1RAs for prevention of C‑RINV [16, 18, 31].
The control rates of nausea and vomiting under our triple antiemetic regimen were also superior to the data reported in previous studies on concurrent chemoradiotherapy for head and neck squamous cell carcinoma. Many studies have reported treatment-related toxicities such as nausea and vomiting while publishing primary endpoints, yet few studies specified the antiemetic regimens. In the RTOG 0129 trial [11], 361 patients were subjected to standard fractionation irradiation with a median dose of 69.8 Gy and concomitant triweekly cisplatin chemotherapy, and granisetron or ondansetron was used as the antiemetic regimen. In this condition, 65.9% of patients developed nausea and 46.8% of patients experienced vomiting. Further, the incidences of grade 3 nausea and grade 3–4 vomiting were both close to 20%. These results imply that single-agent 5‑HT3RAs were insufficient to control nausea and vomiting caused by concurrent chemoradiotherapy in head and neck squamous cell carcinoma. In a randomized phase 3 trial [13], the CCRT arm was subjected to radical radiotherapy (66–70 Gy) with concurrent weekly cisplatin (30 mg/m2). Employing ondansetron and dexamethasone as antiemetics, the overall incidences of nausea and vomiting were 47.7 and 30%, and the incidences of grade 3 nausea and grade 3–4 vomiting were only 1 and 1.5%. As well as the addition of dexamethasone, the reduction of nausea and vomiting could also be attributed to the weekly cisplatin chemotherapy regimen. A preceding meta-analysis compared weekly low-dose (≤ 50 mg/m2) and triweekly high-dose cisplatin (100 mg/m2) for CCRT in LA-HNSCC, and demonstrated that the weekly regimen led to a substantially lower proportion of severe nausea and/or vomiting (3 vs. 16%) [32]. However, the antiemetic efficacy was still superior to the above study under the premise of administrating the stronger emetic triweekly cisplatin regimen in the present study, illustrating that the addition of aprepitant to ondansetron and dexamethasone could more effectively control nausea and vomiting. In a further randomized phase III trial [27], Tang et al. also divided 100 mg/m2 of cisplatin into 3 days, and the antiemetic regimen stipulated adding metoclopramide on the basis of ondansetron/granisetron and dexamethasone. The proportion of patients with nausea and vomiting were both around 80%; whereas the incidence of grade 3 nausea was only 9%, the incidence of grade 3–4 vomiting was up to 18%. Numerically, although the triple regimen containing metoclopramide could be more effective in preventing severe nausea, poor prevention of the overall occurrence of nausea and vomiting was demonstrated, in addition to failure to effectively prevent severe vomiting. Conversely, the majority of patients with nausea presented mainly mild and moderate levels in the present study. Despite determination of the degree of nausea being subjective, only 1 patient required rescue antiemetics, and no patient discontinued treatment due to nausea or vomiting, thereby objectively illustrating that the triple regimen containing aprepitant could effectively control the occurrence of severe nausea and vomiting.
Recently, another prospective study evaluating the antiemetic efficacy of aprepitant in patients with LA-HNSCC receiving radiotherapy and concurrent weekly cisplatin (50 mg/m2) chemotherapy was exhibited at the 2020 Annual Meeting of the American Society of Clinical Oncology (ASCO) [31]. The incidences of no nausea and no vomiting were 57.7 and 73.2%, respectively, in patients receiving aprepitant, 5‑HT3RA, and steroids. The similar antiemetic regimen demonstrated poorer control of nausea and vomiting during concurrent weekly cisplatin and radiation compared with our study. In general, whether horizontally compared with the studies of NK1RAs for prophylaxis of C‑RINV or longitudinally compared with prior studies of CCRT for head and neck squamous cell carcinoma, our study administrated a triple antiemetic regimen consisting of aprepitant, ondansetron, and dexamethasone and presented high antiemetic efficacy. However, the incidence of nausea in our study notably remained close to 40%. A small randomized controlled trial has revealed that the addition of olanzapine increased the control rate of nausea from 40 to 71% [16]. In future research, we will consider adding olanzapine to optimize this antiemetic regimen.
In terms of treatment compliance and toxicities, 86.0% of patients completed both cycles of chemotherapy in the present study. Of the 6 patients who discontinued chemotherapy, only 3 did so as a result of treatment-related adverse events. Owing to the antiemetics that were given together with cisplatin, it was difficult to classify adverse events into antiemetic-related or cisplatin-related, especially fatigue, appetite loss, and hepatic dysfunction. Nevertheless, constipation and hiccups, with incidences of 65.1 and 16.3%, respectively, were primarily regarded as antiemetic-related adverse events. The high incidence of constipation could be attributed to an increase in cumulative dose for 5‑day administration of antiemetics, in addition to the non-use of prophylactic laxatives. Dexamethasone-induced hiccups are not an uncommon symptom in patients with cancer, Vardy et al. reported a 25% incidence of hiccups after dexamethasone administration [33]. Liaw et al. also discovered that more than 40% of patients treated with cisplatin developed hiccups, and 90% of hiccups eased after discontinuation of dexamethasone [34]. In contrast to the data of the above studies, the incidence of hiccups in the present study was not unacceptable. A randomized trial confirmed that replacing dexamethasone with methylprednisolone does not compromise the antiemetic efficacy but reduces the occurrence of hiccups. Hence, if there is a concern that hiccups could affect the quality of life, using methylprednisolone instead of dexamethasone could also be considered [35]. Although grade 3 mucositis and leucopenia also exceeded 10%, both toxicities were recognized as being related to concurrent chemoradiotherapy. Overall, the present study demonstrated that the triple regimen is still well tolerated in HNSCC patients.
Notwithstanding the above, several limitations still exist in the present study. Firstly, the 5‑day antiemetic regimen in the present study was designed based on the 3‑day administration of cisplatin. Thus, for the more extensively used single-day cisplatin administration, the question of whether this triple antiemetic regimen can achieve the same efficacy as in the present study requires further research. Further, the present study was a single-arm phase II trial without an optimal control group. When analyzing the efficacy, only comparison with historical data was possible. For this reason, further phase III randomized controlled trials must be conducted in the future.
Conclusion
The present study extends the combination of aprepitant, ondansetron, and dexamethasone as antiemetic prophylaxis to patients with HNSCC receiving IMRT and high-dose cisplatin chemotherapy. The addition of aprepitant into ondansetron and dexamethasone provides effective protection from emesis and nausea in patients with LA-HNSCC receiving radiotherapy and concomitant high-dose cisplatin chemotherapy. Treatment-related toxicities are mainly mild to moderate and tolerable. Randomized phase III studies are required to further define the potential role of NK1RAs in a chemoradiotherapy setting for HNSCC.
Change history
24 June 2022
In this article the title was incorrectly given as “Antiemetic prophylaxis for chemoradiotherapy-induced nausea and vomiting in locally advanced head and heck squamous cell carcinoma: a prospective phase II trial” but should have been “Antiemetic prophylaxis for chemoradiotherapy-induced nausea and vomiting in locally advanced head and neck squamous cell carcinoma: a prospective phase II trial”.
References
Navari RM, Aapro M (2016) Antiemetic prophylaxis for chemotherapy-induced nausea and vomiting. N Engl J Med 374:1356–1367. https://doi.org/10.1056/NEJMra1515442
Herrstedt J, Roila F, Warr D et al (2016) Updated MASCC/ESMO consensus recommendations: prevention of nausea and vomiting following high emetic risk chemotherapy. Support Care Cancer 2017(25):277–288. https://doi.org/10.1007/s00520-016-3313-0
Razvi Y, Chan S, McFarlane T et al (2019) ASCO, NCCN, MASCC/ESMO: a comparison of antiemetic guidelines for the treatment of chemotherapy-induced nausea and vomiting in adult patients. Support Care Cancer 27:87–95. https://doi.org/10.1007/s00520-018-4464-y
Feyer P, Jahn F, Jordan K (2015) Prophylactic management of radiation-induced nausea and vomiting. Biomed Res Int 2015:893013. https://doi.org/10.1155/2015/893013
Enblom A, Bergius Axelsson B, Steineck G et al (2009) One third of patients with radiotherapy-induced nausea consider their antiemetic treatment insufficient. Support Care Cancer 17:23–32. https://doi.org/10.1007/s00520-008-0445-x
Ruhlmann CH, Herrstedt J (2016) New treatments on the horizon for chemoradiotherapy-induced nausea and vomiting. Expert Opin Pharmacother 17:1623–1629. https://doi.org/10.1080/14656566.2016.1202923
Fraunholz I, Grau K, Weiss C, Rodel C (2011) Patient- and treatment-related risk factors for nausea and emesis during concurrent chemoradiotherapy. Strahlenther Onkol 187:1–6. https://doi.org/10.1007/s00066-010-2196-0
Maranzano E, De Angelis V, Pergolizzi S et al (2010) A prospective observational trial on emesis in radiotherapy: analysis of 1020 patients recruited in 45 Italian radiation oncology centres. Radiother Oncol 94:36–41. https://doi.org/10.1016/j.radonc.2009.11.001
Grunberg S, Chua D, Maru A et al (2011) Single-dose fosaprepitant for the prevention of chemotherapy-induced nausea and vomiting associated with cisplatin therapy: randomized, double-blind study protocol--EASE. J Clin Oncol 29:1495–1501. https://doi.org/10.1200/JCO.2010.31.7859
Ang KK, Zhang Q, Rosenthal DI et al (2014) Randomized phase III trial of concurrent accelerated radiation plus cisplatin with or without cetuximab for stage III to IV head and neck carcinoma: RTOG 0522. J Clin Oncol 32:2940–2950. https://doi.org/10.1200/JCO.2013.53.5633
Nguyen-Tan PF, Zhang Q, Ang KK et al (2014) Randomized phase III trial to test accelerated versus standard fractionation in combination with concurrent cisplatin for head and neck carcinomas in the Radiation Therapy Oncology Group 0129 trial: long-term report of efficacy and toxicity. J Clin Oncol 32:3858–3866. https://doi.org/10.1200/JCO.2014.55.3925
Noronha V, Joshi A, Patil VM et al (2018) Once-a-week versus once-every-3-weeks cisplatin chemoradiation for locally advanced head and neck cancer: a phase III randomized noninferiority trial. J Clin Oncol 36:1064–1072. https://doi.org/10.1200/jco.2017.74.9457
Patil VM, Noronha V, Joshi A et al (2019) A randomized phase 3 trial comparing nimotuzumab plus cisplatin chemoradiotherapy versus cisplatin chemoradiotherapy alone in locally advanced head and neck cancer. Cancer 125:3184–3197. https://doi.org/10.1002/cncr.32179
Jahn F, Riesner A, Jahn P et al (2015) Addition of the neurokinin-1-receptor antagonist (RA) aprepitant to a 5-hydroxytryptamine-RA and dexamethasone in the prophylaxis of nausea and vomiting due to radiation therapy with concomitant cisplatin. Int J Radiat Oncol Biol Phys 92:1101–1107. https://doi.org/10.1016/j.ijrobp.2015.04.037
Hanawa S, Mitsuhashi A, Matsuoka A et al (2016) Efficacy of palonosetron plus aprepitant in preventing chemoradiotherapy-induced nausea and emesis in patients receiving daily low-dose cisplatin-based concurrent chemoradiotherapy for uterine cervical cancer: a phase II study. Support Care Cancer 24:4633–4638. https://doi.org/10.1007/s00520-016-3306-z
Navari RM, Nagy CK, Le-Rademacher J, Loprinzi CL (2016) Olanzapine versus fosaprepitant for the prevention of concurrent chemotherapy radiotherapy-induced nausea and vomiting. J Community Support Oncol 14:141–147. https://doi.org/10.12788/jcso.0245
Ruhlmann CH, Christensen TB, Dohn LH et al (2016) Efficacy and safety of fosaprepitant for the prevention of nausea and emesis during 5 weeks of chemoradiotherapy for cervical cancer (the GAND-emesis study): a multinational, randomised, placebo-controlled, double-blind, phase 3 trial. Lancet Oncol 17:509–518. https://doi.org/10.1016/s1470-2045(15)00615-4
Ades S, Halyard M, Wilson K et al (2017) Effectiveness of aprepitant in addition to ondansetron in the prevention of nausea and vomiting caused by fractionated radiotherapy to the upper abdomen (AVERT). Support Care Cancer 25:1503–1510. https://doi.org/10.1007/s00520-016-3540-4
Yi J, Huang X, Gao L et al (2014) Intensity-modulated radiotherapy with simultaneous integrated boost for locoregionally advanced nasopharyngeal carcinoma. Radiat Oncol 9:56. https://doi.org/10.1186/1748-717x-9-56
Brouwer CL, Steenbakkers RJHM, Bourhis J et al (2015) CT-based delineation of organs at risk in the head and neck region: DAHANCA, EORTC, GORTEC, HKNPCSG, NCIC CTG, NCRI, NRG Oncology and TROG consensus guidelines. Radiother Oncol 117:83–90. https://doi.org/10.1016/j.radonc.2015.07.041
Einhorn LH, Rapoport B, Navari RM et al (2017) 2016 updated MASCC/ESMO consensus recommendations: prevention of nausea and vomiting following multiple-day chemotherapy, high-dose chemotherapy, and breakthrough nausea and vomiting. Support Care Cancer 25:303–308. https://doi.org/10.1007/s00520-016-3449-y
Englert S, Kieser M (2012) Adaptive designs for single-arm phase II trials in oncology. Pharm Stat 11:241–249. https://doi.org/10.1002/pst.541
Kawaguchi R, Tanase Y, Haruta S et al (2015) Addition of aprepitant to standard therapy for prevention of nausea and vomiting among patients with cervical cancer undergoing concurrent chemoradiotherapy. Int J Gynaecol Obstet 131:312–313. https://doi.org/10.1016/j.ijgo.2015.05.030
Strojan P, Vermorken JB, Beitler JJ et al (2016) Cumulative cisplatin dose in concurrent chemoradiotherapy for head and neck cancer: a systematic review. Head Neck 38(Suppl 1):E2151–E2158. https://doi.org/10.1002/hed.24026
Ang KK (2004) Concurrent radiation chemotherapy for locally advanced head and neck carcinoma: Are we addressing burning subjects? J Clin Oncol 22:4657–4659. https://doi.org/10.1200/jco.2004.07.962
Li X‑Y, Luo D‑H, Guo L et al (2022) Deintensified chemoradiotherapy for pretreatment Epstein-Barr virus DNA-selected low-risk locoregionally advanced nasopharyngeal carcinoma: a phase II randomized noninferiority trial. J Clin Oncol. https://doi.org/10.1200/jco.21.01467
Tang L‑Q, Chen D‑P, Guo L et al (2018) Concurrent chemoradiotherapy with nedaplatin versus cisplatin in stage II–IVB nasopharyngeal carcinoma: an open-label, non-inferiority, randomised phase 3 trial. Lancet Oncol 19:461–473. https://doi.org/10.1016/s1470-2045(18)30104-9
Hesketh PJ, Grunberg SM, Gralla RJ et al (2003) The oral neurokinin‑1 antagonist aprepitant for the prevention of chemotherapy-induced nausea and vomiting: a multinational, randomized, double-blind, placebo-controlled trial in patients receiving high-dose cisplatin—the aprepitant protocol 052 study group. J Clin Oncol 21:4112–4119. https://doi.org/10.1200/JCO.2003.01.095
Poli-Bigelli S, Rodrigues-Pereira J, Carides AD et al (2003) Addition of the neurokinin 1 receptor antagonist aprepitant to standard antiemetic therapy improves control of chemotherapy-induced nausea and vomiting. Results from a randomized, double-blind, placebo-controlled trial in Latin America. Cancer 97:3090–3098. https://doi.org/10.1002/cncr.11433
Bosnjak SM, Gralla RJ, Schwartzberg L (2017) Prevention of chemotherapy-induced nausea: the role of neurokinin‑1 (NK1) receptor antagonists. Support Care Cancer 25:1661–1671. https://doi.org/10.1007/s00520-017-3585-z
D’Souza H, Noronha V, Patil VM et al (2020) Aprepitant in weekly cisplatin with radiation in head and neck cancer: Is it required? J Clin Oncol 38:e24122–e24122
Szturz P, Wouters K, Kiyota N et al (2017) Weekly low-dose versus three-weekly high-dose cisplatin for concurrent chemoradiation in locoregionally advanced non-nasopharyngeal head and neck cancer: a systematic review and meta-analysis of aggregate data. Oncologist 22:1056–1066. https://doi.org/10.1634/theoncologist.2017-0015
Vardy J, Chiew KS, Galica J et al (2006) Side effects associated with the use of dexamethasone for prophylaxis of delayed emesis after moderately emetogenic chemotherapy. Br J Cancer 94:1011–1015. https://doi.org/10.1038/sj.bjc.6603048
Liaw CC, Wang CH, Chang HK et al (2005) Cisplatin-related hiccups: male predominance, induction by dexamethasone, and protection against nausea and vomiting. J Pain Symptom Manage 30:359–366. https://doi.org/10.1016/j.jpainsymman.2005.08.008
Go SI, Koo DH, Kim ST et al (2017) Antiemetic corticosteroid rotation from dexamethasone to methylprednisolone to prevent dexamethasone-induced hiccup in cancer patients treated with chemotherapy: a randomized, single-blind, crossover phase III trial. Oncologist 22:1354–1361. https://doi.org/10.1634/theoncologist.2017-0129
Acknowledgements
This work was supported by Beijing Hope Run Special Fund of Cancer Foundation of China, LC2017B17. Preliminary results were presented as an oral presentation at the 62nd Annual Meeting of the American Society of Radiation Oncology (ASTRO), Virtual Meeting, Oct 25–28, 2020, and were selected as one of the “Best of ASTRO” abstracts.
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of interest
Z. Wang, W. Liu, J. Zhang, X. Chen, J. Wang, K. Wang, Y. Qu, X. Huang, J. Luo, J. Xiao, G. Xu, L. Gao, J. Yi, and Y. Zhang declare that they have no competing interests.
Ethical standards
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of National Cancer Center/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College (Approval No.17-115/1371). Informed consent was obtained from all individual participants included in the study.
Additional information
Trial registration ID: NCT03572829.
Rights and permissions
About this article

Cite this article
Wang, Z., Liu, W., Zhang, J. et al. Antiemetic prophylaxis for chemoradiotherapy-induced nausea and vomiting in locally advanced head and neck squamous cell carcinoma: a prospective phase II trial. Strahlenther Onkol 198, 949–957 (2022). https://doi.org/10.1007/s00066-022-01958-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00066-022-01958-7