
Abstract
Objective
Provision of a natural scaffold, good quality cells, and growth factors in order to facilitate the replacement of the complete osteochondral unit with matching talar curvature for large medial primary and secondary osteochondral defects of the talus.
Indications
Symptomatic primary and secondary medial osteochondral defects of the talus not responding to conservative treatment; anterior–posterior or medial–lateral diameter >10 mm on computed tomography (CT); closed distal tibial physis in young patients.
Contraindications
Tibiotalar osteoarthritis grade III; multiple osteochondral defects on the medial, central, and lateral talar dome; malignancy; active infectious ankle joint pathology.
Surgical technique
A medial distal tibial osteotomy is performed, after which the osteochondral defect is excised in toto from the talar dome. The recipient site is microdrilled in order to disrupt subchondral bone vessels. Then, the autograft is harvested from the ipsilateral iliac crest with an oscillating saw, after which the graft is adjusted to an exact fitting shape to match the extracted osteochondral defect and the talar morphology as well as curvature. The graft is implanted with a press-fit technique after which the osteotomy is reduced with two 3.5 mm lag screws and the incision layers are closed. In cases of a large osteotomy, an additional third tubular buttress plate is added, or a third screw at the apex of the osteotomy.
Postoperative management
Non-weight bearing cast for 6 weeks, followed by another 6 weeks with a walking boot. After 12 weeks, a CT scan is performed to assess consolidation of the osteotomy and the inserted autograft. The patient is referred to a physiotherapist.
Results
Ten cases underwent the TOPIC procedure, and at 1 year follow-up all clinical scores improved. Radiological outcomes showed consolidation of all osteotomies and all inserted grafts showed consolidation. Complications included one spina iliaca anterior avulsion and one hypaesthesia of the saphenous nerve; in two patients the fixation screws of the medial malleolar osteotomy were removed.
Zusammenfassung
Operationsziel
Wiederherstellung des natürlichen Knochengerüsts mit gesunden Zellen und Wachstumsfaktoren zur Rekonstruktion von großen primären und sekundären Knochendefekten an der medialen Talusrolle, mit Einsatz einer kompletten osteochondralen Einheit mit passendem Radius entsprechend der Talusrolle.
Indikationen
Symptomatische primäre und sekundäre mediale osteochondrale Defekte am Talus nach fehlgeschlagener Physiotherapie; anteroposteriorer und/oder mediolateraler Durchmesser >10 mm in der Computertomographie (CT); bei jüngeren Patienten: geschlossene Wachstumsfuge der distalen Tibia.
Kontraindikationen
Generalisierte Osteoarthrose im gesamten Sprunggelenk; multiple Osteochondraldefekte; aktive Infektion; Malignität.
Operationstechnik
Zunächst wird eine mediale Osteotomie der distalen Tibia durchgeführt, anschließend der Osteochondrale Defekt vollständig aus dem Talus entfernt. Der Defekt wird angebohrt, um die subchondralen Blutgefäße zu öffnen. Das Transplantat wird am ipsilateralen Beckenkamm mit der oszillierenden Säge entnommen und in den Defekt unter Beachtung der korrekten Wiederherstellung von Form und Radius der Talusrolle eingepasst. Dann wird das Transplantat mittels Press-Fit-Technik fixiert. Anschließend erfolgen die Reposition der Tibiaosteotomie und die Fixation mit zwei 3,5-mm-Zugschrauben sowie der Wundverschluss.
Weiterbehandlung
Unbelastete Mobilisation im Unterschenkelgips für 6 Wochen, danach Vollbelastung in einer Unterschenkelorthese (Walker) für weitere 6 Wochen. Nach 12 Wochen Kontroll-CT zur Analyse der Knochenheilung sowohl der medialen Tibiaosteotomie als auch der Integration des Transplantates in den Talus. Danach beginnen mit Physiotherapie.
Ergebnisse
In einer prospektiven Studie wurden 10 konsekutive Patienten mit der TOPIC-Technik behandelt. Nach einem Nachuntersuchungszeitraum von 12 Monaten verbesserten sich alle klinischen Werte der Patienten. Als Komplikationen sind bisher eine Avulsionsfraktur der Spina iliaca anterior und eine Hypästhesie des N. Saphenus aufgetreten. Bei 2 Patienten traten leichte Druckschmerzen über dem medialen Malleolus auf, die nach Entfernen der Zugschrauben wieder verschwanden.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introductory remarks
Osteochondral defects of the talus are defined as damage to the talar articular cartilage and its subchondral bone. The origin of this injury may be due to ankle fractures and ankle sprains, an avascular episode, and possibly a genetic predisposition [1, 15, 25, 50]. The injuries have a severe impact on the quality of life of active patients, due to deep ankle pain during weight-bearing and sporting activities [4, 5, 22].
Primary management of these defects is conservative; surgery is considered in cases of persistent symptoms [52]. For small primary defects, common first-line surgical management options consist of (arthroscopic) bone marrow stimulation and retrograde drilling [11,12,13, 30, 43]. For fixable defects, arthroscopic and open internal fixation procedures are amenable options and have proven to be effective for pediatric and adult patient populations [28, 29, 31, 45, 46]. In case of large defects or in case of failure of first-line surgical treatment, more extensive and invasive surgery can be considered a necessary step in the management process [30]. The more common treatment strategies currently include osteochondral allograft procedures, osteochondral autograft transfer system (OATS) procedures, and classic and matrix-associated chondrocyte implantation (ACI, MACI) [20, 21, 32, 39, 55, 56]. Even though the OATS procedure is regarded as an effective surgical management option with a 90% success rate reported in the literature, donor-site morbidity has been reported to occur relatively frequently with incidence rates ranging from 11 to 35% when the graft was harvested from the ipsilateral femoral condyle [13, 16, 19, 23, 24, 26, 44, 57]. As an alternative to an OATS procedure harvesting the graft from the knee, an autologous osteoperiosteal cylinder graft can be harvested from the iliac crest. This technique has been described by Hu et al. [26] and Chen et al. [10]. This surgical treatment yielded highly promising results with good clinical follow-up scores and radiological outcomes. However, both author groups utilized cylindrical grafts, thereby compromising optimal individualized treatment for large talar osteochondral defects as it is known that that the size of the cylinder autograft is static and determined preoperatively.
In order to overcome the aforementioned disadvantages, we developed a new surgical technique for the treatment of large talar osteochondral defects or secondary lesions: the Talar OsteoPeriostic grafting from the Iliac Crest (TOPIC) procedure. This technique utilizes the ipsilateral iliac crest with its overlying periosteal layer as a harvesting location for the autograft. The use of the periosteum has been shown to have potential concerning articular cartilage-like tissue regeneration [35, 40]. The chondrogenic potential of this technique arises because the cambium layer of periosteum contains chondrocyte precursor cells [27, 37]. A bone-periosteal transplant for bone–cartilage repair meets the three requirements for tissue engineering: a source of cells, a scaffold, and local growth factors [2, 18, 34, 47, 54]. In addition, the curvature of the iliac crest is highly similar to the curvature of the talar bone, and the harvested graft can be exactly fitted to the excised defect from the talus [38]. The goal of the present surgical technique description is to describe the surgical technique of the newly developed TOPIC procedure and evaluate potential pearls and pitfalls.
Surgical principle and objective
A large primary or secondary osteochondral defect to the talus is a challenging problem in the orthopedic clinic. Multiple techniques exist to treat these defects, ranging from a cartilage implantation technique to an OATS procedure as well as an allograft procedure. These techniques have their individual advantages and disadvantages—such as donor-site morbidity, poor quality subchondral bone repair and low clinical efficacy. The current paper describes a new surgical technique for the treatment of large primary and secondary medial talar osteochondral defects. The technique comprises a medial distal tibial osteotomy and a talar autograft transplantation from the ipsilateral iliac crest. The technique has the main advantage of providing a natural scaffold, good quality cells, and growth factors, facilitating the replacement of the complete osteochondral unit—a triad considered important in the treatment of these defects.
Disadvantages
-
Access to talar dome through an osteotomy
-
Potential complaints of discomfort of the inserted screws and/or plate
-
Complications specifically for the harvest site, the iliac crest, and hyp(er)aesthesia of the skin [14]
Indications
-
General: painful osteochondral defect with a clear episode of deep ankle pain not responding to conservative treatment
-
Anterior–posterior or medial–lateral diameter should exceed 10 mm on computed tomography (CT)
-
The depth of the defect is no limitation for this procedure
-
Both primary and secondary surgical lesions are treated with a TOPIC
-
Closed distal tibial physis in young patients
-
If concomitant instability is present, a stabilizing procedure will be considered
-
In case of malalignment, a corrective osteotomy will be considered.
Contraindications
-
Tibiotalar osteoarthritis grade III
-
Multiple osteochondral defects on the medial, central, and lateral talar dome
-
Active infectious ankle joint pathology
-
Malignancy
Patient information
-
Usual surgical risks include infection, hematoma, thromboembolic event, wound healing problems
-
Transient or permanent nerve damage leading to hypaesthesia of the saphenous nerve
-
Late or early screw and or plate discomfort requiring removal after consolidation
-
Nonweight bearing cast for 6 weeks, followed by a walking boot for another 6 weeks
Preoperative work up
The Department of Orthopedic Surgery of the Amsterdam UMC, Location AMC has been officially recognized as an expert center for the treatment of osteochondral defects of the ankle and foot. All patients are screened with a careful patient history and physical examination of both lower legs. During the physical examination there is special attention for recognizable pain on palpation over the site of the talar osteochondral defect with the foot in plantar flexion to be sure that the patients’ deep ankle pain indeed arises from the osteochondral defect and not from any other pathology. Special emphasis is also put on the range of motion of the ankle joint, especially plantar flexion. This is done in order to determine whether an osteotomy will be necessary or whether the total defect can be reached without an osteotomy.
For confirmation of the diagnosis and as a preoperative sizing and planning tool, an additional CT scan is made. All talar osteochondral lesions are scanned for defect size, location, shape, and morphology. In addition, the lesion’s preoperative shape is classified according to the modified Berndt and Harty’s staging system with added stage V by Scranton and McDermott [7, 51].
Instruments and implants
-
Hohman retractors
-
Oscillating saw and/or chisel with thin blades
-
Beaver knife
-
2.0 mm Kirschner wires
-
2.0 mm drill
-
Coagulation knife
-
Hemostatic gelatin sponge (Spongostan®)
-
Impactor
-
3.5 mm cortical screws or a headless alternative
-
Standard orthopedic set
-
Chisel set
-
Large Weber clamps
Anesthesia and positioning
-
General or spinal anesthesia
-
Supine position with a tourniquet applied around the thigh
-
Antibiotic prophylaxis (cefazolin 2 g intravenous injection) is administered to each patient
Surgical technique
(Figs. 1, 2, 3, 4, 5, 6 and 7)

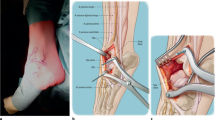
Medial distal tibial osteotomy. After prepping and draping, a slightly curved incision of approximately 7 cm is made over the medial malleolus (a), the large saphenous vein is identified and protected. An anteromedial arthrotomy is performed with a partial resection of the anteromedial joint capsule. Posterior from the medial malleolus, the retinaculum of the posterior tibial tendon is opened and the tendon is retracted to allow a subtle posteromedial capsular resection. Anterior and posterior Hohman retractors are placed in order to protect the neurovascular structures and the tendons. Then, an osteotomy is first prepared by predrilling the lag screw holes (b). Thereafter, the osteotomy is performed with an oscillating saw (c). In order to prevent thermal damage to the cartilage, the last 3 mm of the osteochondral zone of the distal tibial plafond is finished with a chisel (d). The extent of the osteotomy is decided based on the exact localization of the defect, as well as the sagittal and the coronal diameter of the defect. After finishing the osteotomy, the osteotomized distal tibia part is dislocated in both medial and plantar direction and this position is secured with the use of 1 (or 2) 2.0 mm Kirschner wire(s). This facilitates full exposure of the medial to central talar dome (e)

Excision of the diseased osteochondral defect. After the identification and exposure of the defect, a rectangular incision of the cartilage is made to preserve as much healthy cartilage as possible and to prevent the cartilage from rupturing in the next steps of the procedure (a). All cystic and necrotic bone is removed in total with the use of either an oscillating saw or a chisel with thin blades or both. The end result should be a total removal of the premeasured talar diseased osteochondral defect, deep enough so that healthy bone can be observed (b)

Drilling of the recipient’s subchondral bone base. As the defect has been excised beyond the subchondral bone plate, the base of the autograft recipient can be freely (micro)drilled for bone marrow stimulation using a 2.0 mm drill (a). This step of the procedure disrupts intraosseous vessels so that blood and bone marrow cells are introduced into the yet empty defect. b End result after drilling of the subchondral bone

Measuring and harvesting the donor autograft from the iliac crest. After having drilled the subchondral bone of the talus, the graft harvest is started. The first step is to exactly measure the size of the excised block, so that a correct approximation of the donor autograft can be performed—the graft should be 1 mm larger in all directions (anteroposterior and mediolateral diameter as well as depth). Approach the iliac crest through a horizontal incision of approximately 3.5 cm. Take care not to use the coagulation knife in order to keep the periosteum nicely intact and attached. Expose part of the iliac crest by means of two retractors (a). Then, a monocortical, bicortical, or tricortical osteoperiosteal autograft from the ipsilateral iliac crest is harvested with an oscillating saw and chisel (b). The combination of the size of the graft needed and the width of the crest dictates the choice for monocortical, bicortical, or a tricortical graft. A hemostatic gelatin sponge (Spongostan®) can be left in the iliac crest after harvesting the autograft

Adjusting the fitting shape of the autograft. The graft can be further fine-tuned to optimally fit curvature, size, and depth of the talar defect. Take care that graft is not too proud: 1–2 mm under the talar cartilage level at all sides seems best in order to prevent over-stuffing. The graft should be placed press-fit, which means 1 mm should be added on all dimensions of the excised defect, as mentioned in Fig. 4. Take time to perform this correctly as it will facilitate the step of executing a press-fit insertion technique. Comparing the graft to the excised talar defect may ameliorate the similarity of the autograft

Implanting the graft through a press-fit technique. Once the optimal fitting shape has been reached, the autograft is transported and placed into the host site (a). By means of an impactor the inserted autograft can be fitted exactly 1–2 mm underneath the level of the talar cartilage. The curvature of the iliac crest accurately matches the talar curvature (b). As this is a press-fit technique, no additional screws are necessary in order to fixate the autograft. In case of graft instability, the option of using one or two screws to stabilize the graft always remains

Closure of the distal tibial osteotomy and incision layers. The distal tibial osteotomy is closed and fixated by means of two 3.5 mm lag screws in case of a standard small medial malleolar osteotomy. We aim for two divergent bicortical screws (a). In case of a larger distal osteotomy we opt for two bicortical medial screws perpendicular to the osteotomy and an antiglide plate to prevent rotation and proximal translation of the osteotomy (b–d). Sometimes a third screw at the apex of the osteotomy is also a suitable option. Rinsing and closure in layers follows
Special surgical considerations
-
A preoperative CT scan is used to measure the bony dimensions of the osteochondral defect (anteroposterior diameter, mediolateral diameter and depth)
-
The last part of the distal tibial osteotomy is done with a chisel to prevent thermal damage to the osteochondral unit
-
Both the distal tibial osteotomy and iliac crest autograft transplantation can be customized for every patient
-
In case a larger distal tibial osteotomy is indicated, an extra antiglide plate can be used to prevent rotation and proximal translation
-
Press-fit autograft transplantation allows for quick rehabilitation without need for intra-articular screw removal
-
Theoretically, an optimal graft to replace an osteochondral unit has the following characteristics: natural scaffold, good quality cells, and growth factors [36, 41, 42, 48, 53]
Postoperative management
Directly after surgery a lower leg splint is provided for the first 24 h. Surgery is performed as a 1-day admission as this allows for adequate pain management and application of a fresh circular nonweight bearing lower leg cast applied for 2 weeks. After 2 weeks, the stitches are removed and the patient is allowed an hour of dorsoplantar ankle flexion motion in order to prevent stiffness and possibly enhance the stimulation of progenitor cells from the periosteum to produce an optimal chondral layer following stimulation through ankle joint motion [8, 9, 33].
The non-weight bearing period is 6 weeks with regular cast changes in order to allow an hour of ankle joint motion. At the 6‑week follow-up, a walking boot is applied for another 6 weeks. At the 12-week follow-up, a computed tomography (CT) scan provides information on consolidation of the distal tibial osteotomy as well as the autograft. At this visit we also do a clinical assessment of the patient and provide an individualized guideline for the next 3 months of rehabilitation. The patient is referred to a physiotherapist to guide and stimulate clinical progress and aid in the rehabilitation process. Additional follow-ups are performed at 6 months and 1 year postoperatively in order to closely assess progress of the patient, also concerning return to work, sports, and performance.
Errors, hazards, complications
At every follow-up, patients are checked for potential complications, such as crest pain, hyp(er)aesthesia in the crest and ankle joint region, infections, ankle joint synovitis, and postoperative pain. A radiograph is obtained 6 weeks postoperatively to assess consolidation of the osteotomy. A CT scan is made at 3 and 12 months after surgery to assess consolidation, ingrowth, and talar remodeling of the transplant. Potential pitfalls include the following:
-
Cartilage damage to ankle joint if not enough attention is paid to the distal tibial osteotomy
-
Neurovascular or posterior tibial tendon damage if Hohman retractors are not placed properly
-
Avulsion or fracture of the iliac crest when harvesting the graft too close to the anterior superior iliac spine
-
Proudness of the autograft might give a kissing lesion or chondral wear to distal anteromedial corner of the ankle joint
-
Graft failure
-
Non- or malunion of the osteotomy
-
Ankle joint stiffness
-
Persistent ankle pain because of progressive osteoarthritis (OA)
-
Impingement of the medial gutter if the graft has slight overhang or in case of presence of an osteophyte or multiple osteophytes
Results
The present study was approved by the local Medical Ethics Committee at the University of Amsterdam and performed in accordance with the current ethical standards (Declaration of Helsinki, reference number MEC 14/237 #14.17.0288). All patients undergoing a TOPIC procedure were assessed preoperatively and at 1 year postoperatively. Ten patients underwent the TOPIC procedure. Mean age was 36.1 years (standard deviation [SD] 17.9). The mean follow-up for the patients was 12 months (SD 1.0). Pre- and postoperative assessment included the Foot and Ankle Outcome Score (FAOS) subcales, the American Orthopaedic Foot and Ankle Society (AOFAS), Short-Form 36 (SF-36) Mental Component Scale (MCS) and Physical Component Scale (PCS), and the Numeric Rating Scales (NRS) of pain at rest and during walking and stair-climbing. Dual energy CT scans were taken preoperatively and at the 1 year follow-up. All patients were available for follow-up. The AOFAS significantly improved from 50 to 83 (p = 0.02). The NRS during rest improved from 2.4 to 1.0 (p = 0.072), during walking from 4.6 to 2.3 (p = 0.009), during stairclimbing from 4.3 to 1.8 (p = 0.011), and during running from 7.1 to 2.6 (p = 0.0011). The SF-36 PCS improved from 36 to 48 (p = 0.001) and the MCS from 47 to 56 (p = 0.132). All Foot and Ankle Outcome Score (FAOS) subscales improved significantly, except for the symptoms subscale. On the postoperative CT scans, all osteotomies and grafts showed consolidation (Fig. 8). Complications included one spina iliaca anterior avulsion and one temporary loss of sensitivity of the saphenous nerve; in two patients the medial malleolar screws were removed.

Preoperative and postoperative (1 year follow-up) computed tomography (CT) scans of the same patient. a Coronal preoperative CT scan. b Sagittal preoperative CT scan. c Coronal postoperative CT scan. d Sagittal postoperative CT scan
We present a novel press-fit autograft transfer technique for large talar osteochondral defects. Talar OsteoPeriostic grafting from the Iliac Crest (TOPIC) proved to be a reproducible and safe technique, with good short-term functional results and early radiographic consolidation of the graft on CT scan. We consider an improvement of on average of 30 points on the AOFAS scale and 2.3 (during activity) and 4.5 points (during running) on the NRS very promising. This, as a mean improvement of −2.0 on the NRS scale of 0 to 10 is significantly associated with the concept of a “much better improvement” [49].
Further advantages of the technique are its relative ease to perform, limited operation time, and the costs being relatively low in comparison to other extensive techniques such as for example an allograft implantation technique or chondrogenesis-inducing techniques. In addition, the iliac crest as a harvesting site not only matches the talar surface geometry, but it also has a chondrogenic potential to regenerate articular cartilage utilizing periosteum [27, 40]. If a TOPIC does fail, various salvage procedures are available: a redo, an ankle fusion or a total ankle prosthesis.
Disadvantages are the use of an autograft of the ipsilateral iliac crest that has potential complications such as persistent pain, neuralgia, or contour loss of the crest; however, with the technique used for harvesting the graft, this is minimized [3, 14]. Another disadvantage might be the use of a fairly large medial distal tibial osteotomy that has to extend into the tibial plafond in order to be able to excise the entire defect. All medial malleolar osteotomies showed complete union at 3 months postoperatively. Another complication of the present technique may be the complaints of the medial malleolar screws that were inserted [6, 17]. We encountered this in 3 patients, and hardware removal was necessary in 2 patients. A further disadvantage of the TOPIC technique might be the requirement of a high level of surgical skill for exact graft shaping. It needs to be 0.5 mm oversized in the sagittal plane while the width and depth in the coronal and axial plane should exactly fit the depth of the created defect in order to allow the graft to be placed 1–2 mm subchondral after impaction.
In a recent review, we described that there are several options that appear to be safe and provide good results in prospective case series, with up to 90% success of OATS techniques for larger talar osteochondral defects after failed prior surgical treatment [30]. In these OATS results, there were several harvesting sites described for the plugs. The iliac crest as a graft site has been previously described with good results; however, all techniques have the potential disadvantage of a nonfully anatomical fit and the possibility of new cyst formation in medium and long-term follow-up along the plugs used [26].
References
Alexander AH, Lichtman DM (1980) Surgical treatment of transchondral talar-dome fractures (osteochondritis dissecans). Long-term follow-up. J Bone Joint Surg Am 62:646–652
Armiento AR, Stoddart MJ, Alini M, Eglin D (2018) Biomaterials for articular cartilage tissue engineering: learning from biology. Acta Biomater 65:1–20
Arrington ED, Smith WJ, Chambers HG, Bucknell AL, Davino NA (1996) Complications of iliac crest bone graft harvesting. Clin Orthop Relat Res 329:300–309
Aspenberg P, Van der Vis H (1998) Migration, particles, and fluid pressure. A discussion of causes of prosthetic loosening. Clin Orthop Relat Res 352:75–80
Astrand J, Skripitz R, Skoglund B, Aspenberg P (2003) A rat model for testing pharmacologic treatments of pressure-related bone loss. Clin Orthop Relat Res 409:296–305
Baltzer AW, Arnold JP (2005) Bone-cartilage transplantation from the ipsilateral knee for chondral lesions of the talus. Arthroscopy 21:159–166
Berndt AL, Harty M (1959) Transchondral fractures (osteochondritis dissecans) of the talus. J Bone Joint Surg Am 41:988–1020
Campbell TM, Reilly K, Laneuville O, Uhthoff H, Trudel G (2018) Bone replaces articular cartilage in the rat knee joint after prolonged immobilization. Bone 106:42–51
Carter DR, Beaupre GS, Giori NJ, Helms JA (1998) Mechanobiology of skeletal regeneration. Clin Orthop Relat Res 355:S41–S55
Chen W, Tang K, Yuan C, Zhou Y, Tao X (2015) Intermediate results of large cystic medial osteochondral lesions of the talus treated with osteoperiosteal cylinder autografts from the medial tibia. Arthroscopy 31:1557–1564
Choi GW, Choi WJ, Youn HK, Park YJ, Lee JW (2013) Osteochondral lesions of the talus: are there any differences between osteochondral and chondral types? Am J Sports Med 41:504–510
Chuckpaiwong B, Berkson EM, Theodore GH (2008) Microfracture for osteochondral lesions of the ankle: outcome analysis and outcome predictors of 105 cases. Arthroscopy 24:106–112
Dahmen J, Lambers KT, Reilingh ML, van Bergen CJ, Stufkens SA, Kerkhoffs GM (2017) No superior treatment for primary osteochondral defects of the talus. Knee Surg Sports Traumatol Arthrosc 26:2142–2157
Dimitriou R, Mataliotakis GI, Angoules AG, Kanakaris NK, Giannoudis PV (2011) Complications following autologous bone graft harvesting from the iliac crest and using the RIA: a systematic review. Injury 42(Suppl 2):S3–S15
Draper SD, Fallat LM (2000) Autogenous bone grafting for the treatment of talar dome lesions. J Foot Ankle Surg 39:15–23
Ferreira C, Vuurberg G, Oliveira JM, Espregueira-Mendes J, Pereira H, Reis RL, Ripoll PL (2016) Good clinical outcome after osteochondral autologous transplantation surgery for osteochondral lesions of the talus but at the cost of a high rate of complications: a systematic review. J ISAKOS 2016:184–191
Gaulrapp H, Hagena FW, Wasmer G (1996) Postoperative evaluation of osteochondrosis dissecans of the talus with special reference to medial malleolar osteotomy. Z Orthop Ihre Grenzgeb 134:346–353
Gervaso F, Sannino A, Peretti GM (2013) The biomaterialist’s task: scaffold biomaterials and fabrication technologies. Joints 1:130–137
Giannini S, Vannini F (2004) Operative treatment of osteochondral lesions of the talar dome: current concepts review. Foot Ankle Int 25:168–175
Giannini S, Buda R, Vannini F, Di Caprio F, Grigolo B (2008) Arthroscopic autologous chondrocyte implantation in osteochondral lesions of the talus: surgical technique and results. Am J Sports Med 36:873–880
Giza E, Sullivan M, Ocel D, Lundeen G, Mitchell ME, Veris L, Walton J (2010) Matrix-induced autologous chondrocyte implantation of talus articular defects. Foot Ankle Int 31:747–753
Goddard NJ, Gosling PT (1988) Intra-articular fluid pressure and pain in osteoarthritis of the hip. J Bone Joint Surg Br 70:52–55
Haleem AM, Ross KA, Smyth NA, Duke GL, Deyer TW, Do HT, Kennedy JG (2014) Double-plug autologous osteochondral transplantation shows equal functional outcomes compared with single-plug procedures in lesions of the Talar dome: a minimum 5‑year clinical follow-up. Am J Sports Med 42:1888–1895
Hannon CP, Baksh N, Newman H, Murawski CD, Smyth NA, Kennedy JG (2013) A systematic review on the reporting of outcome data in studies on autologous osteochondral transplantation for the treatment of osteochondral lesions of the talus. Foot Ankle Spec 6:226–231
Hintermann B, Regazzoni P, Lampert C, Stutz G, Gachter A (2000) Arthroscopic findings in acute fractures of the ankle. J Bone Joint Surg 82:345–351
Hu Y, Guo Q, Jiao C, Mei Y, Jiang D, Wang J, Zheng Z (2013) Treatment of large cystic medial osteochondral lesions of the talus with autologous osteoperiosteal cylinder grafts. Arthroscopy 29:1372–1379
Ito Y, Fitzsimmons JS, Sanyal A, Mello MA, Mukherjee N, O’Driscoll SW (2001) Localization of chondrocyte precursors in periosteum. Osteoarthritis Cartilage 9:215–223
Kerkhoffs G, Karlsson J (2019) Osteochondral lesions of the talus. Knee Surg Sports Traumatol Arthrosc 27:2719–2720
Kerkhoffs GM, Reilingh ML, Gerards RM, de Leeuw PA (2016) Lift, drill, fill and fix (LDFF): a new arthroscopic treatment for talar osteochondral defects. Knee Surg Sports Traumatol Arthrosc 24:1265–1271
Lambers KT, Dahmen J, Reilingh ML, van Bergen CJ, Stufkens SA, Kerkhoffs GM (2017) No superior surgical treatment for secondary osteochondral defects of the talus. Knee Surg Sports Traumatol Arthrosc. https://doi.org/10.1007/s00167-00017-04616-00165
Lambers KTA, Dahmen J, Reilingh ML, van Bergen CJA, Stufkens SAS, Kerkhoffs GMMJ (2019) Arthroscopic lift, drill, fill and fix (LDFF) is an effective treatment option for primary talar osteochondral defects. Knee Surg Sports Traumatol Arthrosc. https://doi.org/10.1007/s00167-019-05687-w
Lee KT, Kim JS, Young KW, Lee YK, Park YU, Kim YH, Cho HK (2013) The use of fibrin matrix-mixed gel-type autologous chondrocyte implantation in the treatment for osteochondral lesions of the talus. Knee Surg Sports Traumatol Arthrosc 21:1251–1260
Leong DJ, Hardin JA, Cobelli NJ, Sun HB (2011) Mechanotransduction and cartilage integrity. Ann N Y Acad Sci 1240:32–37
Maia FR, Carvalho MR, Oliveira JM, Reis RL (2018) Tissue engineering strategies for osteochondral repair. Adv Exp Med Biol 1059:353–371
Matsushima S, Isogai N, Jacquet R, Lowder E, Tokui T, Landis WJ (2011) The nature and role of periosteum in bone and cartilage regeneration. Cells Tissues Organs 194:320–325
McGoldrick NP, Murphy EP, Kearns SR (2018) Osteochondral lesions of the ankle: the current evidence supporting scaffold-based techniques and biological adjuncts. Foot Ankle Surg 24:86–91
Mendes LF, Katagiri H, Tam WL, Chai YC, Geris L, Roberts SJ, Luyten FP (2018) Advancing osteochondral tissue engineering: bone morphogenetic protein, transforming growth factor, and fibroblast growth factor signaling drive ordered differentiation of periosteal cells resulting in stable cartilage and bone formation in vivo. Stem Cell Res Ther 9:42
Nagerl H, Hansen C, Kubein-Meesenburg D, Fanghanel J, Dathe H, Dumont C, Wachowski MM (2016) The upper ankle joint: Curvature morphology of the articulating surfaces and physiological function. Acta Bioeng Biomech 18:83–90
Nehrer S, Domayer SE, Hirschfeld C, Stelzeneder D, Trattnig S, Dorotka R (2011) Matrix-associated and autologous chondrocyte transplantation in the ankle: clinical and MRI follow-up after 2 to 11 years. Cartilage 2:81–91
O’Driscoll SW (1999) Articular cartilage regeneration using periosteum. Clin Orthop Relat Res 367:S186–S203
Pereira H, Vuurberg G, Spennacchio P, Batista J, D’Hooghe P, Hunt K, Van Dijk N (2018) Surgical treatment paradigms of ankle lateral instability, osteochondral defects and impingement. Adv Exp Med Biol 1059:85–108
Pintus E, Baldassarri M, Perazzo L, Natali S, Ghinelli D, Buda R (2018) Stem cells in osteochondral tissue engineering. Adv Exp Med Biol 1058:359–372
Ramponi L, Yasui Y, Murawski CD, Ferkel RD, DiGiovanni CW, Kerkhoffs GM, Calder JD, Takao M, Vannini F, Choi WJ, Lee JW, Stone J, Kennedy JG (2016) Lesion size is a predictor of clinical outcomes after bone marrow stimulation for osteochondral lesions of the talus: a systematic review. Am J Sports Med 45:1698–1705
Reddy S, Pedowitz DI, Parekh SG, Sennett BJ, Okereke E (2007) The morbidity associated with osteochondral harvest from asymptomatic knees for the treatment of osteochondral lesions of the talus. Am J Sports Med 35:80–85
Reilingh ML, Kerkhoffs GM, Telkamp CJ, Struijs PA, van Dijk CN (2014) Treatment of osteochondral defects of the talus in children. Knee Surg Sports Traumatol Arthrosc 22:2243–2249
Reilingh ML, Lambers KTA, Dahmen J, Opdam KTM, Kerkhoffs G (2018) The subchondral bone healing after fixation of an osteochondral talar defect is superior in comparison with microfracture. Knee Surg Sports Traumatol Arthrosc 26:2177–2182
Roseti L, Parisi V, Petretta M, Cavallo C, Desando G, Bartolotti I, Grigolo B (2017) Scaffolds for bone tissue engineering: state of the art and new perspectives. Mater Sci Eng C Mater Biol Appl 78:1246–1262
Rothrauff BB, Murawski CD, Angthong C, Becher C, Nehrer S, Niemeyer P, Sullivan M, Valderrabano V, Walther M, Ferkel RD (2018) Scaffold-based therapies: proceedings of the international consensus meeting on cartilage repair of the ankle. Foot Ankle Int 39:41s–47s
Salaffi F, Stancati A, Silvestri CA, Ciapetti A, Grassi W (2007) Minimal clinically important changes in chronic musculoskeletal pain intensity measured on a numerical rating scale. Eur J Radiol 8:283–291
Saxena A, Eakin C (2007) Articular talar injuries in athletes: results of microfracture and autogenous bone graft. Am J Sports Med 35:1680–1687
Scranton PE Jr., McDermott JE (2001) Treatment of type V osteochondral lesions of the talus with ipsilateral knee osteochondral autografts. Foot Ankle Int 22:380–384
Seo SG, Kim JS, Seo DK, Kim YK, Lee SH, Lee HS (2018) Osteochondral lesions of the talus. Acta Orthop 89:462–467
Shimozono Y, Yasui Y, Ross AW, Miyamoto W, Kennedy JG (2017) Scaffolds based therapy for osteochondral lesions of the talus: a systematic review. World J Orthop 8:798–808
Spencer V, Illescas E, Maltes L, Kim H, Sathe V, Nukavarapu S (2018) Osteochondral tissue engineering: translational research and turning research into products. Adv Exp Med Biol 1058:373–390
Thermann H, Becher C, Vannini F, Giannini S (2014) Autologous matrix-induced chondrogenesis and generational development of autologous chondrocyte implantation. Oper Tech Orthop 24:210–215
Whittaker JP, Smith G, Makwana N, Roberts S, Harrison PE, Laing P, Richardson JB (2005) Early results of autologous chondrocyte implantation in the talus. J Bone Joint Surg Br 87:179–183
Yoon HS, Park YJ, Lee M, Choi WJ, Lee JW (2014) Osteochondral autologous transplantation is superior to repeat arthroscopy for the treatment of osteochondral lesions of the talus after failed primary Arthroscopic treatment. Am J Sports Med 42:1896–1903
Funding
Open access funding provided by Amsterdam UMC (University of Amsterdam).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
G.M.M.J. Kerkhoffs, J. N. Altink, S.A.S. Stufkens and J. Dahmen declare that they have no competing interests.
The study was performed in accordance with the current ethical standards.
Additional information
Editor
H. Waizy, Hannover
Illustrator
B. Brühmüller, Waghäusel
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kerkhoffs, G.M.M.J., Altink, J.N., Stufkens, S.A.S. et al. Talar OsteoPeriostic grafting from the Iliac Crest (TOPIC) for large medial talar osteochondral defects. Oper Orthop Traumatol 33, 160–169 (2021). https://doi.org/10.1007/s00064-020-00673-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00064-020-00673-9