
Abstract
Background
Laparoscopic surgeries are a risk factor for raised intracranial **pressure and neurological complications. Even though rare, the consequences may be severe.
Methods
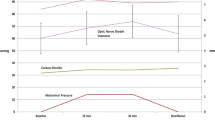
One hundred and one patients of laparoscopic cholecystectomy were enrolled and were randomized into two groups: low-pressure 8 mm Hg (Group A) and high-pressure 14 mm Hg (Group B) carbon dioxide pneumoperitoneum during surgery. Fifty patients were in group A and 51 patients were in group B. Intracranial pressure was measured by measuring the optic nerve sheath diameter (ONSD) using ultrasound examination. Baseline ONSD was recorded followed by ONSD recording at various intervals: at the induction of anesthesia; 30 min, 45 min, at the end of surgery; and 30 min post surgery.
Results
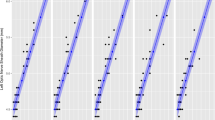
The groups were comparable in terms of demographics and comorbidities. The mean age of group A was 45 years and for group B it was 45.75 years. Most common indication for surgery was symptomatic gall stone disease. Baseline ONSD in group A was 0.427 ± 0.0459 mm, whereas it was 0.412 ± 0.0412 mm in group B. There was a significant rise of ONSD (p < 0.05) 30 min after induction of pneumoperitoneum and up to 30 min post anesthesia. In the low-pressure group 7 (14%) patients had a significant rise of ICP, whereas in the high-pressure group 20 (39%) patients had a significant rise of ICP (p < 0.05).
Conclusions
High-pressure pneumoperitoneum causes significant rise in intracranial pressure in comparison to low-pressure pneumoperitoneum during laparoscopic cholecystectomy, which can be monitored by ONSD measurement by ultrasound examination and is totally non-invasive.
Similar content being viewed by others

References
Soper NJ, Stockmann PT, Dunnegan DL, Ashley SW (1992) Laparoscopic cholecystectomy: the new gold standard. Arch Surg 127(8):917–923
Warttig S, Ward S, Rogers G, Guideline Development Group (2014) Diagnosis and management of gallstone disease: summary of NICE guidance. BMJ 349:6241
Robba C, Cardim D, Donnelly J, Bertuccio A, Bacigaluppi S, Bragazzi N, Cabella B, Liu X, Matta B, Lattuada M, Czosnyka M (2016) Effects of pneumoperitoneum and Trendelenburg position on intracranial pressure assessed using different non-invasive methods. BJA 117(6):783–791
Kalmar AF, Foubert L, Hendrickx JF, Mottrie A, Absalom A, Mortier EP, Struys MM (2010) Influence of steep Trendelenburg position and CO2 pneumoperitoneum on cardiovascular, cerebrovascular, and respiratory homeostasis during robotic prostatectomy. BJA 104(4):433–439
Citerio G, Vascotto E, Villa F, Celotti S, Pesenti A (2001) Induced abdominal compartment syndrome increases intracranial pressure in neurotrauma patients: a prospective study. Crit Care Med 29(7):1466–1471
Rosenthal RJ, Hiatt JR, Phillips EH, Hewitt W, Demetriou AA, Grode M (1997) Intracranial pressure. Surg Endosc 11(4):376–380
Pandey R, Garg R, Darlong V, Punj J, Kumar A (2010) Unpredicted neurological complications after robotic laparoscopic radical cystectomy and ileal conduit formation in steep trendelenburg position: two case reports. Acta Anaesthesiol Belg 61(3):163–166
Kamine TH, Papavassiliou E, Schneider BE (2014) Effect of abdominal insufflation for laparoscopy on intracranial pressure. JAMA Surg 149:380–382
Rosin D, Brasesco O, Varela J et al (2002) Low-pressure laparoscopy may ameliorate intracranial hypertension and renal hypo- perfusion. J Laparoendosc Adv Surg Technol A 12:15–19
Cooke SJ, Paterson-Brown S (2001) Association between laparoscopic abdominal surgery and postoperative symptoms of raised intracranial pressure. Surg Endosc 15:723–725
Lanfranco AR, Castellanos AE, Desai JP, Meyers WC (2004) Robotic surgery: a current perspective. Ann Surg 239(1):14
Robba C, Bacigaluppi S, Cardim D, Donnelly J, Bertuccio A, Czosnyka M (2015) Non-invasive assessment of intracranial pressure. Acta Neurol Scand 32:1587–1597
Strumwasser A, Kwan RO, Yeung L et al (2011) Sonographic optic nerve sheath diameter as an estimate of intracranial pressure in adult trauma. J Surg Res 170:265–271
Kimberly HH, Shah S, Marill K, Noble V (2008) Correlation of optic nerve sheath diameter with direct measurement of intracranial pressure. Acad Emerg Med 15:201–204
Moretti R, Pizzi B (2011) Ultrasonography of the optic nerve in neurocritically ill patients. Acta Anaesthesiol Scand 55:644–652
Robba C, Santori G, Czosnyka M et al (2018) Optic nerve sheath diameter measured sonographically as non-invasive estimator of intracranial pressure: a systematic review and meta-analysis. Intensiv Care Med 44:1284–1294
Ghosh A, Elwell C, Smith M (2012) Review article: cerebral Near-infrared Spectroscopy in adults: a work in progress. Anesth Analg 115:1373–1383
Sridhar R, Gadhinglajkar SV (2003) Pharmacological neuroprotection. Indian J Anaesth 47(1):8–22
Funding
Nil.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
T. Yashwashi, Lileswar Kaman, Kamal Kajal, Divya Dahiya, Ashish Gupta, Shyam C. Meena, Kaptan Singh, and Abhinaya Reddy declare that they have no conflicts of interest or financial ties to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Yashwashi, T., Kaman, L., Kajal, K. et al. Effects of low- and high-pressure carbon dioxide pneumoperitoneum on intracranial pressure during laparoscopic cholecystectomy. Surg Endosc 34, 4369–4373 (2020). https://doi.org/10.1007/s00464-019-07207-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-019-07207-w