
Background and Purpose:
To analyze dose distribution in the hearing organ and to evaluate the dose effect on the hearing thresholds in patients treated with post-parotidectomy 3-dimensional conformal radiotherapy (3D-CRT).
Methods and Materials:
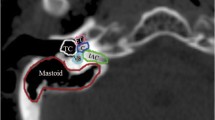
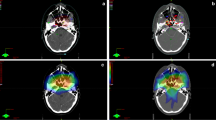
A total of 17 patients received post-parotidectomy 3D-CRT (median dose: 63 Gy). The audiometric evaluation comprised pure tone audiometry and tympanometry performed before radiotherapy (RT) and 3, 6, and 24 months after RT. The ear structures were delineated on planning computer tomography scans. Mean and maximum doses were calculated and dose–volume histograms were plotted.
Results:
Before RT, the median baseline audiometric thresholds were normal. At 3 months post-RT, 3 patients were diagnosed as having middle ear underpressure and/or effusion that resolved completely by 6 months. During 2-year follow-up, none of the ears showed perceptive hearing loss at speech frequencies. The mean doses at ipsilateral external auditory canal, mastoids cells, tympanic case, Eustachian tube, semicircular canals, and cochlea were 44.8 Gy, 39.0 Gy, 30.9 Gy, 33.0 Gy, 19.6 Gy, and 19.2 Gy, respectively. The doses to the contralateral ear were negligible, except for the Eustachian tube (up to 28.2 Gy).
Conclusion:
Post-parotidectomy 3D-CRT is associated with relatively low doses to the ear and the surrounding structures. Post-RT audiometry did not show any permanent (neither conductive nor perceptive) hearing impairment. Only in 3 patients were there signs of transient unilateral dysfunction of the Eustachian tube observed during the first few months after RT. Longer follow-up and larger patient series are warranted to confirm these preliminary findings.
Hintergrund und Ziel:
Dosisverteilungsanalyse im Hörorgan für Patienten mit 3-dimensionaler konformaler Radiotherapie (3D-CRT) nach Parotidektomie.
Patienten und Methoden:
17 Patienten erhielten eine 3D-CRT nach radikaler Parotidektomie (mittlere Dosis: 63 Gy). Die audiometrische Evaluierung umfasste Tonaudiometrie und Tympanometrie vor, 3, 6 und 24 Monate nach der Radiotherapie. Die Ohrstrukturen wurden im Planungscomputertomogramm konturiert. Die mittleren und maximalen Gesamtstrahlendosen wurden berechnet und die Dosis-Volumen-Histogramme ausgewertet.
Ergebnisse:
Vor Radiotherapie waren die medianen audiometrischen Ausgangsgrenzwerte normal. 3 Monate nach der RT zeigten sich bei 3 Patienten Unterdruck im Mittelohr und/oder Effusion, die nach 6 Monaten vollständig verschwanden. Während des 2-jährigen Follow-up zeigte keines der Ohren perzeptive Hörverluste bei Sprachfrequenzen. Die mittleren Dosen im äußeren ipsilateralen Gehörgang, in Mastoidzellen, im Trommelfell, in der Eustachischen Röhre, in Bogengängen und Cochlea waren 44,8 Gy, 39,0 Gy, 30,9 Gy, 33,0 Gy, 19,6 Gy und 19,2 Gy. Die Dosen im kontralateralen Ohr waren vernachlässigbar, abgesehen von der Eustachischen Röhre (bis zu 28,2 Gy).
Schlussfolgerung:
3D-CRT nach Parotidektomie ist mit relativ geringen Dosen im Hörorgan verbunden. Audiometrie nach der RT zeigte keine Hörschäden an. Längere Folgestudien und größere Patientenserien sind gerechtfertigt, um diese vorläufigen Ergebnisse zu bestätigen.
Similar content being viewed by others

References
Berger B, Belka C, Wienmann M et al. Reirradiation with alternating docetaxel-based chemotherapy for recurrent head and neck squamous cell carcinoma: update of a single-center prospective phase II protocol. Strahlenther Onkol 2010;186:255–261.
Bhandare N, Antonelli PJ, Morris CG et al. Ototoxicity after radiotherapy for head and neck tumors. Int J Radiat Oncol Biol Phys 2007;67:469–479.
Bhandare N, Jackson A, Eisbruch A et al. Radiation therapy and hearing loss. Int J Radiat Oncol BIol Phys 2010;76;S50–S57.
Bhide SA, Harrington KJ, Nutting CM. Otological toxicity after postoperative radiotherapy for parotid tumours. Clin Oncol 2006;19:77–82.
Cacciatore F, Napoli C, Abete P et al. Quality of life determinants and hearing function in an elderly population: Osservatorio Geriatrico Campano Study Group. Gerontol 1999;45:323–328.
Chen WC, Liao CT, Tsai HC et al. Radiation-induced hearing impairment in patients treated for malignant parotid tumor. Ann Otol Rhinol Laryngol 1999;108:1159–1164.
Cheng PW, Young YH, Lou PJ. Patolous eustachian tube in long-term survivors of nasopharyngeal carcinoma. Ann Otol Rhinol Laryngol 1999;108:201–204.
Committee on hearing and equilibrium. Committee on hearing and equilibrium guidelines for the evaluation of hearing preservation in acoustic neuroma (vestibular schwannoma). Otolaryngol 1995;113:179–180.
Fuss M, Debus J, Lohr F et al. Conventionally fractionated stereotactic radiotherapy (FSRT) for acoustic neuromas. Int J Radiat Oncol Biol Phys 2000;48:1381–1387.
Grau C, Overgaard J. Postiradiation sensorineural hearing loss: a common but ignored late radiation complication. Int J Radiat Oncol Biol Phys 1996;36:515–517.
Gunn GB, Endres EJ, Parker B et al. A phase I/II study of altered fractionated IMRT alone for intermediate T-stage oropharyngeal carcinoma. Strahlenther Onkol 2010;186:489–495.
Ho WK, Wei WI, Kwong DL et al. Long-term senorineural hearing deficit following radiotherapy in patients suffering from nasopharyngeal carcinoma: A prospective study. Head Neck 1999;21:547–553.
Hoistad DL, Ondrey FG, Mutlu C et al. Histopathology of human temporal bone after cis-platinum, radiation, or both. Otolaryngol Head Neck Surg 1998;118:825–832.
Honore HB, Bentzen SM, Møller K et al. Sensori-neural hearing loss after radiotherapy for nasopharyngeal carcinoma: individualized risk estimation. for nasopharyngeal carcinoma: individualized risk estimation. Radiother Oncol 2002;65:9–16.
ICRU. Report 62: Prescribing, recording and reporting photon beam therapy (supplement to ICRU report 50). Bethesda: International Commission on RadiationUnits and Measurements, 1999. Units and Measurements, 1999.
Jereczek-Fossa BA, Orecchia R. Radiotherapy-induced mandibular bone complications. Cancer Treat Rev 2002;28:65–74.
Jereczek-Fossa BA, Zarowski A, Milani F et al. Radiotherapy-induced ear toxicity. Cancer Treat Rev 2003;29:417–430.
Johannesen TB, Rasmussen K, Winther FO et al. Late radiation effects on hearing, vestibular function, and taste in brain tumor patients. Int J Radiat Oncol Biol Phys 2002;53:86–90.
Lin R, Hug EB, Schaefer RA et al. Conformal proton radiation therapy of the posterior fossa: a study comparing protons with three-dimensional planned photons in limiting dose to auditory structures. Int J Radiat Oncol Biol Phys 2000;48:1219–1226.
Nutting CM, Rowbottom HB, Cosgrove VP et al. Optimisation of radiotherapy for carcinoma of the parotid gland: a comparison of conventional, three-dimensionalconformal, and intensity-modulated techniques. Radiother Oncol 2001;60:163–172.
Ondrey FG, Greig JR, Herscher L. Radiation dose to otologic structures during head and neck cancer radiation therapy. Laryngoscope 2000;110:217–221.
Ogunrinde OK, Lunsford LD, Flickinger JC et al. Stereotactic radiosurgery for acoustic nerve tumors in patients with useful preoperative hearing: Results at 2-year follow-up examination. J Neurosurg 1994;80:1011–1017.
Pan CC, Eisbruch A, Lee JS et al. Prospective study of inner ear radiation dose and hearing loss in head-and-neck cancer patients. Int J Radiat Oncol Biol Phys 2005;61:1393–1402.
Platteaux N, Dirix P, Hermans R et al. Brachial plexopathy after chemoradiotherapy for head and neck squamous cell carcinoma. Strahlenther Onkol 2010;186:517–520.
Raaijmakers E, Engelen AM. Is sensorineural hearing loss a possible side effect of nasopharyngeal and parotid irradiation? A systematic review of the literature. Radiother Oncol 2002;65:1–7.
Rades D, Stoehr M, Mayners T et al. Evaluation of prognostic factors and two radiation techniques in patients treated with surgery followed by radio(chemo)therapy or definitive radio(chemo)therapy for locally advanced head-and-neck-cancer. Strahlenther Onkol 2008;184:198–205.
Sataloff RT, Rosen DC. Effects of cranial irradiation on hearing acuity: a review of the literature. Am J Otol 1994;15:772–780.
Sobin LH, Witteking Ch. TNM. Classification of malignant tumours, UICC-Internation Union Against Cancer Sixth Edition 2002. Wiley-Liss. John Wiley & Sons, 2002.
Sterzing F, Schubert K, Sroka-Perez G et al. Helical tomotherapy. Experiences of the first 150 patients in Heidelberg. Strahlenther Onkol 2008;184:8–14.
Tribius S, Kronemann S, Kilic Y et al. Radiochemotherapy including cisplatin alone versus cisplatin + 5-fluorouracil for locally advanced unresectable stage IV squamous cell carcinoma of the head and neck. Strahlenther Onkol 2009;185:675–681.
van der Putten L, de Bree R, Plukker JT et al. Permanent unilateral hearing loss after radiotherapy for parotid gland tumors. Head Neck 2006;28:902–909.
Wolf HA, Bosch J, Jung K et al. High-grade acute organ toxicity as positive prognostic factor in primary radio(chemo)therapy for locally advanced, inoperable head and neck cancer. Strahlenther Onkol 2010;186:262–268
Wolfram S. The Mathematica Book — Fourth Edition, Cambridge University Press, Cambridge, 2000.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Jereczek-Fossa, B.A., Rondi, E., Zarowski, A. et al. Prospective study on the dose distribution to the acoustic structures during postoperative 3D conformal radiotherapy for parotid tumors. Strahlenther Onkol 187, 350–356 (2011). https://doi.org/10.1007/s00066-011-2170-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00066-011-2170-5