
Résumé
Introduction
L’efficacité de la sclérothérapie endoscopique est largement reconnue dans le traitement des varices œsophagiennes hémorragiques ou de leurs récidives à long terme. La sclérothérapie des varices œsophagiennes par l’oléate d’éthanolamine a prouvé sa supériorité sur les traitements médicaux conventionnels dans le traitement à long terme des hémorragies de varices œsophagiennes. La glycérine chromée à 72%, est un polyalcool habituellement considéré comme un sclérosant chimique irritant et essentiellement utilisé pour la sclérose des varices superficielles: ses principaux avantages résident dans la rareté des hyperpigmentations et télangiectasies secondaires et parce qu’elle n’entraîne des nécroses par extravasation que très exceptionnellement. A ce jour, aucune étude de son efficacité sur les varices œsophagiennes hémorragiques n’avait été menée.
But
Etudier l’efficacité de la glycérine chromée à 72%versus l’oléate d’éthanolamine sur l’évolution (éradication) à long terme des hémorragies des varices œsophagiennes.
Méthodes
Cette étude a été menée dans l’unité centrale d’endoscopic des hôpitaux universitaires d’Ain Shams d’avril 2003 jusqu’à fin décembre 2003. Quarante patients présentant des varices œsophagiennes hémorragiques ont été randomisés en 2 groupes: la glycérine chromée et l’oléate d’éthanolamine ont été utilisés comme agents sclérosants respectivement dans le groupe 1 (20 patients) et le groupe 2 (20 patients). Les patients des deux groupes ont été soumis à des séances de sclérothérapie endoscopique bi-hebdomadaires pour traiter les varices œsophagiennes jusqu’à complète disparition (éradication) ou sclérose de la moitié inférieure de l’œsophage.
Résultats
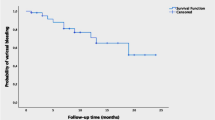
Les deux groupes étaient homogènes quant à l’âge, le sexe, la classification de Child, les résultats du bilan hépatique, l’étiologie de la cirrhose, le grade et la taille des varices, le nombre moyen de séances de sclérothérapie et la quantité moyenne totale de sclérosant utilisée par patient. Toutes les séances de sclérothérapie ont été faites par le même endoscopiste pour éviter tout biais opérateur-dépendant. Les patients du groupe 1 ont subi 72 séances de sclérothérapie par de la glycérine chroméevs 76 séances par de l’oléate d’éthanolamine dans le groupe 2. Il y a eu un meilleur taux d’éradication des varices dans le groupe 1 que dans le groupe 2 (75%vs 60%) mais cette différence n’était pas statistiquement significative. Dans les deux groupes (groupe 1 et groupe 2) ne sont survenues que des complications mineures sans différence significative: douleurs thoraciques (40%vs 55%), dysphagies transitoires (15%vs 40%), petits ulcères de post-sclérothérapie (35%vs 15%), suintements contrôlables du site de ponction (55%vs 55%) et fièvre modérée (5%vs 20%). Peu de complications majeures ont été enregistrées dans les deux groupes. La récidive du saignement est survenue dans 2 cas (10%) dans le groupe 1 contre 4 cas (20%) dans le groupe 2. D’importants ulcères sont apparus en post-sclérothérapie dans 2 cas (10%) dans le groupe 2 et aucun dans le groupe 1. Un malade (5%) du groupe 2 est décédé d’une récidive du saignement et aucun dans le groupe 1. L’analyse statistique de régression pas à pas traduit selon le test de Fischer montre que les paramètres les plus sensibles pour prédire les éradications sont: le nombre de séances, la durée du suivi, le nombre de cordons variqueux œsophagiens et les produits testés. La réussite de l’éradication dépend de l’augmentation du nombre de séances > 3, de la durée du suivi > 5 mois; de la diminution du nombre de cordons variqueux < 4 et de l’utilisation de la glycérine chromée (odd ratio = 0.75vs 0.60 pour l’oléate d’éthanolamine) (test de Fisher: ratio = 15.375,p < 0.001).
Conclusion
La glycérine chromée (Sclérémo®) est un sclérosant efficace qui pourrait être utilisé dans l’éradication de varices œsophagiennes avec quelques complications mineures et peu de complications majeures. Son effet est comparable à celui de l’oléate d’éthanolamine.
Summary
Background
Endoscopie sclerotherapy is widely accepted as an effective method in the management of actively bleeding oesophageal varices and in the long term management of bleeding varices. Sclerotherapy of oesophageal varices with Ethanolamine Oléate proved to be superior to conventional medical treatment in the long term management of bleeding oesophageal varices.
A compound of 72% chromated glycerin, is a polyalcohol that often is considered a chemical irritant sclérosant and is principally useful in the sclerosis of varicose veins. Its principal advantage is that it rarely causes hyperpigmentation or telangiectasic matting, and that it very rarely causes extravasation necrosis. No reports, so far, about its use in the management of bleeding oesophageal varices.
Objective
Is to study the efficacy of 72% chromated glycerine in the long term management (eradication) of bleeding oesophageal varices compared to ethanolamine oléate.
Methods
The present study was conducted in the central unit of endoscopy, Ain Shams University Hospitals from the beginning of April 2003 till the end of December 2003. Forty patients with bleeding oesophageal varices were randomly allocated into two groups: group 1 (20 patients) where chromated glycerine was used as a sclérosant agent and group 2 (20 patients) where ethanolamine oléate was the sclerosing material. The patients of both groups were subjected to biweekly sessions of endoscopic sclerotherapy for the oesophageal varices till complete disappearance (eradication) or sclerosis of the varices in the lower half of the oesophagus.
Results
Both groups were matching together as regards age, gender, Child’s classification, liver function tests, cause of liver cirrhosis, grade and length of varices, mean number of sessions of sclerotherapy and mean total amount of sclérosant per patient. All sessions of sclerotherapy were done by the same endoscopist to prevent bias. Group 1 patients received 72 sessions of sclerotherapy with chromated glycerine vs 76 sessions of ethanolamine oleate for group 2. There was a higher rate of eradication of varices in group 1 than in group 2 (75% vs 60%) but this difference was statistically non significant. Both groups (group 1 and group 2) showed minor complications in the form of chest Pain (40% vs 55%), transient dysphagia (15% vs 40%), small post-sclerotherapy ulcers (35% vs 15%), controllable ooze from the puncture site (55% vs 55%) and low grade fever (5% vs 20%), with no statistically significant difference. Few major complications were recorded in both groups. Recurrence of bleeding occurred in 2 cases (10%) of group 1 versus 4 cases (20%) of group 2. Large post-sclerotherapy ulcers occurred in 2 cases (10%) of group 2 while no large ulcers were reported in group 1. One patient (5%) in group 2 died from recurrence of bleeding while no fatalities were reported in group 1. Stepwise multiregression analysis shows that the most sensitive parameters that can predict eradications are the number of sessions, duration of follow-up, number of columns of oesophageal varices and the tested materials. Successful eradications depends on increased number of sessions > 3, duration of follow-up > 5 months; decreased number of columns of varices < 4 and usage of chromated glycerine (odd ratio =0.75 vs0.60 for ethanol oléate) (Fisher: ratio =15.375, p <0.001).
Conclusion
chromated glycerine (Sclérémo®) is an efficient sclérosant and could be used in eradication of oesophageal varices with minor complications and few major complications. Its effect is comparable to that of Ethanolamine Oléate.
Similar content being viewed by others


Références
Navarro VJ, Garcia Tsao G. Variceal haemorrhage. Crit Care Clin 1991; 11:12.
Burroughs A, Hezzanolte G, Philips A, et al. Cirrhotics with variceal haemorrhage: the importance of the time interval between admission and the start of the analysis for survival and re-bleeding rates. Hepatology 1969; 9: 801.
Silverstein FE, Gilbert DA, Tedesco FJ, et al. The national ASGE survey on upper gastrointestinal bleeding clinical prognostic factors. Gastroint Endose 1981; 27: 80–93.
Graham DY, Smith JL. The course of patients after variceal hemorrhage. Gastroenterology 1981; 80: 800–6.
El-Wakil MR. Assessment of sclerotherapy in the management of bleeding oesophageal varices. MD Thesis. Ain Shams University. Cairo 1987.
Feied CF. Sclerosing solutions. On: The American College of Phlebology Web Site. 2003.
Dagradi A, Stemptein S, Owens L. Bleeding oesophagogastric varices. Arch. Surg. 1966; 92: 944–7.
Infante RC, Esnaola S, Villeneuve JP. Role of endoscopic variceal sclerotherapy in the long term management of variceal bleeding: A meta-analysis. Gasteroenterology 1989; 96:1087–92.
Graham DY, Smith JL. The course of patients after variceal hemorrhage. Gastroenterology 1981; 80: 800–6.
Bessa, S, Helmy I. Esophageal transaction by the EEA stapler for bleeding esophageal varices in schistosomal hepatic fibrosis. Surg Gyn Obs 1988; 166:17.
Bakkar A. Upper gastrointestinal haemorrhage with special reference to variceal bleeding in Ain Shams University Specialized Hospital. Msc Thesis Tropical Medicine. Faculty of Medicine Ain Shams University, Cairo. 1994.
D’Amico G, de Franchis R, Torri V. End of the century reappraisal of the 6 week outcome of upper gastrointestinal bleeding in cirrhosis: a prospective study. Gastroenterology. 1999; 116(suppl):1199A.
Matsumoto H, Suzuki F, Souda K et al. Improved long term survival following complete eradication of esophageal varices by sclerotherapy. Hepatogastroenterology 1999; 46 (25): 172–6.
Gasim B, Fedail S, Mussad A. et al. Endoscopie sclerotherapy for bleeding oesophegeal varices: experience in Sudan. Trop Gastroenterol 2002; 23 (2): 107–9.
Zargar S A, Yatto G N, Javid G. et al. Fifteen-Year follow up of endoscopic injection sclerotherapy in children with extrahepatic portal venous obstruction. J. Gastroenterol Hepatol 2004; 19 (2): 139–145.
Brian C Leach, M, Mitchel P. et al. Comparative Trial between Sodium Tetradecyl sulfate and glycerin in the treatment of telangiectatic leg vein. Dermatologie surgery 2003; 29 (6): 612.
Vandendriessche M. Int J Angiol 1999; 8: 98–10.
Martin D, Goldman M. A comparison of sclerosing agents: clinical and histologie effects of intravascular sodium teteradecyl sulfate and chromated glycerin in the dorsal rabbit ear vein. J Dermatol Surg Oncol 1990; 16 (1): 18–22.
Sanowski RA and Waring JP Endoscopie techniques and complications in variceal sclerotherapy. J Clin Gastroenterol 1988;10: 504–13.
Zambelli A, Pisano G, De Grazia F, et al. Complications of the endoscopic sclerotherapy of esophageal varices. G Ital Endose Dig 1991; 14:103–19.
Ljubieie N, Pero M. Endoscopie therapy of gastroesophageal variceal haemorrhage. Acta Clin Croat 2001; 40 (2): 125.
Krige JE, Bornman PC, Goldberg PA, et al. Variceal rebleeding and recurrence after endoscopic injection sclerotherapy: a prospective evaluation in 204 patients. Arch Surg 2000; 135 (11): 1315–22.
Author information
Authors and Affiliations
About this article
Cite this article
El-Wakil, M.R. Évaluation de l’efficacité de la glycérine chromée versus l’oléate d’éthanolamine dans le traitement de varices œsophagiennes hémorragiques chez des patients égyptiens: une étude pilote. Acta Endosc 34, 691–704 (2004). https://doi.org/10.1007/BF03009078
Issue Date:
DOI: https://doi.org/10.1007/BF03009078