
Abstract
Background
The use of the quick sequential organ failure assessment score (qSOFA) score and systemic inflammatory response syndrome (SIRS) criteria to identify patients at high risk for adverse outcomes in the emergency department (ED) remains controversial due to their low predictive performance and lack of supporting evidence. This study aimed to determine the predictive performance of qSOFA, SIRS, and the qSOFA + SIRS combinations for adverse outcomes.
Methods
All adult patients admitted to the ED with suspected infection were prospectively included. qSOFA scores ≥ 2, SIRS score ≥ 2 were defined as risk-positive for adverse outcome. Furthermore, combination‑1, which was defined as either qSOFA or SIRS positivity, and combination‑2, which was defined as both qSOFA and SIRS positivity, were also considered as risk-positive for adverse outcome. The predictive performance of qSOFA, SIRS, combination‑1, and combination‑2 for a composite adverse outcome within 30 days, including mortality, intensive care unit (ICU) admission, and non-ICU hospitalization, were determined.
Results
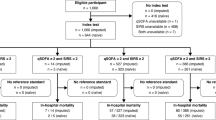
A total of 350 patients were included in the analysis. The composite outcome occurred in 211 (60.3%) patients within 30 days: mortality in 84 (24%), ICU admission in 78 (22.3%), and non-ICU hospitalization in 154 (44%). The sensitivity and specificity, respectively, were determined in predicting composite outcome as 0.34 and 0.93 for qSOFA, 0.81 and 0.31 for SIRS, 0.84 and 0.28 for combination‑1, and 0.31 and 0.96 for combination‑2.
Conclusion
The study results suggest that qSOFA and combination‑2 could be a useful tool for confirming patients at high risk for adverse outcomes. Although SIRS and combination‑1 could be helpful for excluding high-risk patients, the requirement of white blood cell counts limits their utilization for screening.
Zusammenfassung
Hintergrund
Der Einsatz des qSOFA-Scores („quick sequential organ failure assessment score“) und der SIRS-Kriterien („systemic inflammatory response syndrome“) zur Erkennung von Patienten in der Notaufnahme mit hohem Risiko unerwünschter Ergebnisse bleibt wegen ihrer niedrigen prädiktiven Aussagekraft und des Mangels an unterstützender Evidenz umstritten. Ziel der vorliegenden Arbeit war es, die Vorhersagekraft von qSOFA, SIRS und der Kombination qSOFA + SIRS für unerwünschte Ergebnisse zu untersuchen.
Methoden
Alle erwachsenen Patienten der Notfallaufnahme mit Verdacht auf Infektion wurden prospektiv in die Studie einbezogen. Als risikobehaftet für unerwünschte Ergebnisse wurden qSOFA-Scores ≥ 2 und ein SIRS-Score ≥ 2 definiert. Außerdem wurden auch Kombination 1, definiert als entweder qSOFA- oder SIRS-Positivität, und Kombination 2, definiert als sowohl qSOFA- als auch SIRS-Positivität, als risikobehaftet für unerwünschte Ergebnisse angesehen. Die Vorhersagekraft von qSOFA, SIRS, Kombination 1 und Kombination 2 für ein zusammengesetzten Endpunkt unerwünschter Ergebnisse innerhalb von 30 Tagen, einschließlich Mortalität, Aufnahme auf Intensivstation und sonstiger stationärer Aufnahme, wurden ermittelt.
Ergebnisse
In die Studie wurden 350 Patienten aufgenommen. Der zusammengesetzte Endpunkt trat bei 211 (60,3%) Patienten innerhalb von 30 Tagen ein: Mortalität in 84 (24%), Aufnahme auf Intensivstation in 78 (22,3%) und sonstige stationäre Aufnahme in 154 Fällen (44%). Die Sensitivität und Spezifität bei der Vorhersage des zusammengesetzten Endpunkts wurden mit 0,34 bzw. 0,93 für qSOFA; 0,81 bzw. 0,31 für SIRS; 0,84 bzw. 0,28 für Kombination 1 und 0,31 bzw. 0,96 für Kombination 2 ermittelt.
Schlussfolgerung
Den vorliegenden Ergebnissen zufolge könnten qSOFA und Kombination 2 ein hilfreiches Instrument zur Bestätigung des hohen Risikos unerwünschter Ergebnisse entsprechender Patienten sein. SIRS und Kombination 1 könnten zwar hilfreich zum Ausschluss von Hochrisikopatienten sein, aber ihr Einsatz zum Screening wird durch die dazu erforderlichen Leukozytenzahlen eingeschränkt.


Similar content being viewed by others


References
Viale P, Tedeschi S, Scudeller L et al (2017) Infectious diseases team for the early management of severe sepsis and septic shock in the emergency department. Clin Infect Dis 65(8):1253–1259. https://doi.org/10.1093/cid/cix548
Fernando SM, Tran A, Taljaard M et al (2018) Prognostic accuracy of the quick sequential organ failure assessment for mortality in patients with suspected infection, a systematic review and meta-analysis. Ann Intern Med. https://doi.org/10.7326/M17-2820
Liu YC, Luo YY, Zhang X et al (2019) Quick sequential organ failure assessment as a prognostic factor for infected patients outside the intensive care unit: a systematic review and meta-analysis. Intern Emerg Med. https://doi.org/10.1007/s11739-019-02036-0
Haydar S, Spanier M, Weems P, Wood S, Strout T (2017) Comparison of QSOFA score and SIRS criteria as screening mechanisms for emergency department sepsis. Am J Emerg Med 35(11):1730–1733. https://doi.org/10.1016/j.ajem.2017.07.001
VassarStats Website for statistical computation. Clinical research calculators. http://vassarstats.net. Accessed 9 July 2021
Seymour CW, Liu VX, Iwashyna TJ et al (2016) Assessment of clinical criteria for sepsis for the third international consensus definitions for sepsis and septic shock (sepsis-3). J Am Med Assoc 315(8):762–774. https://doi.org/10.1001/jama.2016.0288
Rudd KE, Seymour CW, Aluisio AR et al (2018) Association of the quick sequential (sepsis-related) organ failure assessment (qSOFA) score with excess hospital mortality in adults with suspected infection in low- and middle-income countries. JAMA. https://doi.org/10.1001/jama.2018.6229
Franchini S, Scarallo L, Carlucci M, Cabrini L, Tresoldi M (2019) SIRS or qSOFA? Is that the question? Clinical and methodological observations from a meta-analysis and critical review on the prognostication of patients with suspected sepsis outside the ICU. Intern Emerg Med 14(4):593–602. https://doi.org/10.1007/s11739-018-1965-0
Luo J, Jiang W, Weng L et al (2019) Usefulness of qSOFA and SIRS scores for detection of incipient sepsis in general ward patients: a prospective cohort study. J Crit Care 51:13–18. https://doi.org/10.1016/j.jcrc.2019.01.012
Song JU, Sin CK, Park HK, Shim SR, Lee J (2018) Performance of the quick sequential (sepsis-related) organ failure assessment score as a prognostic tool in infected patients outside the intensive care unit: a systematic review and meta-analysis. Crit Care 22(1):1–13. https://doi.org/10.1186/s13054-018-1952-x
Gando S, Shiraishi A, Abe T et al (2020) The SIRS criteria have better performance for predicting infection than qSOFA scores in the emergency department. Sci Rep. https://doi.org/10.1038/s41598-020-64314-8
Green SL, Smith MTD, Cairns C et al (2020) The combined SIRS + qSOFA (qSIRS) score is more accurate than qSOFA alone in predicting mortality in patients with surgical sepsis in an LMIC emergency department. World J Surg. https://doi.org/10.1007/s00268-019-05181-x
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
O. Yeşil, M. Pekdemir, İ.U. Özturan, N.Ö. Doğan, E. Yaka, S. Yılmaz, A. Karadaş and S.G. Pınar declare that they have no competing interests.
Institutional review board approval was obtained for the study (KÜ GOKAEK 2017/246). All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Consent to participate: Volunteers gave written informed consent before the study enrollment.
Additional information
Redaktion
Michael Buerke, Siegen

Scan QR code & read article online
Rights and permissions
About this article

Cite this article
Yeşil, O., Pekdemir, M., Özturan, İ.U. et al. Performance of qSOFA, SIRS, and the qSOFA + SIRS combinations for predicting 30-day adverse outcomes in patients with suspected infection. Med Klin Intensivmed Notfmed 117, 623–629 (2022). https://doi.org/10.1007/s00063-021-00870-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00063-021-00870-9
Keywords
- Sepsis
- Systemic inflammatory response syndrome
- Sequential organ failure assessment score
- Infections
- Emergency department