
Summary
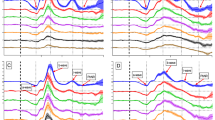
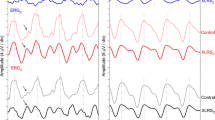
In young children, the ERG is characterized by reduced amplitudes of the a- and b-waves. The photopic and the scotopic components do not always follow the same pattern. Many records are characterized by a photopic predominance (b 1-wave), which would suggest an atypical hemeralopia. Flicker ERG gives similar results as in adults, when using high intensity flashes. With low intensity flashes, however, the results are dissimilar and the dispersion is greater in children than in adults.
As the determination of the critical fusion frequency is not always possible for technical reasons, we have compared the amplitude of the b-wave for different frequencies. For low frequencies, the normal dispersion is great in young children. But a very good superimposition of the curves can be obtained when:
-
1)
an intensity is chosen which gives the same type of ERG (arbitrarily we have taken an ERG characterized by an a-wave of 100 μV), and
-
2)
the amplitudes of the b-waves are plotted in relative values (percentage of the amplitude of a dark adapted single stimulus ERG).
In young children, the mean values obtained with high intensity flashes are very similar.
Résumé
Chez les jeunes enfants, l'ERG est caractérisé par une diminution de l'amplitude des ondes a et b. Les composantes photopiques et scotopiques ne suivent pas toujours la même évolution. De nombreux tracés sont caractérisés par une prédominance photopique (onde b 1), ce qui pourrait suggérer une héméralopie atypique. Le “flicker” ERG donne des résultats analogues à ceux de l'adulte, lorsqu'on utilise des stimuli de forte intensité. Par contre les stimuli de faible intensité donnent des résultats dissemblables et la dispersion est plus grande chez les enfants que chez les adultes.
Comme on ne peut pas toujours déterminer la fréquence critique de fusion pour des raisons techniques, nous avons comparé l'amplitude de l'onde b pour différentes fréquences. Pour les fréquences basses, la dispersion normale est grande chez les jeunes enfants. On peut cependant obtenir une bonne superposition des courbes, à condition de:
-
1.
Choisir une intensité de stimulation, qui donne le même type d'ERG (nous avons pris arbitrairement un ERG caractérisé par une onde a de 100 μV).
-
2.
Transposer l'amplitude des ondes b en valeurs relatives (en pourcentages de l'amplitude de l'onde b obtenue par une stimulation unique chez un sujet adapté à l'obscurité).
Les valeurs moyennes obtenues avec un stimulus de forte intensité présentent peu de dispersion chez les jeunes enfants.
Zusammenfassung
Bei jungen Kindern ist das ERG charakterisiert durch eine Verkleinerung der a- und b-Wellen. Die photopischen und scotopischen Komponenten ändern sich nicht immer auf dieselbe Weise. In manchen Registrierungen dominiert das photopische System (b 1-Welle), was das Bestehen einer atypischen Hemeralopie suggerieren könnte.
Flimmerelektroretinographie gibt dieselben Resultate wie in Erwachsenen, wenn man Reize hoher Intensität benutzt. Mit niedrigen Intensitäten bekommt man Resultate, die nicht identisch sind. Die Streuung ist bei Kindern auch grosser als bei Erwachsenen.
Weil die Bestimmung der Flimmerfusionsfrequenz aus technischen Gründen nicht immer möglich war, haben die Autoren die Amplitude der b-Welle gegenseitig verglichen für die verschiedenen Reizfrequenzen. Für niedrige Frequenzen ist die normale Streuung am grössten bei jungen Kindern.
Eine gute Superposition der Kurven kann jedoch erhalten werden, wenn man:
-
1.
eine Intensität wählt, die den gleichen Typ ERG gibt (die Verfasser haben ein beliebiges ERG angenommen das durch eine a-Welle von 100 μV charakterisiert ist), und
-
2.
die Höhe der b-Wellen in relativen Werten gibt (ein Prozentsatz der Höhe des ERGs eines dunkel-adaptierten Auges).
Bei jungen Kindern ist die Streuung der mittleren Werten, die man mit Reizen hoher Intensitäten bekommt, nur klein.
Similar content being viewed by others
References
Francois, J. & deRouck, A. (1960) La réponse électrorétinographique aux stimulations couplées chez les sujets normaux. Ophthalmologica 140, 353–368.
Heck, J. & Zetterström, B. (1958) Analyse des photopischen Flimmerelektroretinogramms bei Neugeborenen. Ophthalmologica 135, 205–210.
Karpe, G. & Zetterström, B. (1958) Congenital Retinal Dysfunction. Amer. J. Ophthal. 45, 249–253.
Schappert-Kimmijser, J. (1958) Value of Electroretinography in Cases of Doubtful Diagnosis in the Blind and Partially Sighted Child. Ophthalmologica 135, 147–154.
Winkelman, J. E. & Horsten, G. P. M. (1959) L'électrorétinogramme du nouveau né. Bull. Soc. franç. Ophtal. 72, 236–241.
Zetterström, B. (1951) The Clinical Electroretinogram IV. The Electroretinogram of Children During the First Year of Life. Acta ophthal. Kbh. 29, 295–299.
Author information
Authors and Affiliations
Additional information
Ophthalmological Clinic of the University.
Rights and permissions
About this article
Cite this article
François, J., de Rouck, A. The electroretinogram in young children (single stimulus, twin flashes and intermittent stimulation). Doc Ophthalmol 18, 330–343 (1964). https://doi.org/10.1007/BF00160585
Issue Date:
DOI: https://doi.org/10.1007/BF00160585