
Abstract
Background
Regional nodal basin control is an important goal of lymphadenectomy in the management of melanoma patients with nodal disease. The purpose of this study was to determine if previous sentinel lymph node (SLN) biopsy compromises the ultimate regional nodal control achieved by subsequent therapeutic lymph node dissection in melanoma patients with microscopic lymph node metastases.
Methods
A surgical melanoma database and hospital records were reviewed for 602 patients with primary cutaneous melanoma who underwent successful lymphatic mapping and SLN biopsy between 1991 and 1997.
Results
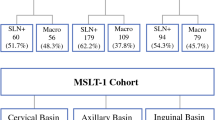
A total of 105 (17%) of 602 patients had histologically positive SLNs and were offered therapeutic lymphadenectomy; 101 (96%) underwent this procedure. Thirty-six patients (36%) developed recurrent melanoma at one or more sites. The median follow-up period was 30 months. Recurrence in the previously dissected nodal basin was observed in 10 patients (10%); none had recurrence at only that site. Nodal basin disease appeared after local/in-transit (n=6) or distant (n=1) failure in seven patients and, as a component of the first site of failure, simultaneously with local/in-transit (n=2) or distant (n=1) recurrence in three patients.
Conclusions
Nodal basin failure after lymphadenectomy in patients who underwent previous biopsy of a histologically positive SLN is primarily a function of aggressive locoregional disease rather than of contamination from previous surgery. Because regional nodal control was comparable with that in other series, we conclude that SLN biopsy with selective lymphadenectomy does not compromise regional nodal basin control.
Similar content being viewed by others


References
Ross M. The case for elective lymphadenectomy.Surg Oncol Clin N Am 1992;1:205–22.
Ross M, Balch C. The current management of cutaneous melanoma,Adv Surg 1990;24:139–200.
Balch C, Milton G, Cascinelli N, et al. Elective lymph node dissection: pros and cons. In. Balch C, Houghton A, Milton G, et al., eds.Cutaneous Melanoma, 2nd ed. Philadelphia: J.B. Lippincott, 1992:345.
Slingluff CL Jr, Stidham KR, Ricci WM, Stanley WE, Seigler HF. Surgical management of regional lymph nodes in patients with melanoma.Ann Surg 1994;219:120–30.
Kelemen P, Wanek L, Morton D. Lymph node biopsy does not impair survival after therapeutic dissection for palpable melanoma metastases.Ann Surg Oncol 1999;6:139–43.
Balch CM, Soong SJ, Murad TM, Ingalls AL, Maddox WA. A multifactorial analysis of melanoma: III. Prognostic factors in melanoma patients with lymph node metastases (stage II).Ann Surg 1981;193:377–88.
Landis S, Murray T, Bolden S, Wingo P. Cancer statistics.CA Cancer J Clin 1999;49:8–31.
Miller EJ, Daly JM, Synnestvedt M, Schultz D, Elder D, Guerry D 4th. Loco-regional nodal relapse in melanoma.Surg Oncol 1992;1:333–40.
Calabro A, Singletary S, Balch C. Patterns of relapse in 1001 consecutive patients with melanoma nodal metastases.Arch Surg 1989;124:1051–5.
Gershenwald JE, Thompson W, Mansfield PF, et al., Multi-institutional lymphatic mapping experience: the prognostic value of sentinel lymph node status in 612 stage I or II melanoma patients.J Clin Oncol 1999;17:976–83.
Lefebvre JL, Coche-Dequeant B, Van JT, et al. Cervical lymph nodes from an unknown primary tumor in 190 patients.Am J Surg 1990;160:443–6.
Austin JR, Byers RM, Brown WD, Wolf P. Influence of biopsy on the prognosis of cutaneous melanoma of the head and neck.Head Neck 1996;18:107–17.
Gershenwald JE, Colome MI, Lee JE, et al. Patterns of recurrence following a negative sentinel lymph node biopsy in 243 patients with stage I or II melanoma.J Clin Oncol 1998;16:2253–60.
Ross M, Reintgen D, Balch C. Selective lymphadenectomy: emerging role for lymphatic mapping and sentinel node biopsy in the management of early stage melanoma.Semin Surg Oncol 1993;9:219–23.
Morton DL, Wen DR, Wong JH, et al. Technical details of intraoperative lymphatic mapping for early stage melanoma.Arch Surg 1992;127:392–9.
Morton DL, Wen DR, Cochran A. Management of early-stage melanoma by intraoperative lymphatic mapping and selective lymphadenectomy or “watch and wait.”Surg Oncol Clin N Am 1992;1:247–59.
Reintgen D, Cruse C, Wells K, et al. The orderly progression of melanoma nodal metastases.Ann Surg 1994;220:759–67.
Gershenwald JE, Tseng CH, Thompson W, et al. Improved sentinel lymph node localization in primary melanoma patients with the use of radiolabeled colloid.Surgery 1998;124:203–10.
Gadd M, Coit D. Recurrence patterns and outcome in 1019 patients undergoing axillary or inguinal lymphadenectomy for melanoma.Arch Surg 1992;127:1412–6.
Coates AS, Ingvar CI, Peterson-Schaefer K, et al. Elective lymph node dissection in patients with primary melanoma of the trunk and limbs treated at the Sydney Melanoma Unit from 1960 to 1991.J Am Coll Surg 1995;180:402–9.
Warso MA, Das Gupta TK. Melanoma recurrence in a previously dissected lymph node basin.Arch Surg 1994;129:252–5.
Monsour P, Sause W, Avent J, Noyes R. Local control following therapeutic nodal dissection for melanoma.J Surg Oncol 1993;54:18–22.
Buzaid AC, Ross MI, Balch CM, et al. Critical analysis of the current American Joint Committee on Cancer staging system for cutaneous melanoma and proposal of a new staging system.J Clin Oncol 1997;15:1039–51.
Coit D, Rogatko A, Brennan M. Prognostic factors in patients with melanoma metastatic to axillary or inguinal lymph nodes: a multivariate analysis.Ann Surg 1991;214:627–36.
Author information
Authors and Affiliations
Additional information
J.E.G. and R.S.B contributed equally to this study. Presented at the 52nd Annual Meeting of the Society of Surgical
Rights and permissions
About this article
Cite this article
Gershenwald, J.E., Berman, R.S., Porter, G. et al. Regional Nodal basin control is not compromised by previous sentinel lymph node biopsy in patients with melanoma. Annals of Surgical Oncology 7, 226–231 (2000). https://doi.org/10.1007/BF02523658
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF02523658