
Abstract
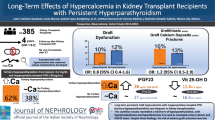
In an attempt to find out if a particular group of patients with hyperparathyroidism after renal transplantation (HRT) are at risk of developing complications, 14 patients with overt untreated HRT who had at least 1 serum calcium determination ≥ 12 mg/100 ml were evaluated and compared retrospectively with 11 normocalcemic transplant recipients at 6 and 30± 8 months after successful renal allografting. Serum calcium was ≥ 12 mg/100 ml within 6 months of transplantation in 13 of the 14 HRT patients. At 6 months significant differences were found between HRT and controls in mean serum calcium (11.6 versus 9.2 mg/100 ml) and alkaline phosphatase (228 versus 120 U/l). At 30±8 months differences were found in serum calcium (10.2 versus 9.4 mg/100 ml), phosphate (2.8 versus 4.8 mg/100 ml), and alkaline phosphatase (180 versus 88 U/l). Serum creatinine levels were similar in the 2 groups. A significant correlation was found between early and late determinations of alkaline phosphatase when all 25 patients were studied as a single group (r=0.72, p<0.001). Bone pain and/or radiological evidence of hyperparathyroid bone disease were significantly associated with HRT (8 versus 1 and 7 versus 0, respectively). A higher but not significant incidence of vascular calcifications (5 versus 1) and acute pancreatitis (2 versus 0) was found in HRT. Patients who develop moderate to severe HRT as defined by at least 1 serum calcium determination ≥ 12 mg/100 ml do so within 6 months of renal transplantation, have increased morbidity, particularly involving the skeleton, and might benefit from early subtotal parathyroidectomy.
Résumé
Dans le but de déterminer les risques de complications chez un groupe de malades ayant présenté un hyperparathyroïdisme après transplantation rénale les auteurs ont comparé une série de 14 cas où le taux de calcium avait été au moins une fois supérieure à 12 mg/100 ml et une série de 11 receveurs où le taux de calcium était normal et ce 6 et 30±8 mois après allogreffe rénale. Au bout de 6 mois le taux de calcium fut supérieur à 12 mg/100 ml chez 13 des 14 malades qui avaient subi une transplantation rénale. Des différences significatives furent constatées entre les transplantés et les sujets appartenant au groupe de contrôle aussi bien en ce qui concerne le calcium sérique (11.6 contre 9.2 mg/100 ml) et la phosphatase alcaline (228 contre 120 U/l). Au terme de 30±8 mois des différences furent également constatées pour le calcium (10.2 contre 9.4 mg/100 ml), pour le phosphore (2.8 contre 4.8 mg/100 ml) et pour la phosphatase alcaline (180 contre 88 U/l). Les taux de créatinine sérique étaient identiques dans les 2 groupes. Une corrélation significative fut constatée entre les déterminations précoces et tardives de la phosphatase alcaline chez les 25 sujets rassemblés en un seul groupe (r=0.72, p<0.001). La douleur osseuse et/ou des signes radiologiques évidents d'atteinte osseuse d'origine hyperparathyroïdienne allaient de pair significativement chez les transplantés (8 contre 1 et 7 contre 0 respectivement). Chez ceux-ci fut constatée une fréquence supérieure mais non significative de calcifications vasculaires (5 contre 1) et de pancréatite aiguë (2 contre 0). Les opérés qui ont développé un hyperparathyroïdisme modéré ou intense (un taux supérieur à 12 mg/100 ml, au moins une fois) au cours des 6 mois qui suivirent la transplantation rénale, en particulier lorsqu'ils présentèrent une atteinte du squelette, devraient bénéficier d'une parathyroïdectomie subtotale.
Resumen
Con el propósito de determinar si el grupo particular de pacientes con hiperparatiroidismo después de transplante renal (HTR) posee riesgo de desarrollar complicaciones, se realizó la evaluación de 14 casos definidos de HTR no tratados y que presentaban por lo menos un valor de calcio sérico ≥ 12 mg/100 ml, los cuales fueron comparados con 11 recipientes normocalcémicos de transplante renal a los 6 y 30 ±8 meses después de un aloinjerto renal exitoso. El calcio sérico apareció en ≥ 12 mg/100 ml dentro de los primeros 6 meses de efectuado el transplante en 13 de 14 pacientes con HTR. A los 6 meses se hallaron diferencias significativas entre los pacientes con HTR y los controles en el valor promedio del calcio sérico (11.6 vs. 9.2 mg/100 ml) y de la fosfatasa alcalina (228 vs. 120 U/l). A los 30±8 meses se hallaron diferencias en el calcio sérico (10.2 vs. 9.4 mg/100 ml), fosfato (2.8 vs. 4.8 mg/100 ml) y fosfatasa alcalina (180 vs. 88 U/l). Los niveles de creatinina sérica aparecieron similares en los 2 grupos. Se encontró una correlación significativa entre las determinaciones tempranas y las tardías de la fosfatasa alcalina cuando la totalidad de los 25 pacientes fue estudiada como grupo único (r= 0.72, p<0.001). El dolor óseo y/o la evidencia radiológica de enfermedad ósea paratiroidea aparecieron en asociación significativa con el HTR (8 vs. 1 y 7 vs. 0, respectivamente). Una incidencia mayor, aunque no significativa, de calcificaciones vasculares (5 vs. 1) y de pancreatitis aguda (2 vs. 0) fue hallada en el HTR. Los pacientes con HTR severo definido como el hallazgo de por lo menos una determinación de calcio sérico ≥ 12 mg/100 ml, lo desarrollan dentro de los 6 meses siguientes al transplante renal, presentan morbilidad aumentada, especialmente con afección esquelética, y es posible que se beneficien de paratiroidectomía subtotal.
Similar content being viewed by others


References
Alfrey, A.C., Jenkins, D., Groth, C.G., Schorr, W.S., Gecelter, L., Ogden, D.A.: Resolution of hyperparathyroidism, renal osteodystrophy and metastatic calcification after renal homotransplantation. N. Engl. J. Med.271:1349, 1968
Diethelm, A.G., Edwards, R.P., Whelchel, J.D.: The natural history and surgical treatment of hypercalcemia before and after renal transplantation. Surg. Gynecol. Obstet.154:481, 1982
Blohmé, I., Eriksson, A.: Parathyroidectomy after renal transplantation. Scand. J. Urol. Nephrol. [Suppl.]42:134, 1977
Normann, E., Fryjordet, A., Halvorsen, S.: Stones in renal transplants. Scand. J. Urol. Nephrol.14:73, 1980
Sitges-Serra, A., Esteller, E., Ricart, M.J., Caralps, A.: Indications and late results of subtotal parathyroidectomy for hyperparathyroidism after renal transplantation. World J. Surg.8:534, 1984
David, D.S., Sakai, S., Brennan, B.L., Riggio, R.A., Cheigh, J., Stenzel, K.H., Rubin, A.L., Sherwood, L.M.: Hypercalcemia after renal transplantation. Long-term follow-up data. N. Engl. J. Med.289:398, 1973
McPhaul, J.J., McIntosh, D.A., Hammond, W.S., Park, O.K.: Autonomous secondary (renal) parathyroid hyperplasia. N. Engl. J. Med.271:1342, 1964
Wibell, L., Grimelius, L., Johansson, H.: Explorative parathyroidectomy before and after kidney transplantation. Scand. J. Urol. Nephrol. [Suppl.]42:153, 1977
Geis, W., Popovtzer, M.M., Corman, J.L., Halgrimson, C.G., Groth, C.G., Starzl, T.E.: The diagnosis and treatment of hyperparathyroidism after renal homotransplantation. Surg. Gynecol. Obstet.137:997, 1973
Sivula, A., Kuhlbäck, B., Kock, B., Kahri, A., Wallenius, M., Edgren, J.: Parathyroidectomy in chronic renal failure. Acta Chir. Scand.145:19, 1979
Hognestad, J., Flatmark, A.: Hyperparathyroidism in uremia and after kidney transplantation. Scand. J. Urol. Nephrol. [Suppl.]42:137, 1977
Lundgren, G., Asaba, M., Magnusson, G., Pieper, R., Alveryd, A.: The role of parathyroidectomy in the treatment of secondary hyperparathyroidism before and after renal transplantation. Scand. J. Urol. Nephrol. [Suppl.]42:149, 1977
Christensen, M.S., Nielsen, H.E.: The clinical significance of hyperparathyroidism after renal transplantation. Scand. J. Urol. Nephrol. [Suppl.]41:130, 1977
Pieper, R., Alveryd, A., Lundgren, G., Collste, H., Magnusson, G., Svahn, T., Groth, C.G.: Secondary hyperparathyroidism and its sequelae in renal transplant recipients. Scand. J. Urol. Nephrol. [Suppl.]42:144, 1977
Chatterjee, S.N., Friedler, R.M., Bernes, T.V., Oldham, S.B., Singer, F.R., Massry, S.G.: Persistent hypercalcemia after successful renal transplantation. Nephron17:1, 1976
Lins, L.E.: Renal function in hypercalcemia after renal transplantation. Scand. J. Urol. Nephrol. [Suppl.]42:159, 1977
Malmaeus, J., Akerström, G., Johansson, H., Ljunghall, S., Nilsson, P., Selking, O.: Parathyroid surgery in chronic renal insufficiency. Acta Chir. Scand.148:229, 1982
Salinas Payer, J.C., Mendez Picon, G., Lee, H.M.: Complicaciones gastrointestinales y biliopancreáticas tras el transplante renal. Med. Clin. (Barcelona)82:195, 1984
Penn, I., Durst, A.L., Machado, M., Halgrimson, C.G., Bouth, A.S., Jr., Putnam, C.W., Groth, C.G., Starzl, T.E.: Acute pancreatitis and hyperamylasemia in renal homograft recipients. Arch. Surg.105:167, 1972
Meyers, W.C., Harris, N., Stein, S., Brooks, M., Jones, R.C., Thompson, W.C, Stickel, D.L., Seigler, H.F.: Alimentary tract complications after renal transplantation. Ann. Surg.190:535, 1979
Mallory, A., Kern, F., Jr.: Drug-induced pancreatitis: A critical review. Gastroenterology78:813, 1980
Author information
Authors and Affiliations
Additional information
Supported by a grant from the Fondo de Investigaciones Sanitarias de la Seguridad Social. Ministerio de Sanidad, Spain.
Rights and permissions
About this article
Cite this article
Sitges-Serra, A., Gores, P., Hesse, U. et al. Serum calcium as an early indicator for surgical treatment of hyperparathyroidism after renal transplantation. World J. Surg. 10, 661–666 (1986). https://doi.org/10.1007/BF01655550
Issue Date:
DOI: https://doi.org/10.1007/BF01655550