
Abstract
Background
Bowel and/or mesentery injuries represent the third most common injury among patients with blunt abdominal trauma. Delayed diagnosis increases morbidity and mortality. The aim of our study was to evaluate the role of clinical signs along with CT findings as predictors of early surgical repair.
Material and methods
Between March 2014 and February 2017, charts and CT scans of consecutive patients treated for blunt abdominal trauma in two different trauma centers were reread by two experienced radiologists. We included all adult patients who underwent contrast-enhanced CT of the abdomen and pelvis with CT findings of blunt bowel and/or mesenteric injury (BBMI). We divided CT findings into two groups: the first included three highly specific CT signs and the second included six less specific CT signs indicated as “minor CT findings.” The presence of abdominal guarding and/or abdominal pain was considered as “clinical signs.” Reference standards included surgically proven BBMI and clinical follow-up. Association was evaluated by the chi-square test. A logistic regression model was used to estimate odds ratio (OR) and confidence intervals (CI).
Results
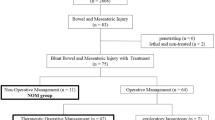
Thirty-four (4.1%) out of 831 patients who sustained blunt abdominal trauma had BBMI at CT. Twenty-one out of thirty-four patients (61.8%) underwent surgical repair; the remaining 13 were treated conservatively. Free fluid had a significant statistical association with surgery (p = 0.0044). The presence of three or more minor CT findings was statistically associated with surgery (OR = 8.1; 95% CI, 1.2–53.7). Abdominal guarding along with bowel wall discontinuity and extraluminal air had the highest positive predictive value (100 and 83.3%, respectively).
Conclusion
In patients without solid organ injury (SOI), the presence of free fluid along with abdominal guarding and three or more “minor CT findings” is a significant predictor of early surgical repair. The association of bowel wall discontinuity with extraluminal air warrants exploratory laparotomy.



Similar content being viewed by others


References
Scaglione M, De Lutio di Castelguidone E, Scialpi M et al (2004) Blunt trauma to the gastrointestinal tract and mesentery: is there a role for helical CT in the decision-making process? Eur J Radiol 50:67–73
Cinquantini F, Tugnoli G, Piccinini A, Coniglio C, Mannone S, Biscardi A, Gordini G, di Saverio S (2017) Educational review of predictive value and findings of computed tomography scan in diagnosing bowel and mesenteric injuries after blunt trauma: correlation with trauma surgery findings in 163 patients. Can Assoc Radiol J 68:276–285
Brody JM, Leighton DB, Murphy BL, Abbott GF, Vaccaro JP, Jagminas L, Cioffi WG (2000) CT of blunt trauma bowel and mesenteric injury: typical findings and pitfalls in diagnosis. Radiographics 20:1525–1527
McNutt MK, Chinapuvvula NR, Beckmann NM et al (2015) Early surgical intervention for blunt bowel injury: the Bowel Injury Prediction Score (BIPS). J Trauma Acute Care Surg 78:105–111
Bates DDB, Wasserman M, Malek A, Gorantla V, Anderson SW, Soto JA, LeBedis CA (2017) Multidetector CT of surgically proven blunt bowel and mesenteric injury. Radiographics 37:613–625
Abdi H (2007) The Bonferonni and Šidák corrections for multiple comparisons. In: Encyclopedia of measurement and statistics. SAGE, Thousand Oaks
Youden W (1950) Index for rating diagnostic tests. Cancer 3:32–35
Joseph DK, Kunac A, Kinler RL et al (2013) Diagnosing blunt hollow viscus injury: is computed tomography the answer? Am J Surg 205:414–418
Yu J, Fulcher AS, Turner MA, Cockrell C, Halvorsen RA (2011) Blunt bowel and mesenteric injury: MDCT diagnosis. Abdom Imaging 36:50–61
Malinoski DJ, Patel MS, Yakar DO, Green D, Qureshi F, Inaba K, Brown CVR, Salim A (2010) A diagnostic delay of 5 hours increases the risk of death after blunt hollow viscus injury. J Trauma 69:84–87
Fakhry SM, Brownstein M, Watts DD et al (2000) Relatively short diagnostic delays (< 8 hours) produce morbidity and mortality in blunt small bowel injury: an analysis of time to operative intervention in 198 patients from a multicenter experience. J Trauma 48:408–14–5
Livingston DH, Lavery RF, Passannante MR et al (1998) Admission or observation is not necessary after a negative abdominal computed tomographic scan in patients with suspected blunt abdominal trauma: results of a prospective, multi-institutional trial. J Trauma 44:273–80–2
Dowe MF, Shanmuganathan K, Mirvis SE, Steiner RC, Cooper C (1997) CT findings of mesenteric injury after blunt trauma: implications for surgical intervention. AJR Am J Roentgenol 168:425–428
Brofman N, Atri M, Hanson JM, Grinblat L, Chughtai T, Brenneman F (2006) Evaluation of bowel and mesenteric blunt trauma with multidetector CT. Radiographics 26:1119–1131
Ekeh AP, Saxe J, Walusimbi M, Tchorz KM, Woods RJ, Anderson HL III, McCarthy MC (2008) Diagnosis of blunt intestinal and mesenteric injury in the era of multidetector CT technology—are results better? J Trauma 65:354–359
Soto JA, Anderson SW (2012) Multidetector CT of blunt abdominal trauma. Radiology 265:678–693
Drasin TE, Anderson SW, Asandra A, Rhea JT, Soto JA (2008) MDCT evaluation of blunt abdominal trauma: clinical significance of free intraperitoneal fluid in males with absence of identifiable injury. AJR Am J Roentgenol 191:1821–1826
Mirvis SE, Shanmuganathan K, Erb R (1994) Diffuse small-bowel ischemia in hypotensive adults after blunt trauma (shock bowel): CT findings and clinical significance. AJR Am J Roentgenol 163:1375–1379
Prasad KR, Kumar A, Gamanagatti S, Chandrashekhara SH (2011) CT in post-traumatic hypoperfusion complex—a pictorial review. Emerg Radiol 18:139–143
Virmani V, George U, MacDonald B, Sheikh A (2013) Small-bowel and mesenteric injuries in blunt trauma of the abdomen. Can Assoc Radiol J 64:140–147
Malhotra AK, Fabian TC, Katsis SB, Gavant ML, Croce MA (2000) Blunt bowel and mesenteric injuries: the role of screening computed tomography. J Trauma 48:991–1000
Dhatt HS, Behr SC, Miracle A, Wang ZJ, Yeh BM (2015) Radiological evaluation of bowel ischemia. Radiol Clin N Am 53:1241–1254
Ames JT, Federle MP (2009) CT hypotension complex (shock bowel) is not always due to traumatic hypovolemic shock. AJR Am J Roentgenol 192:W230–W235
Alarhayem AQ, Myers JG, Dent D et al (2015) Blush at first sight significance of computed tomographic and angiographic discrepancy in patients with blunt abdominal trauma. Am J Surg 210:1104–10–1
Ingram M-CE, Siddharthan RV, Morris AD, Hill SJ, Travers CD, McKracken CE, Heiss KF, Raval MV, Santore MT (2016) Hepatic and splenic blush on computed tomography in children following blunt abdominal trauma: is intervention necessary? J Trauma Acute Care Surg 81:266–270
Marek AP, Deisler RF, Sutherland JB, Punjabi G, Portillo A, Krook J, Richardson CJ, Nygaard RM, Ney AL (2014) CT scan-detected pneumoperitoneum: an unreliable predictor of intra-abdominal injury in blunt trauma. Injury 45:116–121
Hamilton P, Rizoli S, McLellan B, Murphy J (1995) Significance of intra-abdominal extraluminal air detected by CT scan in blunt abdominal trauma. J Trauma 39:331–333
Izumi J, Hirano H, Kato T, Ito T, Kinoshita K, Wakabayashi T (2012) CT findings of spontaneous intraperitoneal rupture of the urinary bladder: two case reports. Jpn J Radiol 30:284–287
Hanks PW, Brody JM (2003) Blunt injury to mesentery and small bowel: CT evaluation. Radiol Clin North Am 41:1171–1182
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Firetto, M.C., Sala, F., Petrini, M. et al. Blunt bowel and mesenteric trauma: role of clinical signs along with CT findings in patients’ management. Emerg Radiol 25, 461–467 (2018). https://doi.org/10.1007/s10140-018-1608-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10140-018-1608-9