
Summary and Conclusions
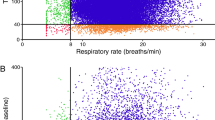
Blood gases, tidal volumes, and respiratory rates were measured preoperatively and during surgery with intermittent positive pressure breathing of 50 per cent oxygen. The ventilator was set to provide a tidal volume and rate closely approximating that in the awake state.
Pao2 dropped significantly during IPPB despite the similar Pio2, Vt, f, and\(\dot VE\). PaCo2 remained the same. As time elapsed, a progressive fall in Pa02 occurred. The P ao2 reached its minimum at approximately one hour after the initiation of IPPB. Individual patient responses varied considerably for both changes in Pao2 and Paco2- Although three patients developed Pao2 values below 100 mm. Hg, none was considered hypoxaemic since the respective Pao2 was at a level above the air control. Some Pao2 values dropped approximately 150 mm. Hg below the awake control while others remained at the 250 mm. Hg level. It should be realized that the tidal volumes used were lower than that during the usual clinical administration of anaesthesia. Changes in PaCo2 were pot usually related to changes in Pao2, and hypocarbia and acceptable estimated VA were frequently associated with a Pao2 lower than during the control. Therefore, under the same conditions, it is concluded that if the tidal volume and respiratory rate used during IPPB are identical to those of the awake control, then during the inhalation of 50 per cent O2 patients are able to maintain normal Paco2 and slightly lower Pao2.
Résumé
Chez 13 malades, nous avons mesuré à toutes les 15 minutes avant et durant l’anesthésie et la chirurgie, alors que le malade respirait sous pression positive intermittente, nous avons mesuré les gaz du sang, les volumes courants et la vitesse de la respiration. Le ventilateur fournissait spécifiquement un air courant et une vitesse respiratoire indentiques à ceux du malade réveillé. Le taux d’oxygene éinhalé était de 50 pour cent.
La2 a baissé de façon marquée durant la pression positive intermittente; la PaC02 est demeurée la même. Le changement de la Pao2 a été progressif et a atteint son sommet au bout d’une heure. Bien que, chez certains malades, la Pa02 ait été au-dessous de 100 mm. Hg, nous n’avons pas estimé qu’il existait d’hypoxémie puisque la Pa02 est demeuree au-dessus du contrôle lorsque le malade respirait de l’air. Nous avons observeé des variations individuelles considerables de la Pa02 et de la PaCo2- Les changements de la PaCo2 n’etaient pas habituellement à l’opposé de ceux de la Pa02 et l’hypocarbie en présence d’un volume/minute adéquat s’accompagnait généralement d’une Pao2 plus basse que durant le contrôle.
Article PDF
Similar content being viewed by others

Avoid common mistakes on your manuscript.
References
Campbell, E. J. M.;Nunn, J. F.; &Peckett, B. W. A Comparison of Artificial Ventilation and Spontaneous Respiration with Particular Reference to Ventilation-Bloodflow Relationships. Brit. J. Anaesth.30: 166 (1958).
Nunn, J. F. &Hill, D. W. Respiratory Dead Space and Arterial to End-Tidal CO., Tension Difference in Anesthetized Man. J. Appl. Physiol.15: 383 (1960).
Frumin, M. K.et al. Alveolar-Arterial O2 Difference during Artificial Respiration in Man. J. Appl. Physiol.14: 694 (1959).
Stark, D. &Smith, H. Pulmonary Vascular Changes during Anaesthesia. Brit. J. Anaesth.32: 460(1960).
Bendixen, H. H.et al. Impaired Oxygenation in Surgical Patients during General Anesthesia with Controlled Ventilation: A Concept of Atelectasis. New England J. Med.269: 991(1963).
Conway, E. M. &Payne, J. P. Hypoxaemia Associated With Anaesthesia and Controlled Respiration. Lancet1: 12 (1964).
Hedley-Whyte, J.;Laver, M. &Bendixen, H. H. Effect of Changes in Tidal Ventilation on Physiologic Shunting. Am. J. Physiol.206: 891 (1964).
Laver, M.et al. Lung Volume, Compliance, and Arterial Oxygen Tensions during Controlled Ventilation. J. Appl. Physiol.19: 725 (1964).
Sykes, M. K.;Young, W. E.; &Robinson, B. E. Oxygenation during Anaesthesia with Controlled Ventilation. Brit. J. Anaesth.37: 314 (1965).
Nunn, J. F.;Bergman, N. A.; &Coleman, A. J. Factors Influencing the Arterial Oxygen Tension during Anaesthesia with Artificial Ventilation. Brit. J. Anaesth.37: 898 (1965).
Pontoppidan, H.et al. Ventilation and Oxygen Requirements during Prolonged Artificial Ventilation in Patients with Respiratory Failure. New England J. Med.273: 401 (1965).
Gold, M. I.;Han, Y. A.; &Helrich, M. Pulmonary Mechanics during Anesthesia: III. Influence of Intermittent Positive Pressure and Relation to Blood Gases. Anesth. & Analg.45: 631 (1966).
Watson, W. E. Observations on the Dynamic Lung Compliance of Patients with Respiratory eakness Receiving Intermittent Positive Pressure Respiration. Brit. J. Anaesth.34: 690 (1962).
Gold, M. I. &Helrich, M. Pulmonary Compliance during Anesthesia. Anesthesiology.26: 281 (1965).
Nunn, J. F. Factors Influencing the Arterial Oxygen Tension during Halothane Anaesthesia with Spontaneous Respiration. Brit. J. Anaesth.36: 327 (1964).
Webb, S. J. S. &Nunn, J. F. Comparison between Nitrogen and Nitrous Oxide in the Development of Venous Admixture during Anaesthesia. Anaesthesia.21: 95 (1966).
Rahn, H. &Farhi, L. E. Ventilation, Perfusion, and Gas Exchange: The Va/Q Concept, inW. O. Fenn andH. Rahn, Handbook of Physiology, Section 3: Respiration I. Baltimore: Williams and Wilkins (1964), chap. 3, pp. 751–54.
Nunn, J. F. The Lung as a Black Box. Canad. Anaesth. Soc. J.13: 81 (1966).
Bonic, J. J.et al. Effects of Surgical Pneumothorax on Pulmonary Ventilation. Anesthesiology.22: 955 (1961).
Author information
Authors and Affiliations
Additional information
This investigation was supported by Public Health Service Research Grant HE-06429 from the National Institutes of Health.
Rights and permissions
About this article
Cite this article
Gold, M.I., Helrich, M. Ventilation and blood gases in anaesthetized patients. Can. Anaes. Soc. J. 14, 424–434 (1967). https://doi.org/10.1007/BF03003805
Issue Date:
DOI: https://doi.org/10.1007/BF03003805