
Abstract
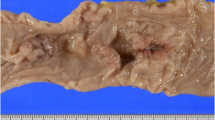
The presentation of change of bowel habit, weight loss, muscle wasting, ascites, and the surgical appearance of “omental cake” are almost pathognomonic of advanced gastrointestinal malignancy. In our case, these symptoms represented a unique presentation of the condition sclerosing mesenteritis. Despite its rarity, the clinician should be aware of this “sheep in wolfs clothing”, the clinical importance of which lies in the condition's benign and selflimiting course and imparts to the patient a prognosis and treatment that could not be further removed from that of advanced malignancy. Investigations that may be helpful to the surgeon in distinguishing the condition from carcinomatosis and avoiding unnecessary laparotomy include preoperative colonoscopy, barium enema, cytology of any ascites, and intraoperative frozen section biopsy. Treatment of the condition is conservative unless it has caused extrinsic bowel obstruction.
Similar content being viewed by others

References
Jura V. Sulla mesentente retrattile e sclerosante. Policlinico 1924;31:575–81.
Durst AL, Freund H, Rosenmann E,et al. Mesenteric panniculitis: review of the literature and presentation of cases. Surgery 1977;81:203–11.
Spark KB, Yakovac WC, Wagget J. Retractile sclerosing mesenteritis: case report. Clin Pediatr (Phila) 1971;10:119–22.
Tedeschi CG, Botta GC. Retractile mesenteritis. N Engl J Med 1962;266:1035–40.
Rigaud C, Bogomoletz WV. Association mesentrite retractile et ischaemique. Ann Pathol 1983;3:171–3.
Gayliss H, Isaacson C, Decker GA. Mesenteric panniculitis presenting as abdominal aortic aneurysm. Surgery 1973;74:626–30.
Thompson GT, Fitzgerald EF, Somers SS. Retractile mesenteritis of the sigmoid colon. Br J Radiol 1985;58:266–7.
Perez-Fontan FJ, Rafaela S, Sanchez J, Iglesias P, Sanjurjo P, Ruiz J. Retractile mesenteritis involving the colon: barium enema, sonographic, and CT findings. AJR Am J Roentgenol 1986;147:503–5.
Bush RW, Hammar SR, Rudolph RH. Sclerosing mesenteritis: response to cyclophosphamide. Arch Intern Med 1986;146:503–5.
Tytgat GN, Roozendaal K, Winter W, Esseveld MR. Successful treatment of a patient with retractile mesenteritis with prednisolone and azathiaprine. Gastroenterology 1980;79:352–6.
Kelly JK, Hwang W. Idiopathic retractile (sclerosing) mesenteritis and its differential diagnosis. Am J Surg Pathol 1989;13:513–41.
Author information
Authors and Affiliations
About this article
Cite this article
Wilkinson, J.M., Nyamekye, I., Reed, M.W.R. et al. Advanced gastrointestinal malignanq or benign inflammatory disease? an unusual presentation of sclerosing mesenteritis. Dis Colon Rectum 37, 1155–1157 (1994). https://doi.org/10.1007/BF02049821
Issue Date:
DOI: https://doi.org/10.1007/BF02049821