
Abstract
Purpose
To determine the hemodynamic responses to, and the efficacy of epinephrine-containing epidural test doses, during sevoflurane anesthesia, based on the conventional heart rate (HR) increase ≥20 beats·min−1, the modified HR increase if ≥ 10 beats·min−1, and the systolic blood pressure (SBP) increase 15 mmHg criteria.
Methods
One hundred and twenty patients were randomised to receive sevoflurane 0.5, 1 or 2% end-tidal (n = 40 each) and nitrous oxide 67% in oxygen aftertracheal intubation. Each group of patients was further divided into groups receiving 3 ml lidocaine 1.5% plus 15 μg epinephrine (1:200,000) iv, or 3 ml normal saline (n = 20 each). The HR and SBP were monitored for four minutes after injection of the study drug.
Results
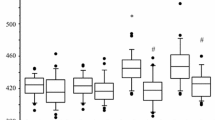
Intravenous injection of the test dose produced HR increases ≥20 beats·min−1 in 18 (90%), 16 (80%) and 14 (70%) patients at sevoflurane concentrations at 0.5, 1 and 2%, respectively, while those receiving saline developed no HR changes. Based on the modified HR criterion, sensitivity, specificity, and positive and negative predictive values were all 100% under sevoflurane concentrations of 0.5 and 1%, but not 2%. On the other hand, all patients in the test dose groups and none in the saline groups developed SBP ≥ 15 mmHg, ensuring 100% efficacy based on the conventional SBP criterion under all sevoflurane concentrations studied. In all patients receiving the intravenous test dose, peak HR occurred 30–45 sec earlier than that of SBP.
Conclusion
During stable sevoflurane anesthesia, peak HR increase ≥ 10 beats·min−1 should be regarded as a positive response with end-tidal sevoflurane concentration ≤ 1%, and peak SBP increase ≥ 15 mmHg is applicable at sevoflurane concentrations between 0.5 and 2%.
Résumé
Objectif
Déterminer les réponses hémodynamiques à des doses tests péridurales contenant de l’épinéphrine et en vérifier l’efficacité pendant l’anesthésie au sévoflurane. Les essais sont basés sur l’augmentation habituelle de la fréquence cardiaque(FC)> 20 battements·min−1, l’augmentation modifiée de la FC si > 10 battements·min−1 et le critère d’accroissement > 15 mmHg de la tension artérielle systolique (TAS).
Méthode
Cent vingt patients ont été répartis au hasard et ont reçu du sévoflurane 0,5, 1 ou 2 % (fin d’expiration) (n = 40 dans chaque groupe) et un mélange de protoxyde d’azote, à 67 %, et d’oxygène après l’intubation endotrachéale. Chaque groupe a ensuite été divisé en sous-groupes à qui on a administré 3 ml de lidocaïne 1,5 % et 15μg d’épinéphrine (1:200 000)iv, ou 3 ml de solution salée (n = 20 chacun). La FC et la TAS ont été surveillées pendant quatre minutes après l’injection du médicament étudié.
Résultats
L’injection intraveineuse de la dose test a produit une augmentation de la FC> 20 battements-min−1 chez 18 (90 %), 16 (80 %) et 14 (70 %) patients pour des concentrations de sévoflurane de 0 5, 1 et 2 %, respectivement, tandis que ceux qui ont reçu une solution salée n’ont pas subi de changement de FC. Sur la base du criète modifié de FC, la sensibilité, la spécificité et les valeurs prédictives positives et négatives ont été de 100 % avec les concentrations de sévoflurane de 0,5 % et de 1 % mais non avec la concentration de 2 %. Par ailleurs, tous les patients qui ont reçu des doses tests ont développé une TAS > 15 mmHg, contrairement aux patients qui ont reçu une solution salée, ce qui assure 100 % d’efficacité, basée sur le critère habituel de TAS, de toutes les concentrations de sévoflurane étudiées. Chez tous les patients qui ont reçu des doses tests intraveineuses, on a enregistré la FC maximale 30–45 s plus tôt que celle de la TAS.
Conclusion
Pendant une anesthésie stable au sévoflurane, l’accroissement de la FC > 10 battements·min−1 devrait être considéré comme une réaction positive avec des concentrations de sévoflurane de fin d’expiration I %, et l’accroissement de TAS maximale > 15 mmHg se manifeste à des concentrations de sévoflurane entre 0,5 et 2 %.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Liu S, Carpenter RL, Neal JM. Epidural anesthesia and analgesia. Their role in postoperative outcome. Anesthesiology 1995; 82: 1474–506.
Marx GF. Cardiotoxicity of local anesthetics — the plot thickens (Editorial). Anesthesiology 1984; 60: 3–5.
Matsumiya N, Dohi S, Takahashi H, Kondo Y, Naito H. Cardiovascular collapse in an infant after caudal anesthesia with a lidocaine-epinephrine solution. Anesth Analg 1986; 65: 1074–6.
Guinard J-P, Mulroy MF, Carpenter RL, Knopes KD. Test doses: optimal epinephrine content with and without acute beta-adrenergic blockade. Anesthesiology 1990; 73: 386–92.
Tanaka M, Takahashi S, Kondo T, Matsumiya N. Efficacy of simulated epidural test doses in adult patients anesthetized with isoflurane: a dose-response study. Anesth Analg 1995; 81: 987–92.
Donchin Y, Feld JM, Forges SW. Respiratory sinus arrhythmia during recovery from isoflurane-nitrous oxide anesthesia. Anesth Analg 1985; 64: 811–5.
Ware PD, Liu SS. Efficacy of epidural test doses (Letter). Anesth Analg 1996; 82: 1304–5.
Stowe DF, Dujic Z, Bosnjak ZJ, Kalbfleisch JH, Kampine JP. Volatile anesthetics attenuate sympathomimetic actions on the guinea pig SA node. Anesthesiology 1988; 68: 887–94.
Lerman J, Sikich N, Kleinman S, Yentis S. The pharmacology of sevoflurane in infants and children. Anesthesiology 1994; 80: 814–24.
Yasuda N, Targ AG, Eger EI II. Solubility of 1-653, sevoflurane, isoflurane and halothane in human tissues. Anesth Analg 1989; 69: 370–3.
Sanuki M, Yuge O, Kawamoto M, Fujii K, Azuma T. Sevoflurane inhibited ß-adrenoceptor-G protein bindings in myocardial membrane in rats. Anesth Analg 1994; 79: 466–71.
Weigt HU, Kwok W-M, Rehmert GC, Turner LA, Bosnjak ZJ. Voltage-dependent effects of volatile anesthetics on cardiac sodium current Anesth Analg 1997; 84: 285–93.
Tanaka M. Epidural test dose: isoproterenol is a reliable marker for intravascular injection in anesthetized adults. Anesth Analg 1996; 82: 1056–9.
Tanaka M. Simulation of an epidural test dose with intravenous isoproterenol in isoflurane-anesthetized adults. Anesth Analg 1997; 85: 639–43.
Leighton BL, Norris MC, DeSimone CA, Rosko T, Gross JB. The air test as a clinically useful indicator of intravenously placed epidural catheters. Anesthesiology 1990; 73: 610–3.
Valley MA, McKenzie AM, Bourke DL, Raja SN. Effects of epidural test dose volume on skin perfusion, temperature, and reflex vasoconstriction. Reg Anesth 1994; 19: 52–8.
Hijzen TH, Slangen JL. The electrocardiogram during emotional and physical stress. Int J Psychophysiol 1985; 2: 273–9.
Fisher QA, Shaffner DH, Yaster M. Detection of intravascular injection of regional anaesthetics in children. Can J Anaesth 1997; 44: 592–8.
Kubota T, Toyoda Y, Kubota H, Asada A. Epinephrine in local anesthetics does indeed produce hypokalemia and ECG changes (Letter). Anesth Analg 1993; 77: 867.
Liu SS. Hemodynamic responses to an epinephrine test dose in adults during epidural or combined epiduralgeneral anesthesia. Anesth Analg 1996; 83: 97–101.
Gieraerts R, Van Zundert A, De Wolf A, Vaes L. Ten ml bupivacaine 0.125% with 12.5 μg epinephrine is a reliable epidural test dose to detect inadvertent intravascular injection in obstetric patients. A double-blind study. Acta Anaesthesiol Scand 1992; 36: 656–9.
Borow KM, Newburger JW. Noninvasive estimation of central aortic pressure using the oscillometric method for analyzing systemic artery pulsatile blood flow: comparative study of indirect systolic, diastolic, and mean brachial artery pressure with simultaneous direct ascending aortic pressure measurements. Am Heart J 1982; 103: 879–86.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Takahashi, S., Tanaka, M. Reduced efficacy of simulated epidural test doses in sevoflurane-anesthetized adults. Can J Anesth 46, 433–438 (1999). https://doi.org/10.1007/BF03012942
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03012942