
Summary
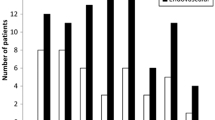
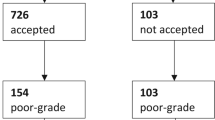
In a retrospective study the clinical management of 74 patients with aneurysmal subarachnoid haemorrhage (SAH) admitted in grade IV and V Hunt and Hess was examined. 39 patients (53%) were admitted within 24 hours after SAH, 29 patients (39%) between 24 and 72 hours after SAH, and 6 patients 8%) later than this time interval. The ruptured aneurysms were located at the anterior communicating artery complex in 34 patients (46%), on the middle cerebral artery in 19 patients (26%), on the internal carotid artery in 12 patients (16%) and at the vertebro-basilar artery complex in 9 patients (12%). In 38 patients (51%) no surgical attack on the aneurysm was performed. 19 (50%) of these patients were in grade IV on admission and 19 (50%) in grade V. In 36 patients (49%) the aneurysm was clipped. Of these patients 29 (81%) were in grade IV and 7 (19%) in grade V. Of the 38 patients in whom no aneurysm surgery was done, 37 patients died, representing a mortality rate of 97%, one patient survived in grade III Glasgow Outcome Scale (GOS). Concerning the outcome in those patients with aneurysm clipping, of 19 patients in grade IV operated on early, 10 patients (53%) made a good recovery, 3 (16%) were left severely disabled and 6 patients (31%) remained in a vegetative state or died. Of the 10 patients in grade IV with delayed surgery 4 (40%) were in grade I and II postoperatively, 2 (20%) in grade III, and again 4 (40%) in grade IV and V GOS. None of the 4 patients in Hunt and Hess grade V in whom early surgery was done achieved a good postoperative outcome. 2 patients survived in grade III GOS, and another 2 patients died. Only three patients admitted in grade V survived long enough to be subjected to delayed surgery. Of these patients one survived without deficit, one survived severely disabled and one patient died.
From the data presented the following conclusions are drawn: 1. Without surgery the chance of survival in poor-grade aneurysm patients is almost non existent 2. Patients admitted in grade V have a uniformly poor prognosis with a very high mortality whether surgery is done or not, and whether surgery is performed early or late. 3. Patients in grade IV represent a distinct group with a better prognosis than those in grade V, justifying an aggressive surgical management. 4. Early surgery in grade IV patients leads to better results than delayed surgery especially in terms of overall management morbidity and mortality. 5. In order to further improve the results of management of poor-grade aneurysm patients early referral to neurosurgical centres is mandatory.
Similar content being viewed by others

References
Auer LM (1984) Acute operation and preventive nimodipine improve outcome in patients with ruptured cerebral aneurysms. Neurosurgery 15: 57–66
Auer LM, Brandt L, Ebeling U, Gilsbach J, Groeger U, Harders A, Ljunggren B, Oppel F, Reulen HJ, Saeveland H (1986) Nimodipine and early aneurysm operation for good condition SAH patients. Acta Neurochir (Wien) 82: 7–13
Bailes JE, Spetzler RF, Hadley MN, Baldwin HZ, Zabramski JM (1989) Management morbidity and mortality of Hunt and Hess Grades IV and V aneurysm patients. (Abstract) Second International Workshop on Intracranial Aneurysms, Nagoya, Japan, p 151
Bonita R, Thomson S (1985) Subarachnoid haemorrhage: epidemiology, diagnosis, management and outcome. Stroke 16: 591–594
Deruty R, Patet JD, Mottolese C, Honorato D (1986) Outcome of ruptured intracranial aneurysms treated by a deferred operation. Neurol Res 8: 183–186
Disney L, Weir B, Grace M (1988) Factors influencing the outcome of aneurysm rupture in poor grade patients: A prospective series. Neurosurg 23: 1–9
Flamm E (1985) The timing of aneurysm surgery 1985. Clin Neurosurg 33: 147–158
Fortuny LA, Adams CBT, Briggs M (1980) Surgical mortality in an aneurysm population: effects of age, blood pressure and properative neurological state. J Neurol Neurosurg Psychiatry 43: 879–892
Gilsbach JM, Harders AG, Eggert HR, Hornyak ME (1988) Early aneurysm surgery: A 7 year clinical practice report. Acta Neurochir (Wien) 90: 91–102
Gilsbach JM, Harders AG (1989) Morbidity and mortality after early aneurysm surgery-aprospective study with nimodipine prevention. Acta Neurochir (Wien) 96: 1–7
Hunt WE, Hess RM (1968) Surgical risk as related to time of intervention in the repair of intracranial aneurysm. J Neurosurg 28: 14–19
Inagawa T, Takahashi M, Hidenobu A, Ishikawa S, Yoshimoto H (1988) Aneurysmal subarachnoid hemorrhage in Izumo City and Shimane prefacture of Japan — Outcome. Stroke 19: 176–181
Jennett B, Bond M (1975) Assessment of outcome after severe brain damage. Lancet I: 480–484
Kassell N, Boarini D, Adams H, Sahs A, Graf C, Torner J, Gerk M (1981) Overall management of ruptured aneurysm: Comparison of early and late operation. Neurosurg 9: 120–128
Koos WT, Perneczky A (1982) Timing of surgery for ruptured aneurysms — Experience from 800 consecutive cases. Acta Neurochir (Wien) 63: 124–133
Ljunggren B, Brandt L (1985) Timing of aneurysm surgery. Clin Neurosurg 33: 159–175
Ljunggren B, Säveland H, Brandt L, Zygmunt S (1985) Early operation and overall outcome in aneurysmal subarachnoid hemorrhage. J Neurosurg 62: 547–551
Milhorat T, Krautheim M (1986) Results of early and delayed operations for ruptured aneurysms in two series of 100 consecutive patients. Surg Neurol 26: 123–128
Petruk KC, West M, Mohr G, Weir BKA, Benoit BG, Gentili F, Disney L, Khan MI, Grace M, Holness RO, Karwon MS, Ford RM, Cameron GS, Tucker WS, Purves GB, Miller JDR, Hunter KM, Richard MT, Durity FA, Chan R, Clein LJ, Maroun FB, Godon A (1988) Nimodipine treatment in poor grade aneurysm patients. Results of a multicenter double-blind placebo-controlled trial. J Neurosurg 68: 505–517
Rasmussen P, Busch H, Haase J, Hansen J, Harmsen A, Knudsen V, Marcussen E, Midholm S, Olsen RB, Rosenorn J, Schmidt K, Voldby B, Hansen L (1980) Intracranial saccular aneurysms. Results of treatment in 851 patients. Acta Neurochir (Wien) 53: 1–17
Seifert V, Stolke D, Trost HA (1988) Timing of Aneurysm Surgery: Comparison of operative results of early and delayed operative intervention. Europ Arch Psychiat Neurol Sciences 237: 291–297
Seifert V, Künnecke St, Stolke D (1988) Decision-making in surgery for primary intracerebral hematomas from aneurysm rupture. Theoretical Surgery 3: 83–88
Seiler RW, Reulen HJ, Huber P, Grolimund P, Ebeling U, Steiger HJ (1988) Outcome of aneurysmal subarachnoid haemorrhage in a hospital population: A prospective study including early operation, intravenous nimodipine, and transcranial doppler ultrasound. Neurosurg 23: 598–604
Sundt TM, Kobayashi S, Fode N, Whisnant J (1982) Results and complications of surgical management of 809 intracranial aneurysms in 722 cases. J Neurosurg 56: 753–756
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Seifert, V., Trost, H.A. & Stolke, D. Management morbidity and mortality in grade IV and V patients with aneurysmal subarachnoid haemorrhage. Acta neurochir 103, 5–10 (1990). https://doi.org/10.1007/BF01420185
Issue Date:
DOI: https://doi.org/10.1007/BF01420185