
Abstract
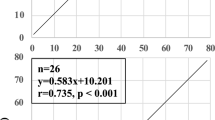
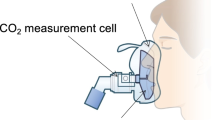
To determine whether end-tidal PCO2 (PETCO2) measurements obtained with two infrared capnometers accurately approximates the arterial PCO2 PaCO2) in critically ill neonates, simultaneous measurements of PETCO2 were obtained from the distal and proximal ends of the tracheal tube with a sidestream capnometer (Puritan Bennett/Datex — BP/D) and from the proximal end with a mainstream capnometer (Hewlett-Packard — HP) in 20 intubated neonates. Distal sidestream PETCO2 and mainstream PetCO2 correlated with the PaCO2 (r2 = 0.66 and 0.61, respectively) within the range of 26–57 mmHg PaCO2. However, proximal PETCO2 with the sidestream capnometer correlated very poorly (r2 = 0.09) with PaCO2. The slope of the least square regression line for the distal sidestream capnometer, 0.67, was significantly less than that for the mainstream capnometer, 0.78 but both were significantly greater than that for the proximal sidestream capnometer, 0.39 (P < 0.05). The slope of the regression for the proximal sidestream capnometer did not differ significantly from horizontal. Insertion of the mainstream sensor for the HP capnometer significantly increased the transcutaneous CO2 when compared with preinsertion values. We conclude that both distal sidestream and mainstream capnometry provide accurate estimates of the PaCO2 in critically ill neonates.
Résumé
En enregistrant simultanément la PCO2 en fin d’expiration (PETCO2) par capnomètre aspirant (Puritan Bennett/Datex —PB/D) à partir du bout distal et du bout proximal d’un tube endotrachéal et par capnomètre passif (Hewlett-Packard — HP) au bout proximal du tube, nous avons mesuré l’efficacité de ces techniques d’estimation à l’infrarouge de la PCO2 artérielle (PaCO2) chez 20 nouveauxnés. Pour des PaCO2 de l’ordre de 26 à 57 mmHg, la pente de la ligne de régression entre la PETCO2 et la PaCO2 était de 0,78 avec le capnomètre passif (r2 = 0,61), significativement plus grande que la pente de 0,67 du capnomètre aspirant au bout distal (r2 = 0,66) mais toutes deux se détachaient (P < 0,05) de celle du capnomètre aspirant au bout proximal qui, avec une valeur de 0,39, pouvait être confondue avec l’horizontale (r2 = 0,09). Pour sa part, l’insertion dans le circuit de la fenêtre de mesure du capnomètre passif contribuait à augmenter la PCO2 transcutanée. La capnométrie passive ou par aspiration du bout distal donne donc un bon estimé de la PaCO2 des nouveauxnés gravement malades.
Article PDF
Similar content being viewed by others

Avoid common mistakes on your manuscript.
References
Meny RG, Bhat AM, Aranas E. Mass spectrometer monitoring of expired carbon dioxide in critically ill neonates. Crit Care Med 1985; 13: 1064–6.
Nelson NM, Prod’hom LS, Cherry RB, Lipsitz PJ, Smith CA. Pulmonary function in the newborn infant II. Perfusion — estimation by analysis of the arterial-alveolar carbon dioxide difference. Pediatrics 1962; 30: 975–89.
Epstein MF, Cohen AR, Feldman HA, Raemer DB. Estimation of PaCO2 by two noninvasive methods in the critically ill newborn infant. J Pediatr 1985; 106: 282–6.
McEvedy BAB, McLeod ME, Mulera M, Kirpalani H, Lerman J. End-tidal, transcutaneous and arterial CO2 measurements in critically ill neonates: a comparative study. Anesthesiology 1988; 69: 112–6.
Badgwell JM, McLeod ME, Lerman J, Creighton RE. End-tidal PCO2 measurements sampled at the distal and proximal ends of the endotracheal tube in infants and children. Anesth Analg 1987; 66: 959–64.
Schena J, Thompson J, Crone RK. Mechanical influences on the capnogram. Crit Care Med 1984; 12: 672–4.
Eberhard P, Mindt W, Schafer R. Methodologic aspects of cutaneous pCO2 monitoring. Intensive Care Med 1981; 7: 249–64.
Zar JH. Biostatistical Analysis. Second edition. Prentice-Hall: Englewood Cliffs, 1984, pp. 309–11, 315–7.
Scheiber RA, Namnoum A, Sugden A, Saville AL, Orr RA. Accuracy of expiratory carbon dioxide measurements using the coaxial and circle breathing circuits in small subjects. J Clin Monit 1985; 1: 149–55.
Hand IL, Shepard EK, Krauss AN, Auld PAM. Discrepancies between transcutaneous and end-tidal carbon dioxide monitoring in the critically ill neonates with respiratory distress syndrome. Crit Care Med 1989; 17: 556–9.
Pascucci RC, Schena JA, Thompson JE. Comparison of a sidestream and mainstream capnometer in infants. Crit Care Med 1989; 17: 560–2.
Watkins AMC, Weindling AM. Monitoring of end tidal CO2 in neonatal intensive care. Arch Dis Child 1987; 62: 837–9.
Dumpit FM, Brady JP. A simple technique for measuring alveolar CO2 in infants. J Appl Physiol 1978; 45: 648–50.
Hillier SC, Badgwell JM, McLeod ME, Lerman J, Creighton RE. End-tidal PCO2 measurements in infants and children ventilated with the Sechrist infant ventilator. Can J Anaesth 1989; 37: 318–21.
Mogue LR, Rantala B. Capnometers. J Clin Monit 1988; 4: 115–21.
Gravenstein N. Capnometry in infants should not be done at lower sampling flow rates. Clin Monit 1989; 5: 63.
Badgwell JM, Wolf AR, Morton WD, Lerman J, McLeod ME, Creighton RE. Fresh gas flow formulae do not accurately predict end-tidal pCO2 in paediatric patients. Can J Anaesth 1988; 35: 581–6.
Nelson NM, Prod’hom LS, Cherry RB, Lipsitz PJ, Smith CA. Pulmonary function in the newborn infant. I: Methods: ventilation and gaseous metabolism. Pediatrics 1962; 30: 963–74.
McCann EM, Lewis K, Deming DD, Donovan MJ, Brady JP. Controlled trial of furosemide therapy in infants with chronic lung disease. J Pediatr 1985; 106: 957–62.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
McEvedy, B.A.B., McLeod, M.E., Kirpalani, H. et al. End-tidal carbon dioxide measurements in critically ill neonates: a comparison of side-stream and mainstream capnometers. Can J Anaesth 37, 322–326 (1990). https://doi.org/10.1007/BF03005583
Issue Date:
DOI: https://doi.org/10.1007/BF03005583