
Abstract
Objectives
To assess to what extent educational differences in total life expectancy (TLE) and disability-free life expectancy (DFLE) could be reduced by improving fruit and vegetable consumption in ten European countries.
Methods
Data from national census or registries with mortality follow-up, EU-SILC, and ESS were used in two scenarios to calculate the impact: the upward levelling scenario (exposure in low educated equals exposure in high educated) and the elimination scenario (no exposure in both groups). Results are estimated for men and women between ages 35 and 79 years.
Results
Varying by country, upward levelling reduced inequalities in DFLE by 0.1–1.1 years (1–10%) in males, and by 0.0–1.3 years (0–18%) in females. Eliminating exposure reduced inequalities in DFLE between 0.6 and 1.7 years for males (6–15%), and between 0.1 years and 1.8 years for females (3–20%).
Conclusions
Upward levelling of fruit and vegetable consumption would have a small, positive effect on both TLE and DFLE, and could potentially reduce inequalities in TLE and DFLE.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Socioeconomic inequalities in mortality risks are persistent in European countries, although previous research has shown that absolute inequalities between educational groups have decreased among men in several countries in the past decades (de Gelder et al. 2017; Mackenbach et al. 2016). Inequalities in mortality risk between low- and high-educated groups remain an important public health challenge, in particular for preventable causes of death (Mackenbach et al. 2008, 2015b).
In addition to inequalities in mortality, lower educational groups have shorter disability-free life expectancy (DFLE) than higher educational groups. Low socioeconomic groups are, to varying extent when comparing countries, consistently worse off than high socioeconomic groups, with inequalities for DFLE being larger than for total life expectancy (TLE) (Cambois et al. 2016b; Maki et al. 2013). If preventable causes of injury and disease could be reduced in low socioeconomic groups, inequalities between socioeconomic groups in TLE and DFLE would be reduced. Estimating the potential impact of addressing preventable causes and modifiable risk factors allows for both priority setting and for implementation of policies with realistic targets to decrease the inequality between socioeconomic groups.
One modifiable risk factor associated with an increased risk of both mortality and disability is low fruit and vegetable consumption. It has been established as a risk factor for all-cause mortality, with pathways via cardiovascular diseases, cancer, and other, yet unspecified diseases causing increased mortality rates (Agudo et al. 2007; Aune et al. 2017; Bellavia et al. 2013; Genkinger et al. 2004; Leenders et al. 2013; Nguyen et al. 2016; Oyebode et al. 2014; Rissanen et al. 2003). Inverse dose–response relationships for fruit and vegetable consumption and the onset of chronic diseases have been described previously, stressing the risk of consuming inadequate amounts of fruit and vegetables (Bazzano et al. 2002; Dauchet et al. 2006; He et al. 2006; Leenders et al. 2014; Wang et al. 2014a, 2015). Fruit and vegetable consumption varies between educational groups across Europe, with larger differences in Northern European countries than in Mediterranean countries (Prattala et al. 2009). However, a higher level of education is overall associated with a higher consumption of fruit and vegetables (De Irala-Estevez et al. 2000).
This raises the question to what extent educational differences in TLE and DFLE can be reduced by improving fruit and vegetable consumption, similarly as has been shown for mortality rates for smoking (Kulik et al. 2013), obesity (Hoffmann et al. 2015), and alcohol consumption (Mackenbach et al. 2015a). The aim of this study is, therefore, to estimate the impact of improving fruit and vegetable consumption on inequalities in TLE and DFLE between socioeconomic groups in European countries. We evaluate the effect of two scenarios: the upward levelling scenario, where exposure in low educational groups is set to the level of exposure in the high educated, and the elimination scenario, with zero exposure to low fruit and vegetable consumption in each educational group.
Methods
Data
Mortality data by age, sex, and level of education were obtained for each country from national census or registries with mortality follow-up including at least data on years 2010 or later, where available. Where no follow-up data were available, we used cross-sectional data provided by the respective countries (see Table 1). Data for Finland, Denmark, United Kingdom, Belgium, Austria, Switzerland, Spain, Poland, Lithuania, and Estonia were included. We included data for ages 35–79 years, excluding age 80 and over since data on mortality by educational level are less reliable in this category.
Data on disability prevalence were obtained from the European Union Statistics on Income and Living Conditions (EU-SILC), years 2010 and 2014, for each selected country. These particular years were selected to avoid bias of including respondents multiple times, since EU-SILC is a rotating panel survey. To assess disability, EU-SILC used the Global Activity Limitation Indicator (GALI). It is a validated and relatively accurate indicator, although there are some inconsistencies between countries (Berger et al. 2015; Jagger et al. 2010; Van Oyen et al. 2006, 2018). The GALI consists of one item, asking subjects “For at least the past 6 months, to what extent have you been limited because of a health problem in activities people usually do?” Respondents were classified as having a disability if they responded “Yes, severely” or “Yes, to some extent”. GALI is used to calculate the European disability-free life expectancy indicator “Healthy Life Years” (HLY).
Data on prevalence of low fruit and vegetables by sex, age, educational level, and country were obtained from round 7 (2014) of European Social Survey (ESS). The ESS aims at charting social structure in Europe. Round 7 included a module on health and nutrition (Eikemo et al. 2017). Subjects were asked how many times a day they eat fruit and vegetables in two separate questions. The answering categories were: “Three times or more a day”, “Twice a day”, “Once a day”, “Less than once a day, but at least 4 times a week”, “Less than 4 times a week, but at least once a week”, “Less than once a week”, and “Never”. In our study, fruit and vegetable consumption was considered low if subjects consumed either fruit or vegetables, or both less than once a day. For the countries included in these analyses, response rates range from 43.6 to 68.9%, with high non-response rates observed in the United Kingdom, Austria, Denmark, and Switzerland.
The highest completed level of education was used as an indicator of socioeconomic status. We chose level of education, since it is usually determined early in life, and remains stable during life thereafter. In addition, education was systematically assessed in all three data sources. Level of education was categorized into three levels: low level of education (ISCED 0–2), medium level of education (ISCED 3–4), and high level of education (ISCED 5–6). In the presentation of the results, we focused on inequalities between low level of education and high level of education. Results for medium educated are available in the electronic supplementary material.
We obtained relative risks of low fruit and vegetable consumption on all-cause mortality and disability from the literature. Wang et al. (2014b) reported hazard ratios for mortality attributable to low fruit and vegetable consumption in a meta-analysis, comprising data from seven studies conducted in the United States and Europe, with a total of 553,698 participants, and 42,219 deaths with at least 11 years of follow-up. Estimates of the included studies were adjusted for age, sex, and risk factors such as BMI, alcohol consumption, smoking, and physical activity. We used these hazard ratios to compute a pooled relative risk, weighing them by the size of the corresponding group in ESS (Electronic supplementary material, Table A1). This resulted in a relative risk for mortality in subjects with no daily consumption of fruit and vegetables as compared to those consuming fruit and vegetables at least once a day of 1.2 (95% CI 1.1–1.3).
For disability, fewer studies and no meta-analyses assessing the relationship with fruit and vegetable consumption were available. In our analyses, therefore, we used the relative risk found by Artaud et al. (2013). They assessed the effects of health risk behaviours on several health outcomes, corrected for other risk factors. Their analysis included 3982 French subjects aged 65 and over, a subpopulation of the Three-City Study. Through personal communication, they provided a relative risk that matched the definition of fruit and vegetable consumption in this study. They calculated that the relative risk for this relationship is 1.20 (95% CI 1.06–1.35).
Statistical methods and models
First, age-standardized mortality rates and prevalences of disability were calculated for each country, using the European Standard population 2013 for descriptive purposes (Eurostat 2013). Restricted cubic spline models were used to smooth weighted age-, gender-, and education-specific prevalences of low fruit and vegetable consumption and prevalence of disability.
Second, population attributable fractions (PAFs) were calculated by combining smoothed prevalences of exposure to a risk factor, specified by age, gender, and level education in the ith exposure category (Pi), the prevalence of exposure to a risk factor, specified by age, gender, and level education, in the ith exposure category in an alternative exposure scenario (\(P_{i}^{\prime }\)), and relative risks (RRi) for the number of exposure categories (n) (formula 1).
Using PAFs, the impact of low fruit and vegetable consumption on mortality rates and disability prevalence in each country was calculated (Hoffmann et al. 2013) for each scenario of exposure (observed, upward levelling, and elimination) by age, gender, and education, as previously explained by Hoffmann et al. (2015). Third, the Sullivan method, an extension of the standard life table method, was used to calculate DFLE (Sullivan 1971). In the Sullivan method, person years are split into years with and without disability by using the prevalence of disability. We used partial TLE and DFLE, which refers to the number of years lived (TLE) or lived free from disability (DFLE) between the ages of 35 and 79. Confidence intervals for these estimates were derived from 1000 bootstrapped samples, taking into account uncertainty for the GALI estimates, fruit and vegetable consumption, and mortality. Uncertainty with regard to the used RRs of low fruit and vegetable consumption on outcomes was not accounted for these samples. Therefore, a sensitivity analysis was conducted, evaluating the impact of imputing alternative values for the relative risks in the PAF calculations.
Scenarios
Two counterfactual scenarios were carried out. First, an upward levelling scenario, similar to Hoffmann et al. (2015), was calculated, assessing the effect of altering the prevalence of low fruit and vegetable consumption in the low-educated group to the level of the high-educated group. By comparing the result of this scenario to the current situation, the gain that could be achieved in low educated was calculated.
Second, the effect of eliminating exposure to low fruit and vegetable consumption was calculated, by setting the prevalence of low fruit and vegetable consumption to zero in all educational groups. By comparing the result of this elimination scenario to the current situation, the loss in TLE and DFLE due to low fruit and vegetable consumption, or the maximum achievable gain due to zero exposure to low fruit and vegetable consumption was calculated.
Results
Prevalence of low fruit and vegetable consumption
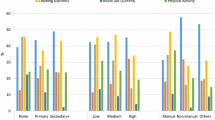
Age-standardized prevalences of low fruit and vegetable consumption are presented in Table 2 for each country, stratified by sex, and level of education. In most countries, the prevalence of low fruit and vegetable consumption was highest in the low-educated group. Prevalences were similar in both educational groups in Austrian and Polish males, and in Swiss females. In some populations, exposure to low fruit and vegetables consumption was the lowest in the medium educated (Electronic supplementary material, Table A4). The highest prevalence of low fruit and vegetable consumption was seen for Lithuania. The largest difference between low and high educated was seen in Lithuania as well, where the prevalence of low fruit and vegetable consumption is 40.6% points (males), and 40.2% points (females) higher in the low educated.
Total life expectancy
TLE between the ages of 35 and 80 years varied by country, sex, and educational level (Table 3 and Fig. 1, Electronic supplementary material Table A9). In low educated, the average TLE was 37.2 years for males and 41.2 years for females. In Estonia, Lithuania, and Poland, TLE for low educated was particularly unfavourable compared to other countries, especially for males. The average differences in TLE between low and high-educated groups were 4.3 years for males and 1.5 years for females. The smallest educational differences in TLE between low- and high-educated groups were seen in Spain, with differences of 2.1 years in males and 0.6 years in females. The largest educational differences were seen in Lithuania, with 8.2 years difference in males, and 4.5 years in females.

Educational inequalities in total life expectancy, disability-free life expectancy as observed and for the elimination and upward levelling scenarios for men and women between ages 35 and 79 in ten European countries
In the upward levelling scenario, a reduction in the gap in TLE between low and high educated was seen in almost all countries, with an average reduction of 0.2 years in low-educated males and 0.1 years in low-educated females (Table 3 and Fig. 1, Electronic supplementary material Table A9). Upward levelling had the largest effect in low-educated Lithuanian males with an increase of 0.6 years, and an increase of 0.4 years in women. In other populations, such as Austrian, Polish, and Spanish males, and in Austrian, Belgian, Spanish, and Swiss females, the gains of upward levelling were 0.1 years of TLE or less.
In the elimination scenario, TLE would increase to varying extent in all countries, with larger increases for low-educated groups than for high-educated groups (Table 3 and Fig. 1, Electronic supplementary material Table A9). On average, TLE would increase by 0.6 years from 37.2 years to 37.8 years in low-educated males and 0.2 years in low-educated females, as opposed to increases of 0.2 years in high-educated males and 0.1 years in high-educated females. Possible gains in TLE in low-educated males varied between 0.4 years (UK) and 1.4 years (Lithuania); in low-educated females, possible gains in TLE varied between 0.1 years (Switzerland) and 0.8 years (Lithuania). Inequalities in TLE between educational groups could be reduced by on average 0.4 years in males, ranging from 0.3 years (UK) to 1.0 years (Lithuania), and 0.2 years in females, ranging from 0.0 years (Switzerland) to 0.6 years (Lithuania) for females.
Disability-free life expectancy
The difference in DFLE between low and high educated was larger than for TLE, with 7.9 years of difference in DFLE for males and 5.9 years for females. Between countries, differences were larger for lower levels of education than for higher levels of education (Table 3 and Fig. 1, Electronic supplementary material A9). DFLE varied between 16.6 years and 28.2 years in low-educated males, and between 18.0 years and 27.9 years in low-educated females. Educational differences in DFLE in Estonia and Lithuania were particularly large, for both males and females.
In the upward levelling scenario, inequalities could be reduced by 0.5 years for males and 0.6 years for females. The largest estimated reductions in the gap between educational groups would be seen in Lithuania, with 1.1 years of DFLE in males, and 1.3 years in females. In other populations, such as Polish males and Swiss females, reductions were practically absent.
The gap in DFLE between educational groups could be reduced by 0.8 years for both males and females. In the elimination scenario, DFLE would improve by 1.5 years in low-educated males, and 1.2 years in low-educated females, and by 0.7 years in high-educated males and 0.4 years in high-educated females. Possible gains in DFLE for low-educated males varied between 1.3 and 2.6 years, and for low-educated females between 0.7 years and 2.4 years (Table 3 and Fig. 1). The gains in DFLE for high-educated individuals varied between 0.4 years (UK) and 1.5 years (Austria) for males, and between 0.3 years (UK) and 0.9 years (Estonia) for females. For males, the possible reduction in the gap in DFLE between educational groups ranged from 0.6 years (Poland, Spain) to 1.7 years (Lithuania). For females, the possible reduction in the gap in DFLE between educational groups ranged from 0.1 years (Switzerland) to 1.8 years (Lithuania).
Discussion
Improving consumption of fruit and vegetables in low-educated groups to the level of high educated would have a small, but positive effect on both total life expectancy (TLE) and disability-free life expectancy (DFLE), and has the potential to reduce inequalities in health, in particular in countries where inequalities in TLE, DFLE, and fruit and vegetable consumption are large. Zero exposure to low fruit and vegetable consumption would improve TLE and DFLE and decrease educational inequalities in TLE and DFLE, but the effect varies between countries. In more than half of the assessed countries, 50% or more of the potential effect of eliminating low fruit and vegetable consumption could be achieved by upward levelling.
Strengths and limitations
Data
The main advantage of the PAF method is that the best available data of separate sources can be combined into one effect estimate. Longitudinal health surveys generally lack power to assess associations between fruit and vegetable consumption and mortality and disability directly, and providing results for several countries is often difficult.
Consumption of fruit and vegetables was measured in ESS as frequency of use, which introduces uncertainty on total consumption measured in grams. However, previous research indicated that the number of servings of fruit and vegetables correlates with an average consumed amount measured in grams (Nothlings et al. 2006).
Due to cross-sectional assessment of fruit and vegetables consumption in ESS, no statements can be made with regard to duration of exposure. We assumed reported frequencies of consumption to be representative for consumption patterns of a respondent averaged over a longer period of time. However, there are indications that traditional Mediterranean countries, known for their high consumption of fruit and vegetables, and other European countries have grown to be more alike in their consumption patterns than in years past (CIHEAM/FAO 2015). This underlines the difficulty to assess the impact of exposure to low fruit and vegetable consumption, which may vary over time for each individual respondent.
We also compared prevalences of low fruit and vegetable consumption in ESS with data from other sources, namely the DAFNE project, the European Food Safety Authority (EFSA), and the European Health Interview Survey (EHIS) (results not shown). No clear pattern in fruit and vegetable consumption per country could be established when comparing these sources, possibly due to differences in measurement units and sampling design. However, even for data sources using similar measurement units, no clear pattern could be established.
Mortality data obtained from mortality follow-up were supplied per country in a standard format. This improved comparability and allowed for stratification by educational level, sex, and age group. We used cross-sectional data for Poland since no longitudinal data were available, which might introduce selection bias and warrants caution in interpreting the results.
Data on disability were assessed in a similar manner in international surveys. Nonetheless, cultural differences between countries, discrepancies in translations of the questions, and differences between socioeconomic groups in the reporting of disabilities are important issues and should warrant careful interpretation of results (Cambois et al. 2016a). The same may apply to the reporting of fruit and vegetable consumption. Additionally, both data on disability and fruit and vegetable consumption are self-reported, which could lead to both over- and underestimation of disability prevalence and exposure to low fruit and vegetable consumption.
Relative risks
For the PAF method, relative risks for mortality and disability in relation to low fruit and vegetable consumption were obtained from the literature. Since no significantly different relative risks specified by country, educational group, or age group were reported, we assumed the effect of fruit and vegetable consumption on all-cause mortality and disability to be the same across countries, educational groups, age groups, and sexes (Artaud et al. 2013; Wang et al. 2014b). A sensitivity analysis by Wang et al. found no significant difference for sex. For disability, we used a RR based on a cohort study among persons aged 65 and over, which might have yielded conservative estimates, as relative risks generally decrease with increase in age.
We conducted a sensitivity analysis to assess the impact of uncertainty around the used relative risks of disability, and, to a lesser extent, all-cause mortality associated with low fruit and vegetable consumption (see Electronic supplementary material, Table A7). We evaluated several combinations of relative risks. In the first series, we changed the relative risks for mortality and disability from the original values of 1.2 to 1.05 and 1.35 for both mortality and disability. These relative risks are based on the confidence interval for the relative risk reported by Wang et al. (2014b). The effects of upward levelling, calculated in the main analysis, would minimize if the relative risks used in the calculations would decrease, although there might still be a noteworthy effect in Lithuania. In a second series, we kept the relative risk for mortality set at 1.2, while varying the relative risk for disability by 1.02, 1.05, 1.2, and 1.35. The gap in DFLE between low and high educated could potentially be reduced by up to 2.0 years by upward levelling if the relative risk was to be larger. There might be potential for reducing inequalities in DFLE if the relative risk were to be smaller than the relative risk used in the main analysis, although these effects might prove to be not statistically significant.
Interpretation and comparison with other studies
Our results show that improving consumption of fruit and vegetable consumption in low-educated groups to the level of high-educated groups would have a small, yet positive, effect on both TLE and DFLE in most countries and indicates a potential to reduce inequalities in TLE and DFLE. This was in particular seen in countries where both inequalities in TLE, DFLE, and the differences in prevalence of low fruit and vegetable consumption between low and high educated were large, such as Lithuania. This gradient in fruit and vegetable consumption by level of education in Lithuania has also been described by Kriaucioniene et al. (2012). In the upward levelling scenario, high educated can be regarded as forerunners, and their level of consumption could be viewed as achievable for the entire population of that country.
Since our definition of adequate fruit and vegetable consumption is relatively lenient, improvements for those not meeting this level of consumption are within reach. Additionally, beneficial health effects could be expected if consumption would meet the World Health Organizations recommendation of at least 400 grams of fruits and vegetables a day, since a dose–response relationship for health benefits of fruit and vegetable consumption has been described as well (Wang et al. 2014b; Wiseman 2008). This is in particular the case for countries in Eastern Europe, where the average consumption of fruit and vegetables is further below this WHO recommendation than other European countries (Lock et al. 2005).
A review by McGill has shown that evidence supporting health education interventions was inconclusive, and might even widen socioeconomic inequalities (McGill et al. 2015). However, reducing financial barriers for consuming fruit and vegetables, for example by lowering prices, could be an effective measure to reduce socioeconomic inequalities (McGill et al. 2015). However, further research on successful implementation and the effectiveness of health interventions is necessary.
Our study was the first to assess the impact of fruit and vegetable consumption on educational differences in TLE and DFLE. In the Global Burden of Disease (GBD) study, the impact of a diet low in fruits and a diet low in vegetables on the years of life lost (YLL) and years lived with disability (YLD) was calculated, but not on DFLE nor by level of education. For the total population, we compared their results for mortality, and the percentage of life expectancy with disability (the difference between TLE and DFLE) attributable to low fruit and vegetable consumption to our PAFs (Electronic supplementary material, Table A8). For mortality, results in the GBD study were similar to what we found. For disability, however, we found the fractions in the GBD study to be 3 to 8 times lower than our fractions. These differences for disability may reflect differences in methods and outcome measure, in addition to differences in defining low fruit and vegetable consumption. In the GBD study, only associations between a diet low in fruit or vegetables and the incidence of several diseases, such as cardiovascular disease, type 2 diabetes and neoplasms were included in the calculations. There are indications that low fruit and vegetable consumption is also associated with additional diseases known for causing disability (Boeing et al. 2012), such as cataract (Huang et al. 2015), depression (Liu et al. 2016), and osteoporosis (Luo et al. 2016).
Conclusion and implications
Improving consumption of fruit and vegetables in low-educated groups to the level of high educated would have a small positive effect on both TLE and DFLE. In particular, in countries where inequalities in TLE, DFLE, and fruit and vegetable consumption are large, such as Lithuania, implementing interventions to improve fruit and vegetable consumption among low-educated groups could be worthwhile. Interventions reducing financial barriers for consuming fruit and vegetables should be considered.
References
Agudo A, Cabrera L, Amiano P et al (2007) Fruit and vegetable intakes, dietary antioxidant nutrients, and total mortality in Spanish adults: findings from the Spanish cohort of the European Prospective Investigation into Cancer and Nutrition (EPIC-Spain). Am J Clin Nutr 85:1634–1642
Artaud F, Dugravot A, Sabia S et al (2013) Unhealthy behaviours and disability in older adults: three-City Dijon cohort study. BMJ. https://doi.org/10.1136/bmj.f4240
Aune D, Giovannucci E, Boffetta P et al (2017) Fruit and vegetable intake and the risk of cardiovascular disease, total cancer and all-cause mortality—a systematic review and dose–response meta-analysis of prospective studies. Int J Epidemiol 46:1029–1056. https://doi.org/10.1093/ije/dyw319
Bazzano LA, He J, Ogden LG et al (2002) Fruit and vegetable intake and risk of cardiovascular disease in US adults: the first National Health and Nutrition Examination Survey Epidemiologic Follow-up Study. Am J Clin Nutr 76:93–99
Bellavia A, Larsson SC, Bottai M et al (2013) Fruit and vegetable consumption and all-cause mortality: a dose–response analysis. Am J Clin Nutr 98:454–459. https://doi.org/10.3945/ajcn.112.056119
Berger N, Van Oyen H, Cambois E et al (2015) Assessing the validity of the Global Activity Limitation Indicator in fourteen European countries. BMC Med Res Methodol. https://doi.org/10.1186/1471-2288-15-1
Boeing H, Bechthold A, Bub A et al (2012) Critical review: vegetables and fruit in the prevention of chronic diseases. Eur J Nutr 51:637–663. https://doi.org/10.1007/s00394-012-0380-y
Cambois E, Grobon S, Van Oyen H et al (2016a) Impact of question wording on the measurement of activity limitation: evidence from a randomized test in France. J Aging Health 28:1315–1338. https://doi.org/10.1177/0898264316656504
Cambois E, Sole-Auro A, Bronnum-Hansen H et al (2016b) Educational differentials in disability vary across and within welfare regimes: a comparison of 26 European countries in 2009. J Epidemiol Community Health 70:331–338. https://doi.org/10.1136/jech-2015-205978
CIHEAM/FAO (2015) Mediterranean food consumption patterns: diet, environment, society, economy and health. A White Paper Priority 5 of Feeding Knowledge Programme, Expo Milan, vol CIHEAM-IAMB, Bari/FAO, Rome
Dauchet L, Amouyel P, Hercberg S et al (2006) Fruit and vegetable consumption and risk of coronary heart disease: a meta-analysis of cohort studies. J Nutr 136:2588–2593
De Gelder R, Menvielle G, Costa G et al (2017) Long-term trends of inequalities in mortality in 6 European countries. Int J Public Health 62:127–141. https://doi.org/10.1007/s00038-016-0922-9
De Irala-Estevez J, Groth M, Johansson L et al (2000) A systematic review of socio-economic differences in food habits in Europe: consumption of fruit and vegetables. Eur J Clin Nutr 54:706–714. https://doi.org/10.1038/sj.ejcn.1601080
Eikemo TA, Bambra C, Huijts T et al (2017) The first pan-European sociological health inequalities survey of the general population: the European social survey rotating module on the social determinants of health. Eur Sociol Rev 33:137–153. https://doi.org/10.1093/esr/jcw019
Eurostat (2013) Revision of the European Standard Population—Report of Eurostat’s task force
Genkinger JM, Platz EA, Hoffman SC et al (2004) Fruit, vegetable, and antioxidant intake and all-cause, cancer, and cardiovascular disease mortality in a community-dwelling population in Washington County, Maryland. Am J Epidemiol 160:1223–1233. https://doi.org/10.1093/aje/kwh339
He FJ, Nowson CA, MacGregor GA (2006) Fruit and vegetable consumption and stroke: meta-analysis of cohort studies. Lancet 367:320–326. https://doi.org/10.1016/S0140-6736(06)68069-0
Hoffmann R, Eikemo TA, Kulhanova I et al (2013) The potential impact of a social redistribution of specific risk factors on socioeconomic inequalities in mortality: illustration of a method based on population attributable fractions. J Epidemiol Community Health 67:56–62. https://doi.org/10.1136/jech-2011-200886
Hoffmann R, Eikemo TA, Kulhanova I et al (2015) Obesity and the potential reduction of social inequalities in mortality: evidence from 21 European populations. Eur J Public Health 25:849–856. https://doi.org/10.1093/eurpub/ckv090
Huang GQ, Wu LW, Qiu LH et al (2015) Association between vegetables consumption and the risk of age-related cataract: a meta-analysis. Int J Clin Exp Med 8:18455–18461
Jagger C, Gillies C, Cambois E et al (2010) The Global Activity Limitation Index measured function and disability similarly across European countries. J Clin Epidemiol 63:892–899. https://doi.org/10.1016/j.jclinepi.2009.11.002
Kriaucioniene V, Klumbiene J, Petkeviciene J et al (2012) Time trends in social differences in nutrition habits of a Lithuanian population: 1994–2010. BMC Public Health. https://doi.org/10.1186/1471-2458-12-218
Kulik MC, Hoffmann R, Judge K et al (2013) Smoking and the potential for reduction of inequalities in mortality in Europe. Eur J Epidemiol 28:959–971. https://doi.org/10.1007/s10654-013-9860-5
Leenders M, Sluijs I, Ros MM et al (2013) Fruit and vegetable consumption and mortality European prospective investigation into cancer and nutrition. Am J Epidemiol 178:590–602. https://doi.org/10.1093/aje/kwt006
Leenders M, Boshuizen HC, Ferrari P et al (2014) Fruit and vegetable intake and cause-specific mortality in the EPIC study. Eur J Epidemiol 29:639–652. https://doi.org/10.1007/s10654-014-9945-9
Liu X, Yan Y, Li F et al (2016) Fruit and vegetable consumption and the risk of depression: a meta-analysis. Nutrition 32:296–302. https://doi.org/10.1016/j.nut.2015.09.009
Lock K, Pomerleau J, Causer L et al (2005) The global burden of disease attributable to low consumption of fruit and vegetables: implications for the global strategy on diet. Bull World Health Organ 83:100–108
Luo S, Li Y, Luo H et al (2016) Increased intake of vegetables, but not fruits, may be associated with reduced risk of hip fracture: a meta-analysis. Sci Rep 6:19783. https://doi.org/10.1038/srep19783
Mackenbach JP, Stirbu I, Roskam AJ et al (2008) Socioeconomic inequalities in health in 22 European countries. N Engl J Med 358:2468–2481. https://doi.org/10.1056/NEJMsa0707519
Mackenbach JP, Kulhanova I, Bopp M et al (2015a) Inequalities in alcohol-related mortality in 17 European countries: a retrospective analysis of mortality registers. PLoS Med 12:e1001909. https://doi.org/10.1371/journal.pmed.1001909
Mackenbach JP, Kulhanova I, Bopp M et al (2015b) Variations in the relation between education and cause-specific mortality in 19 European populations: a test of the “fundamental causes” theory of social inequalities in health. Soc Sci Med 127:51–62. https://doi.org/10.1016/j.socscimed.2014.05.021
Mackenbach JP, Kulhanova I, Artnik B et al (2016) Changes in mortality inequalities over two decades: register based study of European countries. BMJ 353:i1732
Maki N, Martikainen P, Eikemo T et al (2013) Educational differences in disability-free life expectancy: a comparative study of long-standing activity limitation in eight European countries. Soc Sci Med 94:1–8. https://doi.org/10.1016/j.socscimed.2013.06.009
McGill R, Anwar E, Orton L et al (2015) Are interventions to promote healthy eating equally effective for all? Systematic review of socioeconomic inequalities in impact. BMC Public Health 15:457. https://doi.org/10.1186/s12889-015-1781-7
Nguyen B, Bauman A, Gale J et al (2016) Fruit and vegetable consumption and all-cause mortality: evidence from a large Australian cohort study. Int J Behav Nutr Phys Act. https://doi.org/10.1186/s12966-016-0334-5
Nothlings U, Murphy SP, Sharma S et al (2006) A comparison of two methods of measuring food group intake: grams vs servings. J Am Diet Assoc 106:737–739. https://doi.org/10.1016/j.jada.2006.02.006
Oyebode O, Gordon-Dseagu V, Walker A et al (2014) Fruit and vegetable consumption and all-cause, cancer and CVD mortality: analysis of Health Survey for England data. J Epidemiol Community Health 68:856–862. https://doi.org/10.1136/jech-2013-203500
Prattala R, Hakala S, Roskam AJR et al (2009) Association between educational level and vegetable use in nine European countries. Public Health Nutr 12:2174–2182. https://doi.org/10.1017/S136898000900559x
Rissanen TH, Voutilainen S, Virtanen JK et al (2003) Low intake of fruits, berries and vegetables is associated with excess mortality in men: the Kuopio Ischaemic Heart Disease Risk Factor (KIHD) Study. J Nutr 133:199–204
Sullivan DF (1971) A single index of mortality and morbidity. HSMHA Health Rep 86:347–354
Van Oyen H, Van der Heyden J, Perenboom R et al (2006) Monitoring population disability: evaluation of a new Global Activity Limitation Indicator (GALI). Soz Praventivmed 51:153–161
Van Oyen H, Bogaert P, Yokota RTC et al (2018) Measuring disability: a systematic review of the validity and reliability of the Global Activity Limitations Indicator (GALI). Arch Public Health 76:25. https://doi.org/10.1186/s13690-018-0270-8
Wang Q, Chen Y, Wang X et al (2014a) Consumption of fruit, but not vegetables, may reduce risk of gastric cancer: results from a meta-analysis of cohort studies. Eur J Cancer 50:1498–1509
Wang X, Ouyang YY, Liu J et al (2014b) Fruit and vegetable consumption and mortality from all causes, cardiovascular disease, and cancer: systematic review and dose–response meta-analysis of prospective cohort studies. BMJ. https://doi.org/10.1136/bmj.g4490
Wang Y, Li F, Wang Z et al (2015) Fruit and vegetable consumption and risk of lung cancer: a dose–response meta-analysis of prospective cohort studies. Lung Cancer 88:124–130. https://doi.org/10.1016/j.lungcan.2015.02.015
Wiseman M (2008) The second World Cancer Research Fund/American Institute for Cancer Research expert report. Food, nutrition, physical activity, and the prevention of cancer: a global perspective. Proc Nutr Soc 67:253–256. https://doi.org/10.1017/S002966510800712x
Acknowledgements
The permission of the Office for National Statistics to use the Longitudinal Study is gratefully acknowledged, as is the help provided by staff of the Centre for Longitudinal Study Information & User Support (CeLSIUS). CeLSIUS is supported by the ESRC Census of Population Programme (Award Ref: ES/K000365/1). The authors alone are responsible for the interpretation of the data. This work contains statistical data from ONS which is Crown Copyright. The use of the ONS statistical data in this work does not imply the endorsement of the ONS in relation to the interpretation or analysis of the statistical data. This work uses research datasets which may not exactly reproduce National Statistics aggregates. The authors thank Fanny Artaud and Alexis Elbaz for providing the relative risk for disability in relation to low fruit and vegetable consumption.
Funding
Support was provided by the European Commission Research and Innovation Directorate General (Horizon 2020 Grant No. 633666 to the LIFEPATH project). The sponsor had no role in the study design; in the collection, analysis, and interpretation of data; in the writing of the report; and in the decision to submit the article for publication.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors state that they do not have any conflict of interest.
Ethical approval
This article does not contain any studies with human participants performed by any of the authors.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Baars, A.E., Rubio-Valverde, J.R., Hu, Y. et al. Fruit and vegetable consumption and its contribution to inequalities in life expectancy and disability-free life expectancy in ten European countries. Int J Public Health 64, 861–872 (2019). https://doi.org/10.1007/s00038-019-01253-w
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00038-019-01253-w