
Abstract
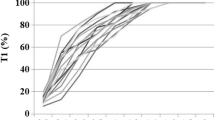
The effect of different priming doses of edrophonium were studied in 77 patients divided into seven groups (n = 11 in each). Edrophonium 1.0 mg-kg-1 was administered either in a single bolus dose (Group I; controls) or in an initial dose of 0.05, 0.1, 0.15, 0.2, 0.25 or 0.3 mg-kg-1 followed one minute later by the remainder of the 1.0 mg-kg-1 dose in Groups II to VII respectively. Reversal was attempted at ten per cent spontaneous recovery of twitch height (TI) from atracurium-induced neuromuscular blockade. Increasing the size of the priming dose from 0.05 to 0.2 mg-kg-1 resulted in a stepwise increase (p < 0.05) in recovery of TI and train-of-four (TOF) ratio. Higher priming doses (0.25 and 0.3 mg-kg-1) were not associated with further improvement in TI and TOF recovery. Reversal time, that is the time taken from the first injection of edrophonium until the TOF ratio value had reached 0.75 was significantly faster (p < 0.01) following priming with edrophonium 0.2 mg-kg-1 (Group V) when compared to Groups I, II, III, IV and VI. Reversal times were also significantly faster in Groups IV and VI when compared to the control group.
It is concluded that 0.2 mg-kg-1 appears to be the optimal priming dose for administration of edrophonium in divided doses.
Résumé
Ľeffet de différentes doses ďamorce ďédrophonium a été étudié chez 77 patients divisés en sept groupes (n = 11). Ľédrophonium 1.0 mg-kg-1 a été administré soit en une dose unique (Groupe I, contrôle) ou en une dose initiale de 0.05, 0.1, 0.15, 0.2, 0.25 ou 0.3 mg-kg-1 suivi une minute plus tard par le restant de la dose de 1.0 mg-kg-1 pour les Groupes II à VII. Ľantagonisme a été tenté après une récupération spontanée à dix pour cent de la hauteur de twitch (TI) après un bloc neuromusculaire induit par ľatracurium. Ľaugmentation de la dose ďamorce de 0.05 à 0.2 mg-kg-1 a produit une augmentation de plus en plus accrue (p < 0.05) dans la récupération de TI et du rapport de ľondée-de-quatre (TOF). La plus grande dose ďamorce (0.25 et 0.3 mg-kg-1) n’était pas associée avec de plus grandes améliorations dans la récupération de TI et TOF. Le temps ďantagonisme, qui représente le temps du début de la première injection ďédrophonium jusqu’à ľobtention ďun rapport de TOF de 0.75 était significativement plus rapide (p < 0.01) après la dose ďamorce ďédrophonium de 0.2 mg-kg-1 Groupe V) en comparaison Groupe I, II, III, IV et VI. Les temps ďantagonisation étaient aussi significativement plus rapides dans les groupes IV et VI comparativement groupe contrôle. On conclut que la dose de 0.1 mg-kg-1 apparaît optimale comme dose ďamorce pour ľadministration de ľédrophonium en doses fractionnées.
Article PDF
Similar content being viewed by others


References
Abdulatif M, Naguib M. Accelerated reversal of atracurium blockade with divided doses of neostigmine. Can Anaesth Sec J 1986; 33: 723–8.
Naguib M, Abdulatif M, Absood GH. Accelerated reversal of atracurium blockade with priming doses of edrophonium. Anesthesiology 1987; 66: 397–9.
Naguib M, Abdulatif M. Priming with anticholinesterases — the effect of different combinations of anticholinesterases and different priming intervals. Can J Anaesth 1988; 35: 47–52.
Viby-Mogensen J. Clinical evaluation of neuromuscular transmission. Br J Anaesth 1982; 54: 209–23.
Ali HH, Kin RJ. Evaluation of recovery from nondepolarizing neuromuscular block using digital neuromuscular transmission analyzer: Preliminary report. Anesth Analg 1973; 52: 740–3.
Dixon WJ. (Ed) BMDP Statistical Software. Berkeley, University of California Press, 1985.
Bevan DR. Reversal of pancuronium with edrophonium. Anaesthesia 1979; 34: 614–9.
Kopman AF. Edrophonium antagonism of pancuroniuminduced neuromuscular blockade in man: a reappraisal. Anesthesiology 1979; 51: 139–43.
Morris RB, Cronnelly R, Miller RD, Stanski DR, Fahey MR. Pharmacokinetics of edrophonium and neostigmine when antagonizing d-tubocurarine neuromuscular blockade in man. Anesthesiology 1981; 54: 399–402.
Donati F, Ferguson A, Bevan DR. Twitch depression and train-of-four ratio after antagonism of pancuronium with edrophonium, neostigmine and pyridostigmine. Anesth Analg 1983; 63: 314–6.
Jones RM, Pearce AC, Williams JP. Recovery characteristics following antagonism of atracurium with neostigmine or edrophonium. Br J Anaesth 1984; 56: 453–7.
Engbaek J, Ording H, Ostergaard D, Viby-Mogensen J. Edrophonium and neostigmine for reversal of neuromuscular blocking effect of vecuronium. Acta Anaesthesiol Scand 1985; 29: 544–6.
Lavery GG, Mirakhur RK, Gibson FM. A comparison of edrophonium and neostigmine for the antagonism of atracurium-induced neuromuscular block. Anesth Analg 1985; 64: 867–70.
Hennart D, ďHollander A, Plasman C, de Janckheere M. Importance of the level of paralysis recovery for a rapid antagonism of atracurium neuromuscular blockade with moderate doses of edrophonium. Anesthesiology 1986; 64: 384–7.
Rupp SM, McChristian JW, Miller RD, Taboada JA, Cronnelly R. Neostigmine and edrophonium antagonism of varying intensity neuromuscular blockade induced by atracurium, pancuronium or vecuronium. Anesthesiology 1986; 64: 711–7.
Kopman AF. Recovery time following edrophonium and neostigmine reversal of pancuronium, atracurium, and vecuronium steady-state infusion. Anesthesiology 1986; 65: 572–8.
Mirakhur RK, Gibson FM, Lavery GG. Antagonism of vecuronium-induced neuromuscular blockade with edrophonium or neostigmine. Br J Anaesth 1987; 59: 473–7.
Naguib M, Abdulatif M, Absood GH. The optimal priming dose for atracurium. Can Anaesth Soc J 1986; 33: 453–7.
Naguib M, Abdulatif M, Gyasi HK, Khawaji Y, Absood GH. The pattern of train-of-four fade following atracurium: influence of different priming doses. Anesth Analg 1987; 66: 427–30.
Paton WDM, Waud DR. The margin of safety of neuromuscular transmission. J Physiol (Lond) 1967; 191: 59–90.
Barber HE, Calvey TN, Muir KT. The relationship between the pharmacokinetics, cholinesterase inhibition and facilitation of twitch tension of the quaternary ammonium anticholinesterase drugs, neostigmine, pyridostigmine, edrophonium and 3-hydrophenyt-trimethylammonium. Br J Pharmacol 1979; 66: 525–30.
Bowman WC, Webb SN. Acetylcholine and anticholinesterase drugs.In: Cheymol J (ed). International Encyclopedia of Pharmacology and Therapeutics. Vol. II. Oxford: Pergamon Press, 1972: 427–502.
Payne JP, Hughes R, Al Azawi S. Neuromuscular blockade by neostigmine in anaesthetized man. Br J Anaesth 1980; 52: 69–76.
Fox MA, Keens SJ, Utting JE. Neostigmine in the antagonism of action of atracurium. Br J Anaesth 1987; 59: 468–72.
Foldes FF, Chaudhry I, Ohta Y, Amaki Y, Nagashima H, Duncalf D. The influence of stimulation parameters on the potency and reversibility of neuromuscular blockiug agents. J Neural Transmission 1981; 52: 227–49.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Naguib, M., Abdulatif, M. Priming with anticholinesterases — the effect of different priming doses of edrophonium. Can J Anaesth 35, 53–57 (1988). https://doi.org/10.1007/BF03010545
Issue Date:
DOI: https://doi.org/10.1007/BF03010545