
Abstract
Purpose
Blunt bowel and mesenteric injuries (BBMI) are regularly missed by abdominal computed tomography (CT) scans. The aim of this study was to develop a risk assessment tool for BBMI to help clinicians in decision-making for blunt trauma after road traffic crashes (RTCs).
Methods
Single-center retrospective study of trauma patients from January 2010 to April 2015. All patients admitted to our hospital after blunt trauma following RTCs and CT scan at admission were assessed.
Results
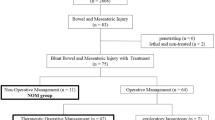
Of the 394 patients included, 78 (19.8%) required surgical exploration and 34 (43.6%) of these had a significant BBMI. A univariate and multivariate analysis were performed comparing patients with BBMI (n = 34) and patients without BBMI (n = 360). A score with a range from 0 to 13 was created. Scores from 8 to 9 were associated with 5–25% BBMI risk. The power of this new score ≥ 8 to predict a surgically significant BBMI had a sensitivity of 96%, specificity of 86.4%, positive predictive value (PPV) of 48% and negative predictive value (NPV) of 99.4%.
Conclusion
This score could be a valuable tool for the management of blunt trauma patients after RTA without a clear indication for laparotomy but at risk for BBMI. The outcome of this study suggests selective diagnostic laparoscopy for a score ≥ 8 in obtunded patients and ≥ 10 in all other. To assess the value and accuracy of this new score, a prospective validation of these retrospective findings is due.



Similar content being viewed by others

References
Fakhry SM, Watts DD, Luchette FA, Group EM-IHVIR. Current diagnostic approaches lack sensitivity in the diagnosis of perforated blunt small bowel injury: analysis from 275,557 trauma admissions from the EAST multi-institutional HVI trial. J Trauma. 2003;54(2):295–306.
Watts DD, Fakhry SM, Group EM-IHVIR. Incidence of hollow viscus injury in blunt trauma: an analysis from 275,557 trauma admissions from the East multi-institutional trial. J Trauma. 2003;54(2):289–94.
Scaglione M, de Lutio di Castelguidone E, Scialpi M, Merola S, Diettrich AI, Lombardo P, Romano L, Grassi R. Blunt trauma to the gastrointestinal tract and mesentery: is there a role for helical CT in the decision-making process? Eur J Radiol. 2004;50(1):67–73.
Jha NK, Yadav SK, Sharma R, Sinha DK, Kumar S, Kerketta MD, Sinha M, Anand A, Gandhi A, Ranjan SK, et al. Characteristics of hollow viscus injury following blunt abdominal trauma; a single centre experience from Eastern India. Bull Emerg Trauma. 2014;2(4):156–60.
Burney RE, Mueller GL, Coon WW, Thomas EJ, Mackenzie JR. Diagnosis of isolated small bowel injury following blunt abdominal trauma. Ann Emerg Med. 1983;12(2):71–4.
Malhotra AK, Fabian TC, Katsis SB, Gavant ML, Croce MA. Blunt bowel and mesenteric injuries: the role of screening computed tomography. J Trauma. 2000;48(6):991–8 (discussion 998–1000).
Demetriades D, Vandenbossche P, Ritz M, Goodmann D, Kowalszik J. Non-therapeutic operations for penetrating trauma: early morbidity and mortality. Br J Surg. 1993;80(7):860–1.
McNutt MK, Chinapuvvula NR, Beckmann NM, Camp EA, Pommerening MJ, Laney RW, West OC, Gill BS, Kozar RA, Cotton BA, et al. Early surgical intervention for blunt bowel injury: the Bowel Injury Prediction Score (BIPS). J Trauma Acute Care Surg. 2015;78(1):105–11.
Zarour A, El-Menyar A, Khattabi M, Tayyem R, Hamed O, Mahmood I, Abdelrahman H, Chiu W, Al-Thani H. A novel practical scoring for early diagnosis of traumatic bowel injury without obvious solid organ injury in hemodynamically stable patients. Int J Surg. 2014;12(4):340–5.
Bossuyt PM, Reitsma JB, Bruns DE, Gatsonis CA, Glasziou PP, Irwig L, LijmerJG Moher D, Rennie D, de Vet HCW, Kressel HY, Rifai N, Golub RM, Altman DG, Hooft L, Korevaar DA, Cohen JF. For the STARD Group. STARD 2015: an updated list of essential items for reporting diagnostic accuracy studies. BMJ. 2015;351:h5527.
Federle MP, Jeffrey RB Jr. Hemoperitoneum studied by computed tomography. Radiology. 1983;148(1):187–92.
R Core Team (2015): R: a language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. https://www.r-project.org/. Accessed 14 Sept 2017.
Joseph DK, Kunac A, Kinler RL, Staff I, Butler KL. Diagnosing blunt hollow viscus injury: is computed tomography the answer? Am J Surg 2013;205(4):414–8.
Porter RS, Zhao N. Patterns of injury in belted and unbelted individuals presenting to a trauma center after motor vehicle crash: seat belt syndrome revisited. Ann Emerg Med 1998;32(4):418–24.
Chidester S, Rana A, Lowell W, Hayes J, Groner J. Is the “seat belt sign” associated with serious abdominal injuries in pediatric trauma? J Trauma. 2009;67(1 Suppl):S34–6.
Fang JF, Chen RJ, Lin BC. Cell count ratio: new criterion of diagnostic peritoneal lavage for detection of hollow organ perforation. J Trauma. 1998;45(3):540–4.
Dolich MO, McKenney MG, Varela JE, Compton RP, McKenney KL, Cohn SM. 2,576 ultrasounds for blunt abdominal trauma. J Trauma. 2001;50(1):108–12.
Mathonnet M, Peyrou P, Gainant A, Bouvier S, Cubertafond P. Role of laparoscopy in blunt perforations of the small bowel. Surg Endosc. 2003;17(4):641–5.
Mitsuhide K, Junichi S, Atsushi N, Masakazu D, Shinobu H, Tomohisa E, Hiroshi Y. Computed tomographic scanning and selective laparoscopy in the diagnosis of blunt bowel injury: a prospective study. J Trauma. 2005;58(4):696–701 (discussion 701–693).
Rossi P, Mullins D, Thal E. Role of laparoscopy in the evaluation of abdominal trauma. Am J Surg. 1993;166(6):707–10 (discussion 710–701).
Villavicencio RT, Aucar JA. Analysis of laparoscopy in trauma. J Am Coll Surg. 1999;189(1):11–20.
Faget C, Taourel P, Charbit J, Ruyer A, Alili C, Molinari N, Millet I. Value of CT to predict surgically important bowel and/or mesenteric injury in blunt trauma: performance of a preliminary scoring system. Eur Radiol. 2015;25(12):3620–8.
Brofman N, Atri M, Hanson JM, Grinblat L, Chughtai T, Brenneman F. Evaluation of bowel and mesenteric blunt trauma with multidetector CT. Radiographics. 2006;26(4):1119–31.
Rodriguez C, Barone JE, Wilbanks TO, Rha CK, Miller K. Isolated free fluid on computed tomographic scan in blunt abdominal trauma: a systematic review of incidence and management. J Trauma. 2002;53(1):79–85.
Jansen TC, van Bommel J, Mulder PG, Rommes JH, Schieveld SJ, Bakker J. The prognostic value of blood lactate levels relative to that of vital signs in the pre-hospital setting: a pilot study. Crit care. 2008;12(6):R160.
Shin JS, Shin JH, Ko HK, Kim JW, Yoon HK. Transcatheter arterial embolization for traumatic mesenteric bleeding: a 15-year, single-center experience. Diagn Interv Radiol. 2016;22(4):385–9.
Jones EL, Stovall RT, Jones TS, Bensard DD, Burlew CC, Johnson JL, Jurkovich GJ, Barnett CC, Pieracci FM, Biffl WL, et al. Intra-abdominal injury following blunt trauma becomes clinically apparent within 9 h. J Trauma Acute Care Surg. 2014;76(4):1020–3. https://doi.org/10.1097/TA.0000000000000131.
Fakhry SM, Brownstein M, Watts DD, Baker CC, Oller D. Relatively short diagnostic delays (< 8 h) produce morbidity and mortality in blunt small bowel injury: an analysis of time to operative intervention in 198 patients from a multicenter experience. J Trauma. 2000;48(3):408–14 (discussion 414–405).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflict of interest.
Funding
None.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Raharimanantsoa, M., Zingg, T., Thiery, A. et al. Proposal of a new preliminary scoring tool for early identification of significant blunt bowel and mesenteric injuries in patients at risk after road traffic crashes. Eur J Trauma Emerg Surg 44, 779–785 (2018). https://doi.org/10.1007/s00068-017-0893-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00068-017-0893-4