
Abstract
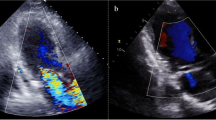
We describe a patient with acute mitral regurgitation due to complete rupture of the papillary muscle immediately after successful late reperfusion for inferior myocardial infarction. An 81-year-old woman was admitted complaining of mild chest discomfort. Although the electrocardiograms, biochemical test results, and her clinical history showed that several days had passed since the onset of acute myocardial infarction, a late coronary stenting was performed. Immediately after successful stenting, she suddenly developed acute pulmonary edema, leading to cardiogenic shock. In addition to high pulmonary capillary wedge pressure (mean 35 mmHg), color Doppler imaging revealed massive mitral regurgitation caused by complete rupture of the posterior papillary muscle. Emergent mitral valve replacement with a prosthetic valve was performed, saving the patient. Hence, late reperfusion should be considered carefully when treating a patient with a high risk, such as an elderly patient or a patient with single-vessel disease or initial transmural myocardial infarction.
Similar content being viewed by others

References
Chevalier P, Burri H, Fahrat F, Cucherat M, Jegaden O, Obadia JF, et al. Perioperative outcome and long-term survival of surgery for acute post-infarction mitral regurgitation. Eur J Cardiothorac Surg 2004; 26: 330–5.
Thompson CR, Buller CE, Sleeper LA, Antonelli TA, Webb JG, Jaber WA, et al. Cardiogenic shock due to acute severe mitral regurgitation complicating acute myocardial infarction: A report from the SHOCK Trial Registry. Should we use emergently revascularize occluded coronaries in cardiogenic shock? J Am Coll Cardiol 2000; 36: 1104–9.
Aversano T, Aversano LT, Passamani E, Knatterud GL, Terrin ML, Williams DO, et al. Thrombolytic therapy vs. primary percutaneous coronary intervention for myocardial infarction in patients presenting to hospitals without on-site cardiac surgery: A randomized controlled trial. JAMA 2002; 287: 1943–51.
Hirayama A, Adachi T, Asada S, Mishima M, Nanto S, Kusuoka H, et al. Late reperfusion for acute myocardial infarction limits the dilatation of left ventricle without the reduction of infarct size. Circulation 1993; 88: 2565–74.
Ishikawa K, Benefits of late reperfusion in the treatment of acute myocardial infarction. J Thromb Thrombolysis 2002; 13: 191–200.
Solodky A, Behar S, Herz I, Assali A, Porter A, Hod H, et al. Comparison of incidence of cardiac rupture among patients with acute myocardial infarction treated by thrombolysis versus percutaneous transluminal coronary angioplasty. Am J Cardiol 2001; 87: 1105–8.
Reiner JS, Lundergan CF, Tenner MP, Abraham AA, Ross AM. Ventricular free wall and septal rupture (double rupture): A “pseudocomplication” during post-infarction laser angioplasty. Cathet Cardiovasc Diagn 1993; 30: 147–9.
Papaleo R, Depowski PL, Dincer AD, Houghton JL. Left ventricular free wall rupture during coronary intervention after acute myocardial infarction: Report of two cases exhibiting fatal pseudocomplications. Catheter Cardiovasc Interv 1999; 47: 67–72.
Jouan J, Tapia M, C Cook R, Lansac E, Acar C. Ischemic mitral valve prolapse: Mechanisms and implications for valve repair. Eur J Cardiothorac Surg 2004; 26: 1112–7.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Kamohara, K., Yoshikai, M. & Murayama, J. Complete rupture of the posterior papillary muscle caused by late reperfusion for acute myocardial infarction. Jpn J Thorac Caridovasc Surg 54, 124–127 (2006). https://doi.org/10.1007/BF02744876
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF02744876