
Summary
The DPTI/STTI ratio as an estimate of the myocardial O2 supply/demand ratio and the prediction of myocardial blood flow (MBF) by the diastolic pressure time index (DPTI) and other indices have been examined in intact anesthetized dogs. We analyzed 89 steady states including maximal alterations of the variables determining DPTI and STTI. Myocardial blood flow was directly measured in the coronary sinus with a differential pressure catheter. All experiments were carried out under maximal coronary dilation obtained by application of dipyridamol. Hemodynamics and MBF were varied by use of pressure loading, β-stimulation and β-blockade, hypo- and hypervolemia, electrical stimulation and hemodilution. Hemodynamic variations included clinically significant situations such as tachycardiac heart failure based on exhausted coronary vascular reserve and severe anemia. Parameters of sufficient myocardial O2 supply were coronary venous O2 saturation, precordial Ecg, hemodynamic evaluation of myocardial performance, result of autopsy and determination of the wet and dry weight ratio.
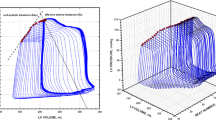
All tested parameters show a poor correlation for prediction of MBF. Correlation coefficient for DPTI is r=0.60. Using the primary data ofBuckberg (1) we obtained similar results for the correlation of DPTI to subendocardial blood flow measured with microspheres (r=0.65). The highest r (0.66) was found in our data for the difference between mean diastolic aortic pressure and mean left ventricular diastolic pressure without regard to diastolic duration. Therefore, in contrast to theoretical expectation, diastolic duration is not a practically important determinant and of MBF. A number of DPTI/STTI ratios fell far below the critical values reported in the literature, but they were never associated with the occurrence of subendocardial ischemia, infarction, depressed cardiac performance or myocardial edema
Zusammenfassung
Das Verhältnis von DPTI/STTI zur Abschätzung der myokardialen O2-Versorgung und die Voraussage der Myokarddurchblutung (MBF) über den diastolischen Druck-Zeit-Index (DPTI) und andere Indizes sind an intakten Hunden geprüft worden. Wir analysierten 89 Steady-states bei maximaler Variation der Determinanten von DPTI und STTI. Die MBF wurde über einen Druckdifferenzkatheter im Sinus coronarius gemessen. Alle Experimente erfolgten bei maximaler Koronardilatation (Dipyridamol). Für breite Variationen von Hämodynamik und MBF kamen latation (Dipyridamol). Für breite Variationen von Hämodynamik und MBF kamen ein intraaortaler Sperrballon, Inotropiestimulation, β-Blockade, Hypo- und Hypervolämie, Elektrostimulation und Hämodilution zum Einsatz. Dabei wurden bewußt klinisch relevante Bilder — wie eine tachykarde Herzinsuffizienz bei erschöpfter Koronarreserve — simuliert. Als Kontrollen einer ausreichenden O2-Versorgung dienten koronarvenöse O2-Sättigung, Elektrokardiographie, Ventrikelfunktion Sektionsergebnis und Ödembildung.
Alle Indizes zeigen eine schwache Korrelation zur MBF. Für DPTI errechnet sich ein r von 0,60. Bei Auswertung der Originaldaten vonBuckberg (1) erhalten wir ein analoges Ergebnis (r=0,65) für die Korrelation von DPTI zur subendokardialen Durchblutung. Die beste Korrelation zeigt die Differenz zwischen mittlerem diastolischem Aortendruck und mittlerem diastolischem Ventrikeldruck (r=0,66) ohne Bezug zur Diastolendauer. Danach ist die Diastolendauer in Abweichung von der theoretischen Erwartung keine praktisch wichtige Determinante der MBF. Die alten und auch die neuen kritischen Grenzwerte für DPTI/STTI wurden bei un ohne Gefahren für das Myokard häufig weit unterschritten. Die Aussagekraft des Quotienten scheint demnach stark limitiert zu sein.
Similar content being viewed by others


References
Buckberg, G. D., D. E. Fixler, J. P. Archie, J. I. E. Hoffman: Experimental subendocardial ischemia in dogs with normal coronary arteries. Circulat. Res.30, 67–81 (1972).
Buckberg, G. D., G. N. Olinger, D. G. Mulder, J. V. Maloney, Jr.: Depressed postoperative cardiac performance. Prevention by adequate myocardial protection during cardiopulmonary bypass. J. Thorac. Cardiovasc. Surg.70, 974–988 (1975).
Seybold-Epting, W., G. Fenchel, H. Seboldt, R. Stunkat, H.-E. Hoffmeister: Überwachung der Myokardfunktion nach offenen Herzoperationen durch kontinuierliche Messung des diastolischen und systolischen Druck-Zeit-Index. 72. 7. Jahrestagung der Deutschen Gesellschaft f. Thorax-, Herz-und Gefäßchirurgie in Bad Nauheim, Februar 1978.
Philips, P. A., A. T. Marty, A. M. Miyamoto: A clinical method for detecting subendocardial ischemia after cardiopulmonary bypass. J. Thorac. Cardiovasc. Surg.69, 30–39 (1975).
Baller, D., W. Jonas, H. Sigmund-Duchanova, H. Prennschütz-Schützenau, J. Zipfel, G. Hellige: Examination of the validity of the DPTI as an estimate of myocardial oxygen supply with special reference to the DPTI/TTI ratio. Basic Res. Cardiol.73, 595–606 (1978)
Tauchert, M.: Koronarreserve und maximaler Sauerstoffverbrauch des menschlichen Herzens. Basic Res. Cardiol.68, 183–223 (1973).
Dengler, H. J.: Die therapeutische Anwendung β-sympathikolytischer Stoffe, p. 107 (discussion) (Stuttgart-New York 1972).
Lochner, W.: Regulation der Koronardurchblutung. In:Dengler, H. J. (ed.): Die therapeutische Anwendung β-sympathikolytischer Stoffe, p. 61 (Stuttgart-New York 1972).
Hensel, I., H. J. Bretschneider: Pitot-Rohr-Katheter für die fortlaufende Messung der Koronar- und Nierendurchblutung im Tierexperiment. Arch. Kreislaufforschg.62, 249–292 (1970).
Kreuzer, H., W. Schoeppe: Das Verhalten des Druckes in der Herzwand. Pflügers Arch. ges. Physiol.278, 181 (1963).
Bretschneider, H. J.: Aktuelle Probleme der Koronardurchblutung und des Myocardstoffwechsels, Regensburg. Jb. ärztl. Fortbild. XV,1, 1–27 (1967).
Buckberg, G., J. Brazier: Coronary blood flow and cardiac function during hemodilution In:Messmer, K. andSchmid-Schönbein, H. (ed.): Intentional Hemodilution, Bibl. haemat.,41, 173–189 (Basel 1975).
Hoffman, J. I., G. D. Buckberg: The Myocardial Supply: Demand ratio — A Critical Review. Amer. J. Cardiol.41, 327–332 (1978).
Author information
Authors and Affiliations
Additional information
With 4 figures and 1 table
Supported by the Deutsche Forschungsgemeinschaft, SFB 89, Kardiologie, Göttingen.
Rights and permissions
About this article
Cite this article
Baller, D., Sigmund-Duchanova, H., Zipfel, J. et al. Prediction of myocardial blood flow by DPTI and prediction of the adequacy of myocardial O2 supply by the DPTI/STTI ratio under maximal coronary dilation. Basic Res Cardiol 74, 378–388 (1979). https://doi.org/10.1007/BF01908391
Received:
Issue Date:
DOI: https://doi.org/10.1007/BF01908391