
Abstract
Background
Procedural sedation and analgesia are commonly used in the Emergency Departments. Despite this common need, there is still a lack of options for adequate and safe analgesia and sedation in children. The objective of this study was to evaluate whether intranasal dexmedetomidine could provide more effective analgesia and sedation during a procedure than intranasal esketamine.
Methods
This was a double-blind equally randomized (1:1) superiority trial of 30 children aged 1–3 years presenting to the Emergency Department with a laceration or a burn and requiring procedural sedation and analgesia. Patients were randomized to receive 2.0 mcg/kg intranasal dexmedetomidine or 1.0 mg/kg intranasal esketamine.
The primary outcome measure was highest pain (assessed using Face, Legs, Activity, Cry, Consolability scale (FLACC)) during the procedure. Secondary outcomes were sedation depth, parents’ satisfaction, and physician’s assessment.
Comparisons were done using Mann–Whitney U test (continuous variables) and Fisher’s test (categorical variables).
Results
Adequate analgesia and sedation were reached in 28/30 patients. The estimated sample size was not reached due to changes in treatment of minor injuries and logistical reasons. The median (IQR) of highest FLACC was 1 (0–3) with intranasal dexmedetomidine and 5 (2–6.75) with intranasal esketamine, (p-value 0.09). 85.7% of the parents with children treated with intranasal dexmedetomidine were “very satisfied” with the procedure and sedation compared to the 46.2% of those with intranasal esketamine, (p-value 0.1). No severe adverse events were reported during this trial.
Conclusions
This study was underpowered and did not show any difference between intranasal dexmedetomidine and intranasal esketamine for procedural sedation and analgesia in young children. However, the results support that intranasal dexmedetomidine could provide effective analgesia and sedation during procedures in young children aged 1–3 years with minor injuries.
Trial registration: Eudra-CT 2017-00057-40, April 20, 2017. https://eudract.ema.europa.eu/
Similar content being viewed by others

Background
The need for pain management and sedation are common in the Emergency Departments (EDs) treating pediatric trauma patients. Every fifth pediatric ED visit is due to trauma [1] and a peak incidence is seen in young children [1, 2]. Their injuries are often classified as minor [3] and can be treated in the ED. As these procedures can be painful and frightening for a child, adequate sedation and analgesia need to be ensured. In addition, the absence of effective procedural sedation and analgesia (PSA) can result in a negative experience for both children and their parents, which in turn can impact future procedures or even hospital visits [4, 5]. Despite the awareness, children still fail to receive adequate PSA due to lack of knowledge and evidence on different possibilities for PSA as reported in recent surveys from Scandinavia and Canada [6, 7].
There are several ways to administer drugs for PSA. Intravenous (IV) administration is widely used. A common risk with IV drugs is deeper sedation than intended, which motivates a sound knowledge of pharmacological effects [8]. The lack of this expertise prevents clinicians from using IV drugs. Another reason for considering alternative delivery routes is the need of an IV-line as cannulation can be difficult and stressful for the child [9]. Intranasal (IN) administration is a non-invasive and easy method and is therefore appealing.
IN esketamine (sKET), an S-enantiomer of ketamine, is routinely used for PSA in Astrid Lindgren Children’s hospital (ALB), but to ensure every child an adequate PSA other options are also needed.
IN dexmedetomidine (DEX) is an interesting alternative as it rarely has clinically significant effects on respiratory or cardiovascular systems [10,11,12,13,14,15,16,17] and causes minimal discomfort when administered [18]. IN DEX has successfully been used as a sedative for non-painful procedures e.g., for imaging [12, 14, 19, 20]. It has been shown to have both a good analgesic effect during IV-cannulation [17] and sedative effect during dental treatment [16]. However, there are limited results for IN DEX in PSA in the ED.
The objective of this study was to evaluate whether IN DEX could provide more effective analgesia and sedation during a painful procedure than IN sKET among young children 1–3 years of age presenting to the ED with minor injuries.
Methods
Trial design
This prospective, equally randomized (1:1), double-blind, parallel group trial was conducted in a large pediatric ED. This study was monitored by an independent regulatory unit, Karolinska Trial Alliance. Ethical approval was obtained from the Regional Ethical Review Board Stockholm. And this study was registered with European Clinical Trial Registry. The trial protocol is presented as Additional file 1.
The CONSORT guidelines [21] were used for reporting our data.
Participants
Inclusion and exclusion criteria
Children 1–3 years old who presented to the ED with a laceration in need of suturing or a burn covering less than 4% of the body surface area and required PSA were eligible for enrolment. Injury was assessed and the need for PSA determined by the ED physician (mainly physicians in training in pediatrics, emergency medicine or general medicine) according to local guidelines. The trial physician was contacted, and the inclusion and exclusion criteria were revised. Patients with American Society of Anesthesiologist physical status classification (ASA) [22] ≥ III, current respiratory tract infection, impaired level of consciousness or any other neurologic symptoms as well as hypersensitivity to the trial drugs were excluded. In addition, children of parents with insufficient understanding of the Swedish language could not be enrolled in this study as written information of the trial was provided in Swedish. Signed informed consent was given by the parents.
Setting and location
This study was conducted in the pediatric ED at Astrid Lindgren Children’s hospital (ALB), Karolinska University Hospital in Stockholm, Sweden. ALB ED has 50 500 annual visits and offers medical care to children and adolescents with all levels of trauma, injuries, and sickness.
Outcomes and definitions
The primary outcome was pain, measured as the highest level of pain during the procedure. Procedure was defined for lacerations as suturing of the wound and for burns as wound debridement and dressing, local guidelines for the procedures were followed. Pain was assessed with Face, Legs, Activity, Cry, Consolability scale (FLACC) [23], which has been validated for procedural pain assessment by Nilsson et al. [24]. FLACC scores were classified as following: 0 = no pain, 1–3 = mild discomfort, 4–6 = moderate pain and 7–10 = severe pain [25, 26]. We considered a change of two points on the FLACC as clinically significant.
Secondary outcomes were sedation depth, parents’ satisfaction, and ED physician’s assessment of the feasibility of the procedure. Ramsay sedation scale [27] was used to evaluate sedation depth, as it is one of the most widely used tools for observationally based sedation assessment and it has been used in studies assessing sedation with intranasal dexmedetomidine [12, 14]. Ramsay score 1 = awake, 2 = awake; co-operative, orientated and tranquil, 3 = awake; responds to commands only 4 = asleep; reacts with a brisk response to a light glabellar tap or a loud auditory stimulus, 5 = asleep; reacts with a sluggish response to a light glabellar tap or a loud auditory stimulus, 6 = asleep; does not respond to pain. We considered a change of one point as clinically significant.
Parent/parents who were with the child from administration of the trial drug until recovery, received a questionnaire with four questions: (1) in your opinion; how much pain did your child have during the procedure on a scale of 0–10 (the revised Faces Pain Scale (FPS-R) [28] was shown to the parents), (2) what was your opinion about the sedation and the procedure on a scale of 1–5 (1 = not satisfied, 5 = very satisfied). (3) if your child needs procedural sedation again in the future, would you prefer the same management? (yes/no), (4) if not what would you wish to be different?
The ED physician graded the feasibility of performing the procedure on a scale of 1–5 (1 = very easy, 5 = very difficult).
Interventions
All patients included in the study received oral paracetamol (40 mg/kg) no later than 1–1.5 h before the procedure.
Patients were enrolled and randomized before the administration of local anesthesia. Buffered lidocaine (10 ml 1% lidocaine + 2 ml NaHCO3 6 M) was used for local anesthesia. The burn area was covered with lidocaine-soaked gauze for 20–30 min before the procedure. Wounds were infiltrated with buffered lidocaine for a minimum of 5 min prior to the procedure. The maximum lidocaine dose without adrenaline was 5 mg/kg and with adrenaline 7 mg/kg.
DEX 100 mcg/ml and sKET 25 mg/ml were used without dilution. A 1 ml syringe with a nasal atomizer was used for drug administration. 2.0 mcg/kg DEX and 1.0 mg/kg sKET were used following the local and national guidelines [29]. The dose was equally divided between both nostrils when the recommended volume per nostril (0.3 ml/nostril) [30] was exceeded.
Patients were monitored from the administration of the trial drug until the patient had recovered, and Ramsay score was 1. Pain (FLACC score) and sedation (Ramsay score) were assessed at least every 5 min before and during the procedure and every 10 min after the procedure. Oxygen saturation (SpO2) and heart rate (HR) were monitored continuously. SpO2 and HR were recorded at the same timepoints with FLACC and Ramsay unless significant changes occurred at other times. Any aberration from normal values described in Pediatric Advanced Life Support (PALS) [31] were considered significant. Assessment and monitoring were done by two experienced pediatricians (AN, KS) who were familiar with both the FLACC and Ramsay scales. Five patients were initially evaluated together to ensure uniform assessment.
The procedure was started when Ramsay score 2 was reached. If it was not reached within 30 min and the child was not co-operative the procedure was not carried through within trial protocol and other sedation was used for the treatment. Patients were able to leave the ED when Ramsay score was 1 and the patient had returned to the habitual condition.
Randomization and blinding
Patients were randomized to two groups: 1) IN DEX 2.0 mcg/kg, 2) IN sKET 1.0 mg/kg. We used block randomization (blocks of 10 subjects (5 from both arms), except one block with 12 subjects). A physician not participating in the trial created a randomization list after a random draw and filled the opaque envelopes with information (trial drug and dose table) and numbered them according to the list. Envelopes were then used in number order. Randomization was kept in a sealed envelope during trial period and the seal was intact at the time of trial closure. The blocks were used in order and the order was not known by the physician performing the assessment of the patient.
The trial physician, ED physician and nurses caring for the patient, as well as the patient and parents were blinded to the trial drug, as were all other staff working in the ED. Trial drug was prepared and administered by a nurse who was not involved in the care of the patient otherwise. Trial physician, ED physician and nurses caring for the patient were not present at the time of drug administration. Patients and their parents did not have knowledge about the trial drugs (e.g., smell or taste, nasal irritation) or the difference between the volume of the two drugs.
Statistical methods
An a priori power analysis was conducted to test the null hypothesis of this superiority trial. We aimed for a mean difference of 2 on FLACC which would be the smallest clinically relevant difference. Assuming a within-group standard deviation of 2.5 we would need n = 26 patient per group to obtain 0.80 power for the test.
Continuous variables are presented using medians and interquartile ranges (IQRs) and tested with Mann–Whitney U test and tested correlations using the Spearman method. Categorical variables are presented using counts and percentages and tested using Fisher’s test. We considered p-values below 0.05 significant. All analyses were done using R version 4.2.2. [32].
Results
Patient enrollment was conducted between July 2017 and October 2019 when one of the two trial physicians was present.
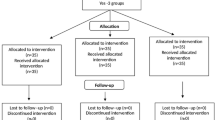
89 patients were assessed for eligibility and 30 patients were randomized, see flow chart (Fig. 1). The groups were similar regarding baseline demographics (Table 1). The estimated sample size was not reached due to changes in treatment of minor injuries and logistical reasons.

Participant flow chart
Adequate analgesia and sedation to complete the procedure was reached in 28/30 patients. One patient in group IN sKET did not reach Ramsay 2 and was not co-operative, hence procedure could not be carried out within the trial protocol. With one patient in group IN DEX the procedure was started but due to high pain reactions (FLACC 9) despite of sedation level of Ramsay 2 the procedure could not be carried out within the trial protocol. The data for each group and comparisons between the groups are summarized in Table 2.
FLACC on all patients before administration of trial drug was 0. The median (IQR) of highest FLACC was 1 (0–3) in group IN DEX and 5 (2–6.75) in group IN sKET, there was no statistical difference between the groups (p-value 0.09). Pain assessment as FLACC is shown in Fig. 2.

Highest pain level during the procedure. Pain level was assessed with Face, Legs, Activity, Cry, Consolability scale (FLACC). This diagram shows the distribution of FLACC scores per drug. The median (IQR) of highest FLACC with patients receiving intranasal dexmedetomidine was 1 (0–3) and in group intranasal esketamine 5 (2–6.75), p-value 0.09
The median (IQR) of Ramsay score was 3 (2–3) with IN DEX and 2 (1–2) with IN sKET, p-value 0.02. Sedation assessment as Ramsay is shown in Fig. 3.

Highest sedation score during the procedure. Sedation level was assessed with Ramsay sedation scale. This diagram shows the distribution of Ramsay scores per drug. The median (IQR) of highest Ramsay with patients receiving intranasal dexmedetomidine was 3 (2–3) and in group intranasal esketamine 2 (1–2), p-value 0.02
Parents’ opinion
One parent in group IN sKET did not wish to answer the questionnaire. The parents of the two patients not receiving sufficient sedation and analgesia with the trial drug only stated they did not wish for the same treatment in the future. 12 (85.7%) of the parents in the group IN DEX were”very satisfied” with the procedure and sedation and 6 (46.2%) in group IN sKET, p-value 0.10. 13/14 of the parents of patients receiving IN DEX and 10 out of 13 parents of patients receiving IN sKET would be satisfied with the same procedural sedation and analgesia if needed in the future. Parents’ assessment of their child’s pain score (FPS-R) median (IQR) was 2.5 (0–5) in group IN DEX and 5 (0–8) in group IN sKET, p-value 0.44.
ED physician’s opinion
The ED physician graded the feasibility of the procedure as 1 = very easy in 8 (57.1%) cases in group IN DEX, whereas 3 (21.4%) cases in group IN sKET were graded 1, p-value 0.21.
Adverse events
No severe adverse events were reported. Two patients in group IN sKET and one in group IN DEX had SpO2 94% very briefly, no drop in HR was noted and no intervening from hospital staff was required. No patients had HR under the 1st age normative percentile.
Discussion
The results of the current study support that IN DEX can provide effective analgesia and sedation during PSA among young children aged 1–3 years with minor injuries, however, it could not be proven to be superior to IN sKET. This lack of significant difference could be explained by the low sample size as a result of not reaching estimated sample size rather than true lack of difference. The estimated sample size was not reached due to changes in treatment of minor injuries and logistical reasons, for details see Limitations below. More parents were satisfied with IN DEX as compared with IN sKET, and these parents would also prefer the same procedural sedation and graded their children’s pain as lower. More procedures were graded as very easy by ED physicians when IN DEX was used as compared with IN sKET.
In our study patients receiving IN DEX had generally lower pain scores during the procedure than those in IN sKET group. Three quarters of the patients receiving IN DEX had no pain or only mild discomfort whereas in the IN sKET group, the majority had moderate to severe pain during the procedure. Two studies [16, 17] have analyzed pain level during PSA, and their results support the findings in our study.
The lack of evidence may have prevented physicians from considering IN DEX as an option for PSA for painful procedures in the ED [7]. In addition, the lack of alternatives may have contributed to the use of physical restraints [6]. We believe that despite incomplete inclusion, and therefore not reaching calculated sample size, these results show clinically relevant information in relation to IN DEX analgesic and sedative effect during painful procedures in young children.
Deeper sedation (Ramsay ≥ 3) was reached more often with IN DEX than IN sKET. Deeper sedation typically has been shown to provide better circumstances for the procedure which, in turn, often contributes to better outcome. In our study ED physicians graded the procedure very easy to perform more often with patients who had received IN DEX than IN sKET. Neville et al. [33] showed the superiority of IN DEX to IN midazolam as an anxiolytic prior to laceration repair in young children. The sedative effect of IN DEX during non-painful procedures has been reported in previous studies [12, 14, 19, 20] and during dental treatment [16]. Results from these studies support the current results that IN DEX provides a deeper sedation and is safe to use.
Parents’ opinion about the PSA is important as their experience and satisfaction can affect a child’s anxiety and fear [34]. In our study, parents to children treated with IN DEX graded their general opinion of the management of the procedure and sedation as the category “very satisfied” more often than was the case in the IN sKET group, although statistical significance was not shown. Parents in group IN DEX also estimated their child’s pain during the procedure to be lower than in group IN sKET. These results are encouraging for the use of IN DEX for PSA in the ED for young children, although further study is required to confirm these results.
Besides providing safe and good PSA, good circumstances to perform a procedure is essential for an ED physician. In our study ED physicians graded the feasibility of performing the procedure very easy more often with patients receiving IN DEX than IN sKET.
We did not see any significant effects on the respiratory or cardiovascular systems in either patient group, but a conclusion of the safety of the drugs cannot be assessed with this small sample size. Adverse events of IN DEX are reported in many studies although no clinically significant changes on systolic blood pressure, HR, respiratory rate or SpO2 has been seen with the use of IN DEX [11,12,13,14,15, 35]. These results support that IN DEX is safe to use for PSA in the ED with adequate monitoring.
Limitations
The main limitation of this study is not reaching the power needed to show statistical significance. We did not reach the estimated sample size during the study period of two years even though this study was conducted in a large pediatric ED. There are several explanations for this. During the study period there was a change in the streaming protocol for children with minor injuries in the region due to the opening of a number of low-acuity emergency care centers in Stockholm treating children with minor injuries which resulted in fewer patients attending the ALB ED, reducing the number of eligible patients for our study. Furthermore, the topical lidocaine, adrenaline, tetracaine gel and tissue glue changed the treatment practice for laceration repair and therefore procedural sedation was needed less frequently. Moreover, the study team could not be expanded as the Karolinska Trial alliance strongly recommended physicians to perform the patient assessment during the trial. Hence the study was required to be done by physicians, which in turn was a limiting factor as there are few experienced pediatric emergency physicians available both at ALB and other centers. Continued enrollment during 2020 was initially planned but could not be executed due to the Covid-19 pandemic. In addition, we could potentially have reached sample size if study drugs were administered in two doses, this would have allowed children weighing more than 15 kg to be enrolled.
There were two trial physicians doing all the assessments, which can be seen as both a strength and a limitation. A strength, as this reduces the variability in the FLACC and Ramsay scores. On the other hand, this obviously can have affected the number of patients enrolled as the trial physicians could not be present at all times.
The dosage of sedative drugs used in this study can be discussed. For IN sKET we followed the national guidelines from the Swedish Medical Product Agency regarding procedural sedation and analgesia for children [29]. The recommended dose for IN sKET is 1.0 mg/kg in children and with a maximum weight of 15 kg as otherwise the intranasal volume would become too large for good absorption from the nasal mucosa. 23 children were excluded from this study as they weighed more than 15 kg. This could have been avoided by administering the drugs twice with a specific time interval. However, we chose to follow the Swedish guidelines. Before 2017 most of the studies on IN DEX were done with the maximum dose of 2.0 mcg/kg [13, 33]. In addition, the local guidelines and the experience from IN DEX for imaging in ALB impacted our choice of the dose. In 2023 Poonai et al. suggested that 3 or 4 mcg/kg could be considered as an optimal dose of IN DEX in laceration repair [36].
Generalisability
This trial was limited to the age group 1–3 years. Lacerations and burns are common minor injury types in this age group and were therefore selected for this trial. Unfortunately, all patients with burns received IN DEX for trial drug as a follow to the random allocation. These limitations need to be taken into consideration when treating children in other age groups and different procedures requiring analgesia and sedation are in question.
Conclusion
This study was underpowered and did not show any difference between intranasal dexmedetomidine and intranasal esketamine for procedural sedation and analgesia in young children. However, the results support that intranasal dexmedetomidine could provide effective analgesia and sedation during procedures in young children aged 1–3 years with minor injuries.
Availability of data and materials
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- ALB:
-
Astrid Lindgren Children’s Hospital
- ASA:
-
Anesthesiologist physical status classification
- DEX:
-
Dexmedetomidine
- ED:
-
Emergency Department
- FLACC:
-
Face, Legs, Activity, Cry, Consolability scale
- FPS-R:
-
Revised Faces Pain Scale
- HR:
-
Heart rate
- IN:
-
Intranasal
- IQR:
-
Interquartile range
- IV:
-
Intravenous
- sKET:
-
Esketamine
- PALS:
-
Pediatric Advanced Life Support
- PSA:
-
Procedural sedation and analgesia
- SpO2 :
-
Oxygen saturation
References
Lee LK, Porter JJ, Mannix R, Rees CA, Schutzman SA, Fleegler EW, et al. Pediatric traumatic injury emergency department visits and management in US children’s hospitals From 2010 to 2019. Ann Emerg Med. 2022;79(3):279–87.
Cintean R, Eickhoff A, Zieger J, Gebhard F, Schütze K. Epidemiology, patterns, and mechanisms of pediatric trauma: a review of 12,508 patients. Eur J Trauma Emerg Surg. 2023;49(1):451–9.
Voth M, Lustenberger T, Auner B, Frank J, Marzi I. What injuries should we expect in the emergency room? Injury. 2017;48(10):2119–24.
Weisman SJ, Bernstein B, Schechter NL. Consequences of inadequate analgesia during painful procedures in children. Arch Pediatr Adolesc Med. 1998;152(2):147–9.
Noel M, Chambers CT, McGrath PJ, Klein RM, Stewart SH. The influence of children’s pain memories on subsequent pain experience. Pain. 2012;153(8):1563–72.
Aaberg Lauridsen J, Lefort Sønderskov M, Hetmann F, Hamilton A, Salmi H, Wildgaard K. Investigating the use of physical restraint of children in emergency departments: a Scandinavian survey. Acta Anaesthesiol Scand. 2021;65(8):1116–21.
Kumar K, Ali S, Sabhaney V, Trottier E, Drendel A, Bhatt M, et al. Anxiolysis for laceration repair in children: a survey of pediatric emergency providers in Canada. CJEM. 2022;24(1):75–83.
Coté CJ, Wilson S. Guidelines for monitoring and management of pediatric patients before, during, and after sedation for diagnostic and therapeutic procedures. Pediatrics. 2019;143(6): e20191000.
Humphrey GB, Boon CM, van Linden van den Heuvell GF, van de Wiel HB. The occurrence of high levels of acute behavioral distress in children and adolescents undergoing routine venipunctures. Pediatrics. 1992;90(1):87–91.
Yuen VM, Hui TW, Irwin MG, Yuen MK. A comparison of intranasal dexmedetomidine and oral midazolam for premedication in pediatric anesthesia: a double-blinded randomized controlled trial. Anesth Analg. 2008;106(6):1715–21.
Akin A, Bayram A, Esmaoglu A, Tosun Z, Aksu R, Altuntas R, et al. Dexmedetomidine vs midazolam for premedication of pediatric patients undergoing anesthesia. Paediatr Anaesth. 2012;22(9):871–6.
Mekitarian Filho E, Robinson F, de Carvalho WB, Gilio AE, Mason KP. Intranasal dexmedetomidine for sedation for pediatric computed tomography imaging. J Pediatr. 2015;166(5):1313-5.e1.
Yuen VM, Hui TW, Irwin MG, Yao TJ, Chan L, Wong GL, et al. A randomised comparison of two intranasal dexmedetomidine doses for premedication in children. Anaesthesia. 2012;67(11):1210–6.
Tug A, Hanci A, Turk HS, Aybey F, Isil CT, Sayin P, et al. Comparison of two different intranasal doses of dexmedetomidine in children for magnetic resonance imaging sedation. Paediatr Drugs. 2015;17(6):479–85.
Cimen ZS, Hanci A, Sivrikaya GU, Kilinc LT, Erol MK. Comparison of buccal and nasal dexmedetomidine premedication for pediatric patients. Paediatr Anaesth. 2013;23(2):134–8.
Surendar MN, Pandey RK, Saksena AK, Kumar R, Chandra G. A comparative evaluation of intranasal dexmedetomidine, midazolam and ketamine for their sedative and analgesic properties: a triple blind randomized study. J Clin Pediatr Dent. 2014;38(3):255–61.
Xie Z, Shen W, Lin J, Xiao L, Liao M, Gan X. Sedation effects of intranasal dexmedetomidine delivered as sprays versus drops on pediatric response to venous cannulation. Am J Emerg Med. 2017;35(8):1126–30.
Yuen VM, Irwin MG, Hui TW, Yuen MK, Lee LH. A double-blind, crossover assessment of the sedative and analgesic effects of intranasal dexmedetomidine. Anesth Analg. 2007;105(2):374–80.
Li BL, Ni J, Huang JX, Zhang N, Song XR, Yuen VM. Intranasal dexmedetomidine for sedation in children undergoing transthoracic echocardiography study–a prospective observational study. Paediatr Anaesth. 2015;25(9):891–6.
Cao Q, Lin Y, Xie Z, Shen W, Chen Y, Gan X, et al. Comparison of sedation by intranasal dexmedetomidine and oral chloral hydrate for pediatric ophthalmic examination. Paediatr Anaesth. 2017;27(6):629–36.
Schulz KF, Altman DG, Moher D. CONSORT 2010 Statement: updated guidelines for reporting parallel group randomised trials. BMC Med. 2010;8(1):18.
https://www.asahq.org/standards-and-practice-parameters/statement-on-asa-physical-status-classification-system Developed By: Committee on Economics, American Society of Anesthesiologists Last Amended: December 13, 2020 (original approval: October 15, 2014)
Merkel SI, Voepel-Lewis T, Shayevitz JR, Malviya S. The FLACC: a behavioral scale for scoring postoperative pain in young children. Pediatr Nurs. 1997;23(3):293–7.
Nilsson S, Finnstrom B, Kokinsky E. The FLACC behavioral scale for procedural pain assessment in children aged 5–16 years. Paediatr Anaesth. 2008;18(8):767–74.
Uitti JM, Salanterä S, Laine MK, Tähtinen PA, Ruohola A. Adaptation of pain scales for parent observation: are pain scales and symptoms useful in detecting pain of young children with the suspicion of acute otitis media? BMC Pediatr. 2018;18(1):392.
Malviya S, Voepel-Lewis T, Burke C, Merkel S, Tait AR. The revised FLACC observational pain tool: improved reliability and validity for pain assessment in children with cognitive impairment. Paediatr Anaesth. 2006;16(3):258–65.
Ramsay MA, Savege TM, Simpson BR, Goodwin R. Controlled sedation with alphaxalone-alphadolone. Br Med J. 1974;2(5920):656–9.
Hicks CL, von Baeyer CL, Spafford PA, van Korlaar I, Goodenough B. The Faces Pain Scale-Revised: toward a common metric in pediatric pain measurement. Pain. 2001;93(2):173–83.
Behandling av barn i samband med smärtsamma procedurer i hälso- och sjukvård Kunskapsdokument Information från Läkemedelsverket 3:2014. https://www.lakemedelsverket.se/48dcfa/globalassets/dokument/behandling-och-forskrivning/behandlingsrekommendationer/behandlingsrekommendation/kunskapsdokument---behandling-av-barn-i-samband-med-smartsamma-procedurer.pdf.
Miller JW, Balyan R, Dong M, Mahmoud M, Lam JE, Pratap JN, et al. Does intranasal dexmedetomidine provide adequate plasma concentrations for sedation in children: a pharmacokinetic study. Br J Anaesth. 2018;120(5):1056–65.
Normal values in children. https://www.aclsmedicaltraining.com/normal-values-in-children
R Core Team (2022). R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. URL https://www.R-project.org/.
Neville DN, Hayes KR, Ivan Y, McDowell ER, Pitetti RD. Double-blind randomized controlled trial of intranasal dexmedetomidine versus intranasal midazolam as anxiolysis prior to pediatric laceration repair in the emergency department. Acad Emerg Med. 2016;23(8):910–7.
Bearden DJ, Feinstein A, Cohen LL. The influence of parent preprocedural anxiety on child procedural pain: mediation by child procedural anxiety. J Pediatr Psychol. 2012;37(6):680–6.
Lei H, Chao L, Miao T, Ya Jun L, Shen Ling L, Yan Ying P, et al. Incidence and risk factors of bradycardia in pediatric patients undergoing intranasal dexmedetomidine sedation. Acta Anaesthesiol Scand. 2020;64(4):464–71.
Poonai N, Sabhaney V, Ali S, Stevens H, Bhatt M, Trottier ED, et al. Optimal Dose of Intranasal Dexmedetomidine for Laceration Repair in Children: A Phase II Dose-Ranging Study. Ann Emerg Med. 2023.
Acknowledgements
We would like to thank the staff at Astrid Lindgren Children’s hospital Emergency Department for their help in patient recruitment and for providing PSA for the patients.
Funding
Open Access funding provided by University of Helsinki (including Helsinki University Central Hospital). Personal research funding for doctoral research from Päivikki and Sakari Sohlberg Foundation, Stiftelsen Samariten, Finska läkaresällskapet. The funding bodies did not have any role in the design of the study, data collection, analysis, interpretation or writing of the manuscript. Open Access funding provided by Helsinki University.
Author information
Authors and Affiliations
Contributions
AN has made substantial contributions to the conception and design of the work, data collection, analysis and interpretation of data, was the principal author of the text and has prepared the manuscript. SL has participated in drafting the work and interpretation of data and has substantially revised it on several occasions. MR-R has participated in drafting the work and interpretation of data and has substantially revised it on several occasions. ML carried out the statistical analysis and made substantial contribution to the statistical part of the manuscript inclusive preparing the figures. KS made substantial contribution in the data collection and revised the manuscript. MC contributed and critically revised the manuscript. LK has made substantial contributions to the conception and design of the work, the interpretation of the results and continuously revised the work as the principal supervisor. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Swedish Ethical Review Authority (2017/824–31/1). Informed consent was provided by both parents of every child enrolled in this trial.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Clinical trial protocol.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Nikula, A., Lundeberg, S., Ryd Rinder, M. et al. A randomized double-blind trial of intranasal dexmedetomidine versus intranasal esketamine for procedural sedation and analgesia in young children. Scand J Trauma Resusc Emerg Med 32, 16 (2024). https://doi.org/10.1186/s13049-024-01190-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13049-024-01190-5