
Abstract
Purposes
The aim of this prospective, randomized, doubleblind study was to compare two doses of intranasal sufentanil for postoperative analgesia, titrated according to individual requirements based upon a numeric rating scale (NRS) from 0 to 10 for pain.
Methods
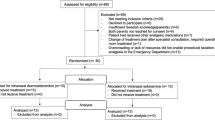
Forty patients, American Society of Anesthesiologists physical status I-II, scheduled for herniorrhaphy or hemorrhoidectomy under general anesthesia, were included when postoperative NRS was > 3. Nurses used a nasal puff device delivering a constant volume. Patients were randomized into two groups: Group A patients received a dose of 0.025 µg·kg-1 /puff, Group B patients a dose of 0.05 µg·kg-1 /puff. Puffs were administered as often as needed to obtain NRS ≤ 3, with an interval time of five minutes. Hemodynamic, respiratory measures and sedation were recorded every five minutes.
Results
The probability of persistence of pain in Group B was consistently lower than in Group A. After 20 min, 20% of the patients had a NRS score > 3 in Group B, as opposed to 60% in Group A. At 60 min, no patient had a NRS > 3 in Group B, whereas there was a probability of 20% to record a NRS > 3 for Group A. Hemodynamic, respiratory parameters and sedation remained stable with no intergroup differences.
Conclusions
Nasal administration of 0.050 µg·kg-1 /puff sufentanil allowed a NRS < 4 to be attained within one hour in all patients, with efficacy achieved after 20 min. These findings suggest that the intranasal route is an effective mode of sufen-tanil administration for immediate postoperative analgesia in adult patients.
Résumé
Objectif
Notre étude prospective, randomisée et à double insu visait à comparer deux doses intranasales de sufentanil comme analgésie postopératoire, ajustées selon les besoins individuels calculés au moyen ďune échelle ďévaluation numérique (EEN) de la douleur de 0 à 10.
Méthode
Quarante patients, ďétat physique ASA I-II, devant subir une herniorraphie ou une hémorroidectomie sous anesthésie générale, ont été inclus quand ľEEN était > 3. Les infirmires ont utilisé un instrument nasal à jet fournissant un volume constant. Les patients ont été répartis en deux groupes: ceux du groupe A ont re÷u une dose de 0,025 µg·kg-1/jet et ceux du groupe B, 0,05 µg·kg-1/jet. Le médicament a été administré aussi souvent que nécessaire pour obtenir une EEN ≤ 3, selon un intervalle de cinq minutes. Les mesures hémodynamiques et respiratoires et la sédation ont été notées toutes les cinq minutes.
Résultats
La probabilité ďune douleur persistante chez les patients du groupe B a été constamment plus basse que chez ceux du groupe A. Aprs 20 min, 20 % avaient un score ďEEN > 3 dans le groupe B, mais 60 % dans le groupe A. A 60 min, aucun patient n’avait une EEN > 3 dans le groupe B, mais il y avait une probabilité de 20 % ďun score ďEEN > 3 dans le groupe A. Les paramètres hémodynamiques et respiratoires et la sédation sont demeurés stables sans différence intergroupe.
Conclusion
Ľadministration nasale de 0,050 µg·kg-1/jet de sufentanil a permis qu’une EEN < 4 soit obtenue en moins ďune heure chez tous les patients et ľefficacité atteinte après 20 min. On peut penser que ľadministration intranasale de sufentanil est un mode efficace pour ľanalgésie postopératoire immédiate chez des adultes.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Dale O, Hjortkjaer R, Kharasch ED. Nasal administration of opioids for pain management in adults. Acta Anaesthesiol Scand 2002; 46: 759–70.
Gillis JC, Benfield P, Goa KL. Transnasal butorphanol. A review of its pharmacodynamic and pharmacokinetic properties, and therapeutic potential in acute pain management. Drugs 1995; 50: 157–75.
Striebel HW, Koenigs D, Kramer J. Postoperative pain management by intranasal demand-adapted fentanyl titration. Anesthesiology 1992; 77: 281–5.
Striebel HW, Pommerening J, Rieger A. Intranasal fentan l titration for postoperative pain management in an unselected population. Anaesthesia 1993; 48: 753–7.
Striebel HW, Oelmann T, Spies C, Rieger A, Schwagmeier R. Patient-controlled intranasal analgesia: a method for noninvasive postoperative pain management. Anesth Analg 1996; 83: 548–51.
Toussaint S, Maidl J, Schagmeier R, Striebel HW. Patient-controlled intranasal analgesia: effective alternative to intravenous PCA for postoperative pain relief. Can J Anesth 2000; 47: 299–302.
Helmers JH, Noorduin H, Van Peer A, Van Leeuwen L, Zuurmond WW. Comparison of intravenous and intranasal sufentanil absorption and sedation. Can J Anaesth 1989; 36: 494–7.
Henderson JM, Brodsky DA, Fisher DM, Brett CM, Hertzka RE. Pre-induction of anesthesia in pediatric patients with nasally administered sufentanil. Anesthesiology 1988; 68: 671–5.
Vercauteren M, Boeckx E, Hannegreefs G, Noorduin H, Vanden Bussche G. Intranasal sufentanil for pre-operative sedation. Anaesthesia 1988; 43: 270–3.
Zedie N, Amory DW, Wagner BK, O’Hara DA. Comparison of intranasal midazolam and sufentanil premedication in pediatric outpatients. Clin Pharmacol Ther 1996; 59: 341–8.
Karl HW, Keifer AT, Rosenberger JL, Larach MG, Ruffle JM. Comparison of the safety and efficacy of intranasal midazolam or sufentanil for preinduction of anesthesia in pediatric patients. Anesthesiology 1992; 76: 209–15.
Mantha S, Thisted R, Foss J, Ellis JE, Roizen M. A proposal to use confidence intervals for visual analog scale data for pain measurement to determine clinical significance. Anesth Analg 1993; 77: 1041–7.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Mathieu, N., Cnudde, N., Engelman, E. et al. Intranasal sufentanil is effective for postoperative analgesia in adults. Can J Anesth 53, 60–66 (2006). https://doi.org/10.1007/BF03021528
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03021528