
Abstract
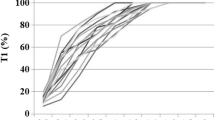
Recovery after doxacurium and pancuronium neuromuscular blockade and their acceleration by neostigmine have not been compared in children. Therefore, 60 paediatric surgical patients aged 2–10 yr (ASA 1–2) were studied. They were randomized to receive doxacurium 30 μg · kg−1 or pancuronium 70 μg · kg−1 iv during propofol, fentanyl, isoflurane and nitrous oxide anaesthesia. Electromyographic (EMG) responses of the adductor pollicis to train-of-four (TOF) stimulation of the ulnar nerve were recorded every ten seconds using a Datex NMT monitor. Six patients in each relaxant group received neostigmine (0, 5, 10, 20 or 40 μg · kg−1) with atropine by random allocation when first twitch height (TI) had recovered to 25% of control. Spontaneous recovery after ten minutes was similar following doxacurium (mean ± SEM values of 45.0 ± 3.9 vs 49.5 ± 10.0 % for TI and 25.2 ± 3.8 vs 14.8 ± 3.6% for TOF ratios). Dose-responses to neostigmine were calculated from the log dose vs logit of TI or TOF ratio after ten minutes. Neostigmine-assisted recovery was not different in the two groups, with ED70 and ED90 doses for TI of 14.3 ± 1.8 and 25.7 ± 2.7 μg·kg−1 for doxacurium and 12.5 ± 1.7 and 25.3 ± 2.3 μg· kg−1 for pancuronium. Time to recovery of TOF ratio to 70% after neostigmine 40 ng · kg−1 was 2.3 ± 1.0 and 4.2 ± 1.7 min (P = NS) following pancuronium and doxacurium, respectively. Adjusted recovery due to neostigmine alone (spontaneous recovery subtracted from the total) required two to three times higher doses of neostigmine. Thus, in children, the spontaneous recovery and reversal of neuromuscular blockade is similar with doxacurium and pancuronium. However, compared with previous adult studies, they recover twice as quickly from doxacurium neuromuscular blockade and neostigmine antagonism is achieved at 25–50% of the adult doses.
Résumé
On n’a jamais comparé chez l’enfant l’antagonisme du bloc neuromusculaire produit par le doxacurium avec celui du pancuronium et son accélération par la néostigmine. Dans ce but, 60 patients pédiatriques programmés pour la chirurgie sont étudiés. Ils sont répartis au hasard pour recevoir soit du doxacurium 30 μg · kg−1 ou du pancuronium 70 μg · kg−1 pendant une anesthésie générale au propofol, fentanyl, isoflurane et protoxyde d’azote. La réponse électromyographique à la stimulation par train de quatre (TOF) du nerf cubital est enregistrée toutes les dix secondes sur un moniteur NMT de Datex. Six patients dans chacun des groupes reçoivent néostigmine (0, 5, 10, 20 ou 40) avec de l’atropine au moment du retour de l’amplitude de la première secousse (TI) à 25% du contrôle. Après dix minutes, la décurarisation spontanée est identique après le doxacurium (moyenne ± SEM, 45.0 ± 3,9 vs 49,5 ± 10,0% pour le TI et 25,2 ± 3,8 vs 14,8 ± 3,6% pour le rapport TOF). Les relations dose-effet de la néostigmine sont calculées avec le log de la dose vs le logit de TI ou la rapport TOF après dix minutes. Avec des ED70 et ED90, la décurarisation assistée par la néostigmine ne diffère pas entre les deux groupes au regard du TI: de 14,3 ± 1,8 et 25,7 ± 2,7 μg · kg−1 pour le doxacurium et de 12,5 ± 1,7 et 25,3 ± 2,3 μg · kg−1 pour le pancuronium. Le délai de retour du rapport TOF à 70% après néostigmine 40 μg · kg−1 est de 2,3 ± 1,0 après le pancuronium et de 4,2 ± 1,7 min (P = NS) après le doxacurium. La décurarisation ajustée pour la néostigmine seule (la décurarisation spontanée soustraite du total) nécessite des doses de deux à trois fois plus importantes de néostigmine. Chez l’enfant, la décurarisation spontanée et l’antagonisme du bloc neuromusculaire sont identiques pour le doxacurium et le pancuronium. Cependant, comparativement aux adultes, les enfants récupèrent deux fois plus rapidement du bloc neuromusculaire produit par le doxacurium et l’antagonisme de la néostigmine est complet à doses de 25–50% inférieures à celles de l’adulte.
Article PDF
Similar content being viewed by others

Avoid common mistakes on your manuscript.
References
Bevan DR, Bevan JC, Donati F. Muscle Relaxants in Clinical Anesthesia. Chicago, London, Boca Raton: Year Book Medical Publishers, Inc. 1988; 345–88.
Cook DR. Muscle relaxants in infants and children. Anesth Analg 1981; 60: 335–43.
Fisher DM, Cronnelly R, Miller RD, Sharma M. The neuromuscular pharmacology of neostigmine in infants and children. Anesthesiology 1983; 59: 220–5.
Meakin G, Sweet PT, Bevan JC, Bevan DR. Neostigmine and edrophonium as antagonists of pancuronium in infants and children. Anesthesiology 1983; 59: 316–21.
Scott RPF, Norman J. Doxacurium chloride: a preliminary clinical trial. Br J Anaesth 1989; 62: 373–7.
Lennon RL, Hosking MP, Houck PC, et al. Doxacurium chloride for neuromuscular blockade before tracheal intubation and surgery during nitrous oxide-oxygen-narcotic-enflurane anesthesia. Anesth Analg 1989; 68: 255–60.
Katz JA, Fragen RJ, Shanks CA, Dunn K, McNulty B, Rudd GD. Dose-response relationships of doxacurium chloride in humans during anesthesia with nitrous oxide and fentanyl, enflurane, isoflurane, or halothane. Anesthesiology 1989; 70: 432–6.
Maddineni VR, Cooper R, Stanley JC, Mirakhur RK, Clarke RSJ. Clinical evaluation of doxacurium chloride. Anaesthesia 1992; 47: 554–7.
Dresner DL, Basta SJ, Ali HH, et al. Pharmacokinetics and pharmacodynamics of doxacurium in young and elderly patients during isoflurane anesthesia. Anesth Analg 1990; 71: 498–502.
Koscielniak-Nielsen ZJ, Law-Min JC, Donati F, Bevan DR, Clement P, Wise R. Dose-response relations of doxacurium and its reversal with neostigmine in young adults and healthy elderly patients. Anesth Analg 1992; 74: 845–50.
Sarner JB, Brandom BW, Cook DR, et al. Clinical pharmacology of doxacurium chloride (BW A938U) in children. Anesth Analg 1988; 67: 303–6.
Goudsouzian NG, Alifimoff JK, Liu LMP, Foster V, McNulty B, Savarese JJ. Neuromuscular and cardiovascular effects of doxacurium in children anaesthetized with halothane. Br J Anaesth 1989; 62: 263–8.
Goudsouzian NG, Ryan JF, Savarese JJ. The neuromuscular effects of pancuronium in infants and children. Anesthesiology 1974; 41: 95–8.
Blinn A, Woelfel SK, Cook DR, Brandom BW, Cohen IT. Pancuronium dose-response revisited. Paediatric Anaesthesia 1992; 2: 153–5.
Goudsouzian NG, Martyn JJA, Liu LMP, Ali HH. The dose resonse effect of long-acting nondepolarizing neuromuscular blocking agents in children. Can J Anaesth 1984; 31:246–50.
Carter JA, Arnold R, Yate PM, Flynn PJ. Assessment of the Datex Relaxograph during anaesthesia and atracuriuminduced neuromuscular blockade. Br J Anaesth 1986; 58: 1447–52.
Meretoja OA, Werner MU, Wirtavuori K, Luosto T. Comparison of thumb acceleration and thenar EMG in a pharmacodynamic study of alcuronium. Acta Anaesthesiol Scand 1989; 33: 545–8.
Eriksson LI, Lennmarken C, Jensen E, Viby-Mogensen J. Twitch tension and train-of-four ratio during prolonged neuromuscular monitoring at different peripheral temperatures. Acta Anaesthesiol Scand 1991; 35: 247–52.
Heier T, Caldwell JE, Eriksson LI, Sessler DI, Miller RD. The effect of hypothermia on adductor pollicis twitch tension during continuous infusion of vecuronium in isoflurane-anesthetized humans. Anesth Analg 1994; 78: 312–7.
Engbaek J, Skovgaard LT, Friis B, Kann T, Viby-Mogensen J. Monitoring of the neuromuscular transmission by electromyography (I). Stability and temperature dependence of evoked EMG response compared to mechanical twitch recordings in the cat. Acta Anaesthesiol Scand 1992; 36: 495–504.
Engbaek J, Skovgaard LT, Fries B, Kann T, Viby-Mogensen J. Monitoring of neuromuscular transmission by electromyography (II). Evoked compound EMG area, amplitude and duration compared to mechanical twitch recording during onset and recovery of pancuronium-induced blockade in the cat. Acta Anaesthesiol Scand 1993; 37: 788–98.
Beemer GH, Bjorksten AR, Dawson PJ, Dawson RJ, Heenan PJ, Robertson BA. Determinants of the reversal time of competitive neuromuscular block by anticholinesterases. Br J Anaesth 1991; 66: 469–75.
Goldhill DR, Embree PB, Ali HH, Savarese JJ. Reversal of pancuronium. Neuromuscular and cardiovascular effects of a mixture of neostigmine and glycopyrronium. Anaesthesia 1988; 43: 443–6.
Bartkowski RR. Incomplete reversal of pancuronium neuromuscular blockade by neostigmine, pyridostigmine, and edrophonium. Anesth Analg 1987; 66: 594–8.
Donati F, Lahoud J, McCready D, Bevan DR. Neostigmine, pyridostigmine and edrophonium as antagonists of deep pancuronium blockade. Can J Anaesth 1987; 34: 589–93.
Delisle S, Bevan DR. Impaired neostigmine antagonism of pancuronium during enflurane anaesthesia in man. Br J Anaesth 1982; 54: 441–5.
Meistelman C, Debaene B, d’Hollander A, Donati F, Saint-Maurice C. Importance of the level of paralysis recovery for a rapid antagonism of vecuronium with neostigmine in children during halothane anesthesia. Anesthesiology 1988; 69: 97–9.
Donati F, McCarroll SM, Antzaka C, McCready D, Bevan DR. Dose-response curves for edrophonium, neostigmine, and pyridostigmine after pancuronium and d-tubocurarine. Anesthesiology 1987; 66: 471–6.
Donati F, Smith CE, Bevan DR. Dose-response relationships for edrophonium and neostigmine as antagonists of moderate and profound atracurium blockade. Anesth Analg 1989; 68: 13–9.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Bevan, J.C., Purday, J.P., Reimer, E.J. et al. Reversal of doxacurium and pancuronium neuromuscular blockade with neostigmine in children. Can J Anaesth 41, 1074–1080 (1994). https://doi.org/10.1007/BF03015657
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03015657