
Abstract
To evaluate the effectiveness of adjuvant immunochemotherapy in advanced adenocarcinoma of the stomach, patients who had undergone radical subtotal gastrectomy for stage III gastric carcinoma were randomized to receive immunochemotherapy or not. For immunotherapy,Streptococcus pyogenes preparation (picibanil) was given intramuscularly every week, and for chemotherapy, either MFC (mitomycin C, 5-fluorouracil, and cytosine arabinoside) regimen or FME (5-fluorouracil and methyl-CCNU) regimen was given. Immunotherapy was started at the fourth or fifth postoperative day and chemotherapy was started at the eighth to tenth postoperative day.
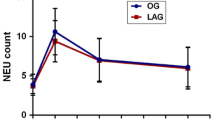
To evaluate the immune status of patients, various immune parameters such as 1-chloro-2, 4-dinitrobenzene (DNCB) test, T-lymphocyte count, PHA- and concanavalin-A-stimulated lymphoblastogenesis, and antibody-dependent cellular cytotoxicity (ADCC) activity were checked before surgery and 3–4 months postoperatively.
One hundred and thirty-eight patients were chosen for study during a 5-year period. Seventy-four patients received postoperative immunochemotherapy and 64 patients received no further anticancer therapy following their operation. All patients had been followed for at least 5 years since they underwent surgery. Survival rate and immune status were compared between the 2 groups. Patient characteristics and preoperative values for the immune status of the 2 groups were similar to each other.
The 5-year survival rate of the postoperative immunochemotherapy group was 44.6%, whereas that of the surgery alone group was 23.4%. The difference is statistically significant (p<0.05). All the postoperative values of immune parameters showed more favorable data in the postoperative immunochemotherapy group.
Postoperative immunochemotherapy is no longer adjuvant, but is an essential systemic therapy to prolong patient survival and cure disease. This author proposes to use the termimmunochemosurgery instead of “surgery and adjuvant immunochemotherapy” for gastric cancer.
Résumé
Dans le souci d'évaluer l'efficacité de l'immunochimiothérapie complémentaire pour traiter le cancer avancé de l'estomac traité par gastrectomie radicale subtotale, les patients ont été sélectionnés au hasard pour être soumis ou non à l'immunochimiothérapie. L'immunothérapie fut effectuée à l'aide de préparations de streptocoques pyogènes (picibanil) administrées chaque semaine et la chimiothérapie par MFC (mitomycine C, 5-FU, et cytosine arabinoside) ou par FME (5-FU et methyl-CCNU). L'immunothérapie fut entreprise 4 ou 5 jours après l'intervention et la chimiothérapie 8 à 10 jour après l'acte opératoire.
Pour apprécier la condition immunologique du malade, différents paramètres immunologiques furent contrôlés avant l'opération et 3–4 mois après l'intervention: 1-chloro-2, 4-dinitrobenzène (DNCB) test, compte des lymphocytes T, PHA et concanavaline A, lymphoblastogénèse stimulée et ADCC.
Cent trente huit malades furent choisis au cours d'une période de 5 ans. Soixante quatorze malades furent traités et soixante quatre ne furent pas soumis à l'immunochimiothérapie. Tous ont été suivis depuis plus de 5 ans. Le taux de survie et la condition immunologique furent comparés entre les 2 groupes. Les valeurs de la condition immunologique et les caractéristiques cliniques des malades étaient identiques.
Le taux de survie à 5 ans après immunochimiothérapie fut de 44.6% et seulement de 23.4% après chirurgie isolée. La différenceest donc statistiquement significative (p<0.05). Toutes les valeurs post-opératoires des paramètres immunologiques furent plus favorables chez les malades du groupe traité par immunochimiothérapie.
Pour l'auteur l'immunochimiothérapie post-opératoire n'est pas seulement un traitement complémentaire mais une méthode essentielle de traitement général permettant de prolonger la vie des malades et d'envisager la guérison. Il propose d'employer le terme d'immuno-chimio-chirurgie au lieu de celui de chirurgie associée à l'immunochimiothérapie complémentaire.
Resumen
Con el fín de valorar la efectividad de la inmunoquimioterapia adyuvante en el adenocarcinoma avanzado de estómago, se procedió a aleatorizar pacientes que habían sido sometidos a gastrectomía subtotal por carcinoma estado III, para recibir o nó inmunoquimioterapia. Para inmunoquimioterapia se administró una preparación de Streptococcus pyogens (picibanil) por vía intramuscular cada semana, y para quimioterapia se administró un regimen de MFC (mitomicina-C, 5-fluoruracilo, y citosina arabinosida) o de FME (5-fluoruracilo y metil-CCNU). La inmunoterapia fue iniciada en el cuarto o quinto día postoperatorio y la quimioterapia en el octavo al décimo día postoperatorio.
Para la valoración del estado inmunológico de los pacientes se determinaron diversos parámetras, tales como la prueba de 1-cloro-2,4-dinitrobenceno (DNCB), el recuento de linfocitos-T, la linfoblastogenesis estimulada por PHA- y concanavalina-A, y la actividad citotóxica celular dependiente de anticuerpos (ADCC), antes de la operación y 3 a 4 meses después de la operación.
Ciento treinta y ocho pacientes fueron escogidos para el estudio en el curso de un periodo de 5 años. Setenta y cuatro pacientes recibieron inmunoquimioterapia postoperatoria y 64 pacientes no recibieron terapia anticancerosa después de la operación. Todos han sido seguidos por no menos de 5 años después de la cirugía. Se compararon las tasas de supervivencia y el estado inmunológico en los 2 grupos. Las características de los pacientes y los valores preoperatorios del estado inmunológico fueron similares en los 2 grupos.
La tasa de supervivencia a 5 años en el grupo de inmunoquimioterapia postoperatoria fue de 44.6%, en tanto que la de la del grupo de cirugía solamente fue de 23.4%. Esta diferencia es estadísticamente significativa (p<0.05). Todos los valores de los parámetros inmunológicos mostraron datos más favorables en el grupo de inmunoquimioterapia postoperatoria.
La inmunoquimioterapia postoperatoria ya no es de carácter adyuvante sino una forma esencial de terapia sistémica para lograr una prolongación de la supervivencia y para curar la enfermedad. El autor propone utilizar el término “inmunoterapia adyuvante” en el manejo del cáncer gástrico.
Similar content being viewed by others


References
Lee, C.K., Lee, S.K., Kim, S.I., Ham, E.K., Kim, Y.I., Kwon, E.H., Kim, D.S., Lee, Y.B., Kim, K.H.: Study on malignant tumors among Koreans based on biopsy and autopsy materials. Korean J. Pathol.2[Suppl.]:1, 1968
Hoerr, S.O.: Prognosis for carcinoma of the stomach. Surg. Gynecol. Obstet.137:205, 1973
Lee, S.K., Chi, J.G., Kim, S.I., Ham, E.K., Kim, Y.I., Cho, H.I., Ahn, G.H.: Malignant tumors among Koreans—Relative frequency study on 7363 cancers during 1968 to 1977. Korean J. Pathol.13:3, 1979
Central Cancer Registry, Ministry of Health, Republic of Korea: Three years report for cancer register programme in the Republic of Korea. July 1980–June 1983. J. Korean Cancer Res. Assoc.16:73, 1984
Kim, J.P., Park, J.G.: The end-results of surgical treatment of gastric cancer. J. Korean Med. Assoc.26:637, 1983
Buchholtz, T.W., Welch, C.E., Malt, R.A.: Clinical correlates of resectability and survival in gastric carcinoma. Ann. Surg.188:711, 1978
The Gastrointestinal Tumor Study Group: A comparative clinical assessment of combination chemotherapy in the management of advanced gastric carcinoma. Cancer49:1362, 1982
Kennedy, B.J.: TNM classification for stomach cancer. Cancer26:971, 1970
Weed, J.E., Nuessle, W., Ochsner, A.: Carcinoma of the stomach. Why are we failing to improve survival? Ann. Surg.193:407, 1981
The Japanese Gastric Cancer Study Group: Gastric cancer registry in Japan—5-year survival rate of cases between 1963 and 1966. Jpn. J. Cancer Clin.27:543, 1981
Taguchi, T., Mattori, T., Inoue, K., Kondo, T., Itoh, I., Kikuchi, K., Suhi, S., Inokuchi, K.: Multihospital randomized study on adjuvant chemotherapy with mitomycin ± futraful for gastric cancer. In Adjuvant Therapy of Cancer II, S.E. Jones, S.E. Salmon, editors, New York, Grune & Stratton, 1979, pp. 581–586
Livstone, E.M., Stablein, D.M.: Adjuvant chemotherapy with 5-FU and methyl CCNU prolongs recurrence free interval and survival following curative resection for gastric adenocarcinoma. Gastroenterology80:1215, 1981
Ota, K., Kurita, S., Nishimura, M., Ogawa, N., Kaneī, Y., Imaī, K., Arīyoshī, Y., Kataoka, K., Murakamī, N., Oyana, A., Hoshīno, A., Ano, H., Kato, T.: Combination therapy with mitomycin-C, 5-fluorouracil and cytosine arabinoside for advanced cancer in man. Cancer Chemother. Rep.56:373, 1972
Moertel, C.G., Mittelman, J.A., Bakemeier, R.F., Engstrom, P., Hanley, J.: Sequential and combination chemotherapy of advanced gastric cancer. Cancer38:678, 1976
Mathé, G., Amiel, J.L., Schwarzenberg, L., Schneider, M., Cattan, A., Schlumberger, J.R., Hayat, M., De Vassal, F.: Active immunotherapy for acute lymphoblastic leukemia. Lancet1:697, 1969
Morton, D.L., Malmgren, R.A., Holmes, E.C., Ketcham, A.S.: Demonstration of antibodies against malignant melanoma by immunofluorescence. Surgery64:233, 1968
Powles, R.O., Crowther, D., Bateman, C.J.T., Beard, M.E.J., McElwain, T.J., Russell, J., Lister, T.A., Whitehouse, J.M.A., Wrigley, P.F.M., Pike, M., Alexander, P., Hamilton Fairly, G.: Immunotherapy for acute myelogenous leukemia. Br. J. Cancer28:365, 1973
Gutterman, J.U., Cardenas, J.O., Blumenschein, G.R., Hortobagyi, G., Burgess, M.A., Livingston, R.B., Mavligit, G.H., Freireich, E.J., Gottlieb, J.A., Hersh, E.M.: Chemoimmunotherapy of advanced breast cancer: Prolongation of remission and survival with BCG. Br. Med. J.2:1222, 1976
Morton, D.L., Eilber, F.R., Malmgren, R.A., Wood, W.C.: Immunological factors which influence the response to immunotherapy in malignant melanoma. Surgery68:158, 1970
Gutterman, J.U., Mavligit, G.M., Blumenshein, G., Burgess, M.A., McBride, C.M., Hersh, Z.M.: Immunotherapy of human solid tumors with BCG: Prolongation of disease free interval and survival in malignant melanoma, breast and colorectal cancer. Ann. N.Y. Acad. Sci.277:135, 1976
Hoerni, B., Chauvergne, J., Hoerni, S.G.: BCG in the immunotherapy of malignant lymphomas. Current results of a controlled trial. Cancer Immunol. Immunother.3:57, 1977
Richman, S.P., Livingston, R.B., Gutterman, J.U., Suen, J.Y., Hersh, E.M.: Chemotherapy versus chemoimmunotherapy of head and neck cancer: Report of a randomized study. Cancer Treat. Rep.60:353, 1976
Wanebo, H.J., Hilal, E.Y., Pinsky, C.M., Strong, E.W., Mike, V., Hirshaut, Y., Oettgen, H.F.: Randomized trial of levamisole in patients with squamous cancer of the head and neck: A preliminary report. Cancer Treat. Rep.62:1663, 1978
Alberts, D.S.: Adjuvant immunotherapy with BCG of advanced ovarian cancer: A preliminary report. In Adjuvant Therapy of Cancer, S.E. Salmon, S.E. Jones, editors, Proceedings in the International Conference on the Adjuvant Therapy of Cancer, Amsterdam, North Holland, 1977, pp. 327–334
Necheles, T.F.: MER/BCG in the treatment of disseminated neuroblastoma. Proc. Am. Soc. Clin. Oncol.17[c-86]:258, 1976
Hattori, T., Mori, A., Hirata, K., Ito, I.: Five-year survival rate of gastric cancer patients treated by gastrectomy, large dose of mitomycin-C and/or allogeneic bone marrow transplantation. Gann63:517, 1972
Okudaira, Y., Sugimachi, K., Inokuchi, K., Kai, H., Kuwano, H., Matsuura, H.: Postoperative long-term immunochemotherapy for esophageal carcinoma. Jpn. J. Surg.12:249, 1982
Kim, J.P., Yoo, I.H.: Relationship between the advance of stomach cancer and the change in immunity. J. Korean Surg. Soc.20:195, 1978
Chun, S.H., Yoo, I.H., Kim, J.P.: The significance of the measurement of immunosuppressive acid protein (IAP) in various cancer patients. Korean J. Immunol.6:31, 1984
Orita, K., Miwa, H., Fukuda, H., Yumora, M., Uehida, Y., Mamnamī, T., Konaga, Z., Tanaka, S.: Preoperative cell-mediated immune status of gastric cancer patient. Cancer38:2343, 1976
Lauren, P.: The two histological main types of gastric carcinoma: Diffuse and so-called intestinal type carcinoma. An attempt at a histoclinical classification. Acta Pathol. Microbiol. Scand.64:31, 1965
Kim, J.P., Choi, W.J.: A study on histologic type of gastric carcinoma: Analysis of clinico pathologic characterization and its implication as a prognostic factor. J. Korean Cancer Res. Assoc. (in press)
Kim, J.P., Jung, S.E.: Staging patients with gastric cancer and their prognosis. J. Korean Cancer Res. Assoc.18:9, 1986
Blake, J.R.S., Hardcastle, J.D., Wilson, R.G.: Gastric cancer: A controlled trial of adjuvant chemotherapy following gastrectomy. Clin. Oncol.7:13, 1981
Serlin, O., Keehn, R.J., Higgins, G.A., Jr., Harrower, H.W., Mendeloff, G.L.: Factors related to survival following resection for gastric carcinoma. Analysis of 903 cases. Cancer40:1318, 1977
The Gastrointestinal Tumor Study Group: Controlled trial of adjuvant chemotherapy following curative resection of gastric cancer. Cancer49:1116, 1982
MacDonald, J.S., Schein, P.S., Woolley, P.V., Smythe, T., Ueno, W., Hoth, D., Smith, F., Boiron, M., Gisselbrecht, C., Brunet, R., Lagarde, C.: 5-fluorouracil, doxorubicin, and mitomycin (FAM) combination chemotherapy for advanced gastric cancer. Ann. Intern. Med.93:533, 1980
Bitran, J.D., Desser, R.K., Kozloff, J.F., Billings, A.A., Shapero, C.M.: Treatment of metastatic pancreatic and gastric adenocarcinoma with fluorouracil, adriamycin, and mitomycin-C (FAM). Cancer Treat. Rep.63:2049, 1979
The Gastrointestinal Tumor Study Group: Phase II–III chemotherapy study in advanced gastric cancer. Cancer Treat. Rep.63:1871 1979
Holland, J.F., Bekesi, J.G., Cuttner, J., Glidewell, O.: Chemoimmunotherapy in acute myelocytic leukemia. Isr. J. Med. Sci.13:694, 1977
Rodriguez, V., Bodey, G.P., Freireich, E.J., McCredie, K.B., Gutterman, J.U., Keating, M.J., Smith, T.L., Gehan, E.A.: Randomized trial of protected environment prophylactic antibodies in 145 adults with acute leukemia. Medicine57:253, 1978
Pouillart, P., Palangie, T., Schwarzenberg, L., Brugerīe, H., Lherītier, J., Mathe, G.: Effect of BCG on hematopoietic stem cells. Biomedicine23:469, 1975
Makowka, J., Falk, R.E., Ambus, U., Bugala, R., Landi, S.: Adjuvant chemoimmunotherapy for gastric carcinoma. Can. J. Surg.23:429, 1980
Suga, S., Tsunekawa, H., Washino, M.: Treatment of gastric cancer, with special reference to the survivals of the cancer patients treated with multiple combination MFC therapy or immunochemotherapy of MFC plus OK-432 (NSC B116209). Gastroenterol. Jpn.12:20, 1977
Gunduz, N., Fisher, B., Saffer, E.A.: Effect of surgical removal on the growth and kinetics of residual tumor. Cancer Res.39:3861, 1979
Nissen-Meyer, R., Kjellgren, K., Malmio, K., Mansson, B., Norin, T.: Surgical adjuvant chemotherapy: Results with one short course with cyclophosphamide after mastectomy for breast cancer. Cancer41:2088, 1978
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Kim, J.P. The concept of immunochemosurgery in gastric cancer. World J. Surg. 11, 465–472 (1987). https://doi.org/10.1007/BF01655811
Issue Date:
DOI: https://doi.org/10.1007/BF01655811