
Abstract
Purpose
To determine the effects of a priming technique with respect to onset time and duration of action of rocuronium ( 1.5 × ED95, 2.0 × ED95) in a pediatric patient population.
Methods
Eighty-four children, age one to seven years undergoing elective pediatric surgery, were studied in a randomized controlled trial. Neuromuscular function was assessed by accelerometry in response to single-twitch stimulation to assess onset of neuromuscular block, followed by train-of-four (TOF) stimulation at the wrist every 15 sec. Children were randomly allocated to one of four groups: Groups 1 and 3 received saline placebo, followed one minute later by a single bolus dose of rocuronium 0.45 mg·kg-1 iv (1.5 × ED95) and 0.6 mg kg-1 iv (2.0 x ED95), respectively. Patients in Groups 2 and 4 received an initial dose of rocuronium 0.045 mg·kg-1 iv and 0.06 mg·kg-1 iv, respectively, followed one minute later by rocuronium 0.405 mg·kg-1 and 0.54 mg·kg-1iv, respectively.
Results
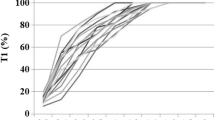
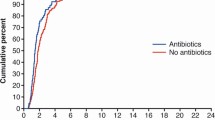
Rocuronium priming significantly accelerated the time to maximum rocuronium-induced neuromuscular block when compared to placebo [median (95% confidence interval)]: 122.5 (98-186) vs 92.5 (68-116) sec (1.5 × ED95, Group 1 vs Group 2, P < 0.05) and 85 (60-142) vs 55 (48-72) sec (2.0 × ED95, Group 3 vs Group 4, P < 0.05), respectively. Spontaneous recovery to a TOF-ratio ≥ 0.9 was dose-dependent and not influenced by priming.
Conclusion
Priming accelerated the onset of rocuronium in children. A priming interval of one minute and a cumulative dose of rocuronium 1.5 × ED95 resulted in an onset of neuromuscular block comparable to a single dose of rocuronium (2.0 × ED95).
Objectif
Déterminer les effets d’une technique d’amorçage sur le délai d’installation et la durée d’action du rocuronium (1,5 × ED95, 2,0 × ED95) chez les enfants.
Méthode
Quatre-vingt-quatre enfants âgés de un à sept ans et subissant une chirurgie pédiatrique élective ont été recrutés dans cette étude randomisée contrôlée. La fonction neuromusculaire a été évaluée par accélérométrie en réponse à une stimulation simple afin de mesurer le début du bloc neuromusculaire, suivie par une stimulation en train-de-quatre (TOF) au poignet toutes les 15 sec. Les enfants ont été randomisés en quatre groupes: les groupes 1 et 3 ont reçu un placebo de sérum physiologique, suivi une minute plus tard par une dose unique en bolus de rocuronium 0,45 mg·kg-1 iv (1,5 × ED95) et 0,6 mg kg-1 iv (2,0 × ED95), respectivement. Les patients des groupes 2 et 4 ont reçu une dose initiale de rocuronium 0,045 mg·kg-1 iv et 0,06 mg·kg-1 iv, respectivement, suivie une minute plus tard par du rocuronium 0,405 mg·kg-1 et 0,54 mg·kg-1iv, respectivement.
Résultats
L’amorçage avec le rocuronium a accéléré de façon significative le délai jusqu’au bloc neuromusculaire maximum induit par le rocuronium comparé au placebo [moyenne (intervalle de confiance 95 %)]: 122,5 (98-186) vs 92,5 (68-116) sec (1,5 × ED95, groupe 1 vs groupe 2, P < 0,05) et 85 (60-142) vs 55 (48-72) sec (2,0 × ED95, groupe 3 vs groupe 4, P < 0,05), respectivement. La récupération spontanée d’un ratio TOF ≥ 0,9 était dépendante de la dose et n’a pas été influencée par l’amorçage.
Conclusion
L'amorçage a accéléré le début de l’action du rocuronium chez les enfants. Un intervalle d’amorçage d’une minute et une dose cumulative de rocuronium 1,5 × ED95 a eu pour résultat un délai de bloc neuromusculaire comparable à celui obtenu avec une dose unique de rocuronium (2,0 × ED95).
Article PDF
Similar content being viewed by others

Avoid common mistakes on your manuscript.
References
Fuchs-Buder T, Tassonyi E. Intubating conditions and time course of rocuronium-induced neuromuscular block in children. Br J Anaesth 1996; 77:335–8.
Magorian T, Flannery KB, Miller RD. Comparison of rocuronium, succinylcholine, and vecuronium for rapid-sequence induction of anesthesia in adult patients. Anesthesiology 1993; 79:913–8.
Gibbs NM, Rung GW, Braunegg PW, Martin DE. The onset and duration of neuromuscular blockade using combinations of atracurium and vecuronium. Anaesth Intensive Care 1991; 19:96–100.
Naguib M. Different priming techniques, including mivacurium, accelerate the onset of rocuronium. Can J Anaesth 1994; 41:902–7.
Taboada JA, Rupp SM, Miller RD. Refining the priming principle for vecuronium during rapid-sequence induction of anesthesia. Anesthesiology 1986; 64:243–7.
England AJ, Margarson MP, Feldman SA. Tracheal intubation conditions after one minute: rocuroni-um and vecuronium, alone and in combination. Anaesthesia 1997; 52:336–40.
Yavascaoglu B, Cebelli V, Kelebek N, Uckunkaya N, Kutlay O. Comparison of different priming techniques on the onset time and intubating conditions of rocuronium. Eur J Anaesthesiol 2002; 19:517–21.
Schmidt J, Irouschek A, Muenster T, Hemmerling TM, Albrecht S. A priming technique accelerates onset of neuromuscular blockade at the laryngeal adductor muscles. Can J Anesth 2005; 52:50–4.
Foldes F. Rapid tracheal intubation with non-depolarizing neuromuscular blocking drugs: the priming principle (Letter). Br J Anaesth 1984; 56:663.
Miller RD. The priming principle. Anesthesiology 1985; 62:381–2.
Abdulatif M, Al-Ghamdi A, El-Sanabary M. Rocuronium priming of atracurium-induced neuromuscular blockade: the use of short priming intervals. J Clin Anesth 1996; 8:376–81.
Foldes FF, Nagashima H, Nguyen HD, Schiller WS, Mason MM, Ohta Y. The neuromuscular effects of ORG9426 in patients receiving balanced anesthesia. Anesthesiology 1991; 75:191–6.
Hofmockel R, Benad G. Time-course of action and intubating conditions with rocuronium bromide under propofol-alfentanil anaesthesia. Eur J Anaesthesiol Suppl 1995; 11:69–72.
Lee SK, Kim JR, Bai SJ, Shin YS, Nam YT, Cohen SP. Effects of priming with pancuronium or rocuronium on intubation with rocuronium in children. Yonsei Med J 1999; 40:327–30.
Loan PB, Paxton LD, Mirakhur RK, Connolly FM, McCoy EP. The TOF-Guard neuromuscular transmission monitor. A comparison with the Myograph 2000. Anaesthesia 1995; 50:699–702.
Viby-Mogensen J, Engaek J, Eriksson LI, et al. Good clinical research practice (GCRP) in pharmacody- namic studies of neuromuscular blocking agents. Acta Anaesthesiol Scand 1996; 40:59–74.
Viby-Mogensen J, Ostergaard D, Donati F, et al. Pharmacokinetic studies of neuromuscular blocking agents: good clinical research practice (GCRP). Acta Anaesthesiol Scand 2000; 44:1169–90.
Kopman AF, Khan NA, Neuman GG. Precurarization and priming: a theoretical analysis of safety and timing. Anesth Analg 2001; 93:1253–6.
Redai I, Feldman SA. Priming studies with rocuronium and vecuronium. Eur J Anaesthesiol Suppl 1995; 11:11–3.
Griffith KE, Joshi GP, Whitman PF, Garg SA. Priming with rocuronium accelerates the onset of neuromuscular blockade. J Clin Anesth 1997; 9:204–7.
Kopman AF, Kumar S, Klewicka MM, Neuman GG. The staircase phenomenon: implications for monitoring of neuromuscular transmission. Anesthesiology 2001; 95:403–7.
Kopman AF, Yee PS, Neuman GG. Relationship of the train-of-four fade ratio to clinical signs and symptoms of residual paralysis in awake volunteers. Anesthesiology 1997; 86:765–71.
Eriksson LI, Sundman E, Olsson R, et al. Functional assessment of the pharynx at rest and during swallowing in partially paralyzed humans: simultaneous videomanometry and mechanomyography of awake human volunteers. Anesthesiology 1997; 87:1035–43.
Author information
Authors and Affiliations
Corresponding author
Additional information
An erratum to this article is available at http://dx.doi.org/10.1007/BF03026811.
Rights and permissions
About this article
Cite this article
Bock, M., Haselmann, L., Böttiger, B.W. et al. Priming with rocuronium accelerates neuromus-cular block in children: a prospective randomized study. Can J Anesth 54, 538–543 (2007). https://doi.org/10.1007/BF03022317
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03022317