
Abstract
Purpose
To highlight the need for referral and prompt intervention when signs of increased intraorbital pressure are present.
Clinical features
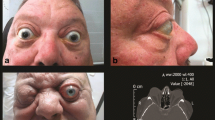
A four year old child presented to hospital with orbital swelling of recent onset, nausea and somnolence. Computed tomography and brain scan demonstrated a normal brain with a mass in the left orbit. She was referred for ophthalmic surgery the following day, when she had lost responsiveness of her left pupil to light. Anaesthetic management was highlighted by the presence of preoperative signs and symptoms of increased intraocular pressure — somnolence, nausea and vomiting, and bradycardia. These signs and symptoms were alleviated postoperatively.
Conclusion
Rapid onset of orbital swelling with physiological signs of increased orbital pressure necessitate urgent surgical intervention. It is possible that early referral and surgery could have preserved some functional vision in a situation where the light reflex remained in the affected eye. Alleviation of preoperative nausea and vomiting, bradycardia, and somnolence indicates that the preoperative symptomatology was related to vagal stimulation from increased intraocular pressure, usually identified as an oculocardiac reflex.
Résumé
Objectif
Souligner la nécessité d’une intervention spécialisée et rapide lorsque des signes d’accroissement de la pression intra-orbiraire sont présents.
Aspects cliniques
Une enfant de quatre ans s’est présentée à l’hôpital souffrant d’un œdème orbitaire d’apparition récente, de nausées et de somnolence. La tomodensitométrie et la scintigraphie cérébrale ont montré un cerveau normal, mais une masse dans l’orbite gauche. La fillette a été dirigée en chirurgie ophtalmique le lendemain, alors que sa pupille gauche ne réagissait plus à la lumière. Les modalités de l’anesthésie ont été dictées par la présence des signes et des symptômes préopératoires de l’accroissement de la pression intraoculaire: somnolence, nausées, vomissements et bradycardie. Ces signes et symptômes se sont atténués après l’intervention.
Conclusion
Le début rapide de l’œdème orbitaire accompagné des signes physiologiques de l’augmentation de pression intraoculaire nécessitent une chirurgie d’urgence. Il est possible que l’examen spécialisé et la chirurgie précoces aient pu préserver, en partie, la vision fonctionnelle dans des circonstances où le réflexe pupillaire était conservé dans l’oeil touché. Le soulagement des nausées, des vomissements, de la bradycardie et de la somnolence préopératoires indique que la symptomatologie était reliée à une stimulation vagale provenant de la pression intraoculaire accrue, habituellement identifiée comme étant un réflexe oculocardiaque.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Donlon JV Jr. Anesthesia and eye, ear, nose, and throat surgery.In: Miller RD (Ed.). Anesthesia, 4th ed. New York: Churchill Livingstone Inc., 1994; 2182.
Schamroth L. Electrocardiographic effects of eyeball compression. Am J Cardiol 1958; 2: 321–33.
Braun U, Feise J, Mühlendyck H. Is there a cholinergic and an adrenergic phase of the oculocardiac reflex during strabismus surgery? Acta Anaesthesiol Scand 1993; 37: 390–5.
Moonie GT, Rees DL, Elton D. The oculocardiac reflex during strabismus surgery. Can Anaesth Soc J 1964; 11: 621–31.
Blanc VF, Hardy J-F, Milot J, Jacob J-L. The oculocardiac reflex: a graphic and statistical analysis in infants and children. Can Anaesth Soc J 1983; 30: 360–9.
Bailey JH. The oculocardiac reflex. Report of a case exhibiting a marked reaction following enucleation of the eyeball. Am J Ophthalmol 1935; 18: 22–5.
Wong DHW. Regional anaesthesia for intraocular surgery. Can J Anaesth 1993; 40: 635–57.
Dagnini G. Intorno ad un riflesso provocato in alcuni emiplegi collo stimolo della cornea e colla pressione sul bulbo oculare. Bull Sci Med 1908; 8: 380–1.
Aschner B. Ueber einen bisher noch nicht beschriebenen Reflex vom Auge auf Kreislauf und Atmung. Versschwinden des Radialispulses bei Druck aus das Auge. Wien Klin Wochenschr 1908; 21: 1529–30.
Wilson RP. Anesthesia.In: Spaeth GL (Ed.). Ophthalmic Surgery: Principles & Practice, 2nd ed. Philadelphia: W.B. Saunders Company, 1990: 94–5.
Van Brocklin MD, Hirons RR, Tolton RL. The oculocardiac reflex: a review. J Am Optom Assoc 1982; 53: 407–13.
Fayon M, Gauthier M, Blanc VF, Ahronheim GA, Michaud J. Intraoperative cardiac arrest due to the oculocardiac reflex and subsequent death in a child with occult Epstein-Barr virus myocarditis. Anesthesiology 1995; 83: 622–4.
Anderson RL. The blepharocardiac reflex. Arch Ophthalmol 1978; 96: 1418–20.
van den Berg AA, Lambourne A, Clyburn PA. The oculo-emetic reflex. A rationalisation of postophthalmic anaesthesia vomiting. Anaesthesia 1989; 44: 110–7.
Krohel GB, Wright JE. Orbital hemorrhage. Am J Ophthalmol 1979; 88: 254–8.
Arnold RW, Ellis FD, Wolfe TM. Prolonged oculocardiac reflex during strabismus surgery under topical anesthesia. J Pediatr Ophthalmol Strabismus 1997; 34: 252–4.
Chang WJ, Nowinski TS, Repke CS, Buerger DG. Spontaneous orbital hemorrhage in pregnant women treated with subcutaneous heparin. Am J Ophthalmol 1996: 122: 907–8.
Bart DJ, Lueder GT. Orbital hemorrhage following extracorporeal membrane oxygénation in a newborn. J Pediatr Ophthalmol Strabismus 1997; 34: 65–7.
Bailey WK, Kuo PC, Evans LS. Diagnosis and treatment of retrobulbar hemorrhage. J Oral Maxillofac Surg 1993; 51: 780–2.
Kremer I, Nissenkorn I, Feuerman P, Ben-Sira I. Congenital orbital vascular malformation complicated by massive retrobulbar hemorrhage. J Pediatr Ophthalmol Strabismus 1987; 24: 190–3.
Motha W, Cowden TP, Sires BS, Dortzbach RK. Subperiostaeal orbital hemorrhage from retrobulbar injection resulting in blindness. Arch Ophthalmol 1997; 115: 123–4.
Cionni RJ, Osher RH. Retrobulbar hemorrhage. Ophthalmology 1991; 98: 1153–5.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Westerling, D., Blohmé, J. & Stigmar, G. Orbital mass in a child causing somnolence, nausea and bradycardia. Can J Anaesth 45, 777–780 (1998). https://doi.org/10.1007/BF03012148
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03012148