
Abstract
Background
There remains a controversy in the literature regarding adequate width of negative surgical margins in breast conservative therapy (BCT). It is now advocated that no tumor on an inked margin is a safe negative margin. Majority of studies on the outcomes of BCT had patients with favorable prognostic factors. Pakistani population has a high expression of unfavorable prognostic factors. The objective of this study was to determine a safe negative margin width in Pakistani population that undergoes BCT.
Methods
A total of 603 patients with identifiable surgical margins underwent BCT from 1997 to 2009 in Shaukat Khanum Cancer Hospital. Patients were divided into close (≤2 mm), free (>2–10 mm), and wide (>10 mm) margin groups. Locoregional recurrence was defined as recurrence within the operated breast, ipsilateral axilla, or supraclavicular or internal mammary lymph nodes. Locoregional recurrence-free survival was calculated from the date of surgery to the date of locoregional recurrence. Five-year locoregional recurrence-free survival was determined for margin groups. Univariate and multivariate Cox proportional hazard analyses were performed to determine independent predictors of locoregional recurrence.
Results
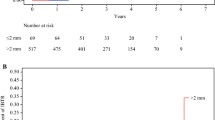
A total of 415 (69 %) patients were <50 years of age. There were 82 (15 %) T3/T4, 337 (56 %) poorly differentiated, and 238 (39 %) ER/PR −ve tumors. Nodal positivity was present in 314 (52 %) patients. The actual number of locoregional recurrences was 16 (12 %), 8 (3 %), and 10 (4.6 %), respectively (P = 0.002). Expected 5-year locoregional recurrence-free survival was 90, 97, and 96 %, respectively (P = 0.002). On multivariate analysis, tumor size, nodal involvement, and negative margin width were independent predictors of locoregional recurrence.
Conclusion
A negative margin width of 2 mm might represent an adequate negative margin width in the Pakistani population undergoing breast conservative therapy.

Similar content being viewed by others


References
Fisher B, Anderson S, Bryant J et al (2002) Twenty-year follow-up of a randomized trial comparing total mastectomy, lumpectomy, and lumpectomy plus irradiation for the treatment of invasive breast cancer. N Engl J Med 347:1233–1241
Van Dongen JA, Voogd AC, Fentiman IS et al (2000) Long-term results of a randomized trial comparing breast-conserving therapy with mastectomy: European Organization for Research and Treatment of Cancer 10801 trial. J Natl Cancer Inst 92:1143–1150
Kreike B, Hart AA, van de Velde T et al (2008) Continuing risk of ipsilateral breast relapse after breast-conserving therapy at long-term follow-up. Int J Radiat Oncol Biol Phys 71:1014–1021
Komoike Y, Akiyama F, Iino Y et al (2006) Ipsilateral breast tumor recurrence (IBTR) after breast-conserving treatment for early breast cancer: risk factors and impact on distant metastases. Cancer 106:35–41
Nottage MK, Kopciuk KA, Tzontcheva A et al (2006) Analysis of incidence and prognostic factors for ipsilateral breast tumour recurrence and its impact on disease-specific survival of women with node-negative breast cancer: a prospective cohort study. Breast Cancer Res 8:R44
Bijker N, Peterse JL, Duchateau L et al (2001) Risk factors for recurrence and metastasis after breast-conserving therapy for ductal carcinoma-in-situ: analysis of European Organization for Research and Treatment of Cancer Trial 10853. J Clin Oncol 19:2263–2271
Jobsen JJ, Van Der Palen J, Ong F et al (2007) Differences in outcome for positive margins in a large cohort of breast cancer patients treated with breast-conserving therapy. Acta Oncol 46:172–180
Arriagada R, Lê MG, Guinebretière JM et al (2003) Late local recurrences in a randomised trial comparing conservative treatment with total mastectomy in early breast cancer patients. Ann Oncol 14:1617–1622
Poggi MM, Danforth DN, Sciuto LC et al (2003) Eighteen-year results in the treatment of early breast carcinoma with mastectomy versus breast conservation therapy: the National Cancer Institute Randomized Trial. Cancer 98:697–702
Groot G, Rees H, Pahwa P et al (2011) Predicting local recurrence following breast-conserving therapy for early stage breast cancer: the significance of a narrow (≤2 mm) surgical resection margin. J Surg Oncol 103:212–216
Hewes JC, Imkampe A, Haji A et al (2009) Importance of routine cavity sampling in breast conservation surgery. Br J Surg 96:47–53
Park CC, Mitsumori M, Nixon A et al (2000) Outcome at 8 years after breast-conserving surgery and radiation therapy for invasive breast cancer: influence of margin status and systemic therapy on local recurrence. J Clin Oncol 18:1668–1675
Taghian A, Mohiuddin M, Jagsi R et al (2005) Current perceptions regarding surgical margin status after breast-conserving therapy: results of a survey. Ann Surg 241:629–639
Morrow M, Harris JR, Schnitt SJ (2012) Surgical margins in lumpectomy for breast cancer—bigger are not better. N Engl J Med 367:79–82
Ahmed R, Shaikh H, Hasan SH (1997) Is breast carcinoma a different disease in Pakistani population? J Pak Med Assoc 47:114–116
Revesz E, Khan SA (2011) What are safe margins of resection for invasive and in situ breast cancer? Oncology (Williston Park) 25:890–895
Cefaro GA, Genovesi D, Marchese R et al (2006) Predictors of local recurrence after conservative surgery and whole-breast irradiation. Breast Cancer Res Treat 98:329–335
Houssami N, Macaskill P, Marinovich ML et al (2010) Meta-analysis of the impact of surgical margins on local recurrence in women with early-stage invasive breast cancer treated with breast-conserving therapy. Eur J Cancer 46:3219–3232
King TA, Sakr R, Patil S et al (2011) Clinical management factors contribute to the decision for contralateral prophylactic mastectomy. J Clin Oncol 29:2158–2164
Noh WC, Paik NS, Kim MS et al (2005) Ipsilateral breast tumor recurrence after breast-conserving therapy: a comparison of quadrantectomy versus lumpectomy at a single institution. World J Surg 29:1001–1006. doi:10.1007/s00268-005-7928-4
Miller AR, Brandao G, Prihoda TJ et al (2004) Positive margins following surgical resection of breast carcinoma: analysis of pathologic correlates. J Surg Oncol 86:134–140
Yildirim E (2009) Locoregional recurrence in breast carcinoma patients. Eur J Surg Oncol 35:258–263
Kurniawan ED, Wong MH, Windle I et al (2008) Predictors of surgical margin status in breast-conserving surgery within a breast screening program. Ann Surg Oncol 15:2542–2549
Romond EH, Perez EA, Bryant J et al (2005) Trastuzumab plus adjuvant chemotherapy for operable HER2-positive breast cancer. N Engl J Med 353:1673–1684
Kyndi M, Sørensen FB, Knudsen H et al (2008) Estrogen receptor, progesterone receptor, HER-2, and response to postmastectomy radiotherapy in high-risk breast cancer. J Clin Oncol 26:1419–1426
Millar EKA, Graham PH, O’Toole SA et al (2009) Prediction of local recurrence, distant metastases, and death after breast conserving therapy in early-stage invasive breast cancer using a five-biomarker panel. J Clin Oncol 27:4701–4708
Nguyen PL, Taghian AG, Katz MS et al (2008) Breast cancer subtype approximated by estrogen receptor, progesterone receptor, and HER-2 is associated with local and distant recurrence after breast-conserving therapy. J Clin Oncol 26:2373–2378
Kunos C, Latson L, Overmoyer B et al (2006) Breast conservation surgery achieving > or =2 mm tumor-free margins results in decreased local-regional recurrence rates. Breast J 12:28–36
Lupe K, Truong PT, Alexander C et al (2011) Subsets of women with close or positive margins after breast-conserving surgery with high local recurrence risk despite breast plus boost radiotherapy. Int J Radiat Oncol Biol Phys 81:e561–e568
Akbari ME, Akbari M, Zirakzadeh H et al (2011) Margin status influence on the outcome of patients treated with breast conserving surgery. Iran J Cancer Prev 4:177–182
Pleijhuis RG, Graafland M, de Vries J et al (2009) Obtaining adequate surgical margins in breast-conserving therapy for patients with early-stage breast cancer: current modalities and future directions. Ann Surg Oncol 16:2717–2730
Conflicts of interest
The authors have no conflicts of interest or financial ties to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Bhatti, A.B., Khan, A., Muzaffar, N. et al. Safe Negative Margin Width in Breast Conservative Therapy: Results from a Population with a High Percentage of Negative Prognostic Factors. World J Surg 38, 2863–2870 (2014). https://doi.org/10.1007/s00268-014-2651-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-014-2651-7