
Abstract
Purpose:
To assess survival, local control and toxicity using fractionated stereotactic conformal radiotherapy (FSCRT) boost and temozolomide in high-grade gliomas (HGGs).
Patients and Methods:
Patients affected by HGG, with a CTV1(clinical target volume, representing tumor bed ± residual tumor + a margin of 5 mm) ≤ 8 cm were enrolled into this phase II study. Radiotherapy (RT, total dose 6,940 cGy) was administered using a combination of two different techniques: three-dimensional conformal radiotherapy (3D-CRT, to achieve a dose of 5,040 or 5,940 cGy) and FSCRT boost (19 or 10 Gy) tailored by CTV1diameter (≤ 6 cm and > 6 cm, respectively). Temozolomide (75 mg/m2) was administered during the first 2 or 4 weeks of RT. After the end of RT, temozolomide (150–200 mg/m2) was administered for at least six cycles. The sample size of 41 patients was assessed by the single proportion–powered analysis.
Results:
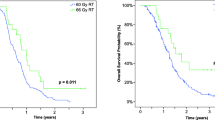
41 patients (36 with glioblastoma multiforme [GBM] and five with anaplastic astrocytoma [AA]) were enrolled; RTOG neurological toxicities G1–2 and G3 were 12% and 3%, respectively. Two cases of radionecrosis were observed. At a median follow-up of 44 months (range 6–56 months), global and GBM median overall survival (OS) were 30 and 28 months. The 2-year survival rate was significantly better compared to the standard treatment (63% vs. 26.5%; p < 0.00001). Median progression-free survival (PFS) was 11 months, in GBM patients 10 months.
Conclusion:
FSCRT boost plus temozolomide is well tolerated and seems to increase survival compared to the standard treatment in patients with HGG.
Zusammenfassung
Ziel:
Untersuchung von Uberleben, lokaler Tumorkontrolle und Toxizitat einer fraktionierten stereotaktischen konformalen Strahlentherapie (FSCRT) mit Boostbestrahlung in Kombination mit Temozolomid bei hochmalignen Gliomen (HMG).
Patienten und Methodik:
Patienten mit HMG und einem CTV1(klinisches Zielvolumen, d. h. Tumorbett ± Resttumor + einem Sicherheitsabstand von 5 mm) ≤ 8 cm wurden in diese Phase-II-Studie eingeschlossen. Die Strahlentherapie (Gesamtdosis 6 940 cGy) wurde als Kombination aus zwei unterschiedlichen Techniken appliziert: dreidimensionale konformale Strahlentherapie (3D-CRT, um eine Strahlendosis von 5 040 oder 5 940 cGy zu erreichen) und lokale Dosisaufsattigung mit FSCRT-Boost (19 oder 10 Gy), die auf den CTV1-Durchmesser (≤ 6 cm bzw. > 6 cm) zugeschnitten war. Temozolomid (75 mg/m2) wurde wahrend der ersten 2 oder 4 Wochen der Strahlentherapie verabreicht. Nach dem Ende der Strahlentherapie erhielten die Patienten Temozolomid (150–200 mg/m2) fur wenigstens sechs Zyklen. Die Fallzahl wurde mit Hilfe eines einfach-proportionalen Testverfahrens („single proportion-powered analysis“) bei 41 Patienten bestimmt.
Ergebnisse:
41 Patienten (36 mit Glioblastoma multiforme [GBM] und funf mit anaplastischem Astrozytom [AA]) wurden behandelt; Neurotoxizitat gemas RTOG-Skala G1–2 bzw. G3 wurde in 12% bzw. 3% der Patienten beobachtet. Zwei Falle von Radionekrose traten auf. Bei einer mittleren Beobachtungszeit von 44 Monaten (Range 6–56 Monate) lagen die mittlere Gesamt- und die GBM-spezifische Uberlebenszeit (OS) bei 30 und 28 Monaten. Die 2-Jahres-Uberlebensrate war signifikant besser im Vergleich zur Standardbehandlung (63% vs. 26,5%; p < 0.00001). Die mittlere progressionsfreie Uberlebenszeit (PFS) betrug 11 Monate, bei GBM-Patienten 10 Monate.
Schlussfolgerung:
FSCRT-Boostbestrahlung plus Temozolomid wird gut toleriert und scheint im Vergleich zur Standardbehandlung die Uberlebenszeit von Patienten mit HMG zu verbessern.
Similar content being viewed by others

References
Aydın H, Sillenberg I, von Lieven H, et al. Patterns of failure following CT-based 3-D irradiation for malignant glioma. Strahlenther Onkol 2001;177:424–31
Balducci M, D’Agostino GR, Manfrida S, et al. Radiotherapy and concomitant temozolomide during the first and last weeks in high grade gliomas: long-term analysis of a phase II study. J Neurooncol 2010;97:95–100
Baumert BG, Lutterbach J, Bernays R, et al. Fractionated stereotactic radiotherapy boost after post-operative radiotherapy in patients with high-grade gliomas. Radiother Oncol 2003;67:183–90
Cardinale R, Won M, Choucair A, et al. A phase II trial of accelerated radiotherapy using weekly stereotactic conformal boost for supratentorial glioblastoma multiforme: RTOG 0023. Int J Radiat Oncol Biol Phys 2006;65:1422–8
Chan JL, Lee SW, Fraass BA, et al. Survival and failure patterns of high-grade gliomas after three-dimensional conformal radiotherapy. J Clin Oncol 2002;20:1635–42
Cho KH, Hall WA, Lo SS, et al. Stereotactic radiosurgery versus fractionated stereotactic radiotherapy boost for patients with glioblastoma multiforme. Technol Cancer Res Treat 2004;3:41–9
Cox DR. Regression models and life tables. J R Stat Soc 1972;34:187–229
Cox JD, Stetz J, Pajak TF. Toxicity criteria of the Radiation Therapy Oncology Group (RTOG) and the European Organization for Research and Treatment of Cancer (EORTC). Int J Radiat Oncol Biol Phys 1995;31:1341–6
Curran WJ Jr, Scott CB, Horton J, et al. Recursive partitioning analysis of prognostic factors in three Radiation Therapy Oncology Group malignant glioma trials. J Natl Cancer Inst 1993;85:704–10
Emami B, Lyman J, Brown A, et al. Tolerance of normal tissue to therapeutic radiation. Int J Radiat Oncol Biol Phys 1991;21:109–22
Erlich SS, Davis RL. Spinal subarachnoid metastasis from primary intracranial glioblastoma multiforme. Cancer 1978;42:2854–64
Fokas E, Wacker U, Gross MW, et al. Hypofractionated stereotactic reirradiation of recurrent glioblastomas. A beneficial treatment option after high-dose radiotherapy? Strahlenther Onkol 2009;185:235–40
Glas M, Happold C, Rieger W, et al. Long-term survival of patients with glioblastoma treated with radiotherapy and lomustine plus temozolomide. J Clin Oncol 2009;27:1257–61
Henke G, Paulsen F, Steinbach JP, et al. Hypofractionated reirradiation for recurrent malignant glioma. Strahlenther Onkol 2009;185:113–9
Iliades G, Selviaridis P, Kalogera-Fountzila A, et al. The importance of tumor volume in the prognosis of patients with glioblastoma. Comparison of computerized volumetry and geometric models. Strahlenther Onkol 2009;185:743–50
Kaplan EL, Meier P. Nonparametric estimation from incomplete observations. J Am Stat Assoc 1958;53:457
Lai A, Filka E, McGibbon B, et al. Phase II pilot study of bevacizumab in combination with temozolomide and regional radiation therapy for up-front treatment of patients with newly diagnosed glioblastoma multiforme: interim analysis of safety and tolerability. Int J Radiat Oncol Biol Phys 2008;71:1372–80
Lamborn KR, Chang SM, Prados MD. Prognostic factors for survival of patients with glioblastoma: recursive partitioning analysis. Neuro Oncol 2004;6:227–35
Lee SW, Fraass BA, Marsh LH, et al. Patterns of failure following high-dose 3-D conformal radiotherapy for high-grade astrocytomas: a quantitative dosimetric study. Int J Radiat Oncol Biol Phys 1999;43:79–88
Macdonald DR, Cascino TL, Schold SC, et al. Response criteria for phase II studies of supratentorial malignant glioma. J Clin Oncol 1990;8:1277–80
Mangiola A, de Bonis P, Maira G, et al. Invasive tumor cells and prognosis in a selected population of patients with glioblastoma multiforme. Cancer 2008;113:841–6
Mantel N. Evaluation of survival data and two new rank order statistics arising in its consideration. Cancer Chemother Rep 1966;5:163–70
Marks JE, Baglan RJ, Prassad SC, et al. Cerebral radionecrosis: incidence and risk in relation to dose, time, fractionation and volume. Int J Radiat Oncol Biol Phys 1981;7:243–52
Mirinamoff RO, Gorlia T, Mason W, et al. Radiotherapy and temozomide for newly diagnosed glioblastoma: recursive partitioning analysis of the EORTC 26981/22981-NCIC CE3 phase III randomized trial. J Clin Oncol 2006;24:2563–9
Nakagawa K, Aoki Y, Fujimaki T, et al. High-dose conformal radiotherapy influenced the pattern of failure but did not improve survival in glioblastoma multiforme. Int J Radiat Oncol Biol Phys 1998;40:1141–9
Narayana A, Golfinos JG, Fischer I, et al. Feasibility of using bevacizumab with radiation therapy and temozolomide in newly diagnosed high-grade glioma. Int J Radiat Oncol Biol Phys 2008;72:383–9
Nieder C, Andratschke N, Wiedenmann N, et al. Radiotherapy for high-grade gliomas. Does altered fractionation improve the outcome? Strahlenther Onkol 2004;180:401–7
Nwokedi EC, DiBiase SJ, Jabbour S, et al. Gamma knife stereotactic radiosurgery for patients with glioblastoma multiforme. Neurosurgery 2002;50:41–6
Park I, Tamai G, Lee MC, et al. Patterns of recurrence analysis in newly diagnosed glioblastoma multiforme after three-dimensional conformal radiation therapy with respect to pre-radiation therapy magnetic resonance spectroscopic findings. Int J Radiat Oncol Biol Phys 2007;69:381–9
Regine WF, Patchell RA, Strottmann JM, et al. Preliminary report of a phase I study of combined fractionated stereotactic radiosurgery and conventional external beam radiation therapy for unfavourable gliomas. Int J Radiat Oncol Biol Phys 2000;48:421–6
Rickhey M, Koelbl O, Eilles C, Bogner L. A biologically adapted dose-escalation approach, demonstrated for 18F-FET-PET in brain tumors. Strahlenther Onkol 2008;184:536–42
Sarkaria JN, Mehta MP, Loeffler JS, et al. Radiosurgery in the initial management of malignant gliomas: survival comparison with the RTOG recursive partitioning analysis. Int J Radiat Oncol Biol Phys 1995;32:931–41
Shepherd SF, Laing RW, Cosgrove VP, et al. Hypofractionated stereotactic radiotherapy in the management of recurrent glioma. Int J Radiat Oncol Biol Phys 1997;37:393–8
Souhami L, Seiferheld W, Brachman D, et al. Randomized comparison of stereotactic radiosurgery followed by conventional radiotherapy with carmustine to conventional radiotherapy with carmustine for patients with glioblastoma multiforme: report of Radiation Therapy Oncology Group 93-05 protocol. Int J Radiat Oncol Biol Phys 2004;60:853–60
Stupp R, Hegi ME, Gilbert MR, Chakravarti A. Chemoradiotherapy in malignant glioma: standard of care and future directions. J Clin Oncol 2007; 25:4127–36
Stupp R, Mason WP, van den Bent MJ, et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med 2005;352:987–96
Walker MD, Strike T, Sheline GE. An analysis of dose-effect relationship in the radiotherapy of malignant gliomas. Int J Radiat Oncol Biol Phys 1979;5:1725–31
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Balducci, M., Apicella, G., Manfrida, S. et al. Single-Arm Phase II Study of Conformal Radiation Therapy and Temozolomide plus Fractionated Stereotactic Conformal Boost in High-Grade Gliomas. Strahlenther Onkol 186, 558–564 (2010). https://doi.org/10.1007/s00066-010-2101-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00066-010-2101-x