
Abstract
Background
We compared direct stenting (DS) with conventional stenting (CS) – i.e., stenting after predilation – during primary percutaneous coronary intervention (P-PCI) in terms of procedural results and long-term mortality in patients with ST-elevated myocardial infarction (STEMI).
Methods
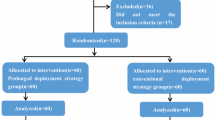
We retrospectively analyzed 2306 patients (mean age 59 years, 22% female) who underwent P‑PCI within 12 h of symptom onset. Patients were then followed up prospectively for clinical events. Patients were divided into a DS group (n = 597) and a CS group (n = 1709). The CS group was further divided into a CS-1 group (baseline thrombolysis in myocardial infarction [TIMI] flow grade ≥ 1) and a CS-2 group (baseline TIMI flow grade 0). Main outcome measures were postprocedural myocardial reperfusion and all-cause mortality in long-term follow-up.
Results
Patients in the DS group had a higher percentage of final TIMI-3 flow, myocardial blush grade 3 and complete ST-segment resolution, better left ventricular ejection fraction, and a lower incidence of distal embolization compared with CS patients. In-hospital (1.5 vs. 4.6%, respectively, p = 0.001) and long-term all-cause mortality (8.8 vs. 17.0%, respectively, p < 0.001) were significantly lower in the DS group than in the CS group. Kaplan–Meier survival analysis showed similar survival rates in the DS and CS-1 groups (log-rank p = 0.40), but significantly worse survival in the CS-2 group than in the other groups (log-rank p < 0.001). After adjusting for risk factors, DS was not found to be a predictor of long-term mortality.
Conclusion
DS in P‑PCI was associated with better postprocedural angiographic results and long-term survival. However, the DS group had similar in-hospital and long-term mortality to matched patients in the CS group.
Zusammenfassung
Hintergrund
Ziel war es, die direkte Stentimplantation („direct stenting“, DS) mit der konventionellen Stenteinlage („conventional stenting“, CS), d. h. Stenteinlage nach Vordehnung, während primärer perkutaner Koronarintervention (P-PCI) in Bezug auf Verfahrensergebnisse und Langzeitmortalität bei Patienten mit ST-Hebungs-Infarkt (STEMI) zu vergleichen.
Methoden
Retrospektiv wurden die Daten von 2306 Patienten (Durchschnittsalter: 59 Jahre, 22 % w.) ausgewertet, bei denen innerhalb von 12 h nach Symptombeginn eine P‑PCI erfolgte. Danach wurden die Patienten prospektiv in Hinsicht auf klinische Ereignisse nachbeobachtet. Die Patienten wurden aufgeteilt auf eine DS-Gruppe (n = 597) und eine CS-Gruppe (n = 1709). Die CS-Gruppe war weiter unterteilt in eine CS-1-Gruppe (Ausgangswert für den Durchflussgrad nach TIMI-Klassifikation, „thrombolysis in myocardial infarction“ ≥1 und eine CS-2-Gruppe (Ausgangswert für den TIMI-Fluss: 0). Hauptendpunktparameter waren die postprozedurale Myokardreperfusion und die Gesamtmortalität im Langzeit-Follow-up.
Ergebnisse
Bei den Patienten in der DS-Gruppe bestanden für einen größeren Anteil ein abschließender TIMI-Fluss von 3, „myocardial blush grade“ von 3 und vollständige ST-Strecken-Erholung, bessere linksventrikuläre Ejektionsfraktion und niedrigere Inzidenz der distalen Embolisierung im Vergleich zu CS-Patienten. Die stationäre (1,5 % vs. 4,6 %, p = 0,001) und die Langzeitgesamtmortalität (8,8 % vs. 17,0 %, p < 0,001) waren in der DS-Gruppe signifikant niedriger als in der CS-Gruppe. Die Überlebensanalyse nach Kaplan-Meier zeigte in der DS- und CS-1-Gruppe (log-rank: p = 0,40) ähnliche Überlebensraten, aber ein signifikant schlechteres Überleben in der CS-2-Gruppe im Vergleich zu den anderen Gruppen (log-rank: p < 0,001). Wurden die Risikofaktoren berücksichtigt, stellte sich DS nicht als Prädiktor der Langzeitmortalität heraus.
Schlussfolgerung
Die DS-Methode bei P‑PCI ging mit besseren postprozeduralen Angiographieergebnissen und Langzeitüberleben einher. Jedoch waren für die DS-Gruppe die stationäre und die Langzeitmortalität ähnlich wie für entsprechend ausgewählte Patienten in der CS-Gruppe.


Similar content being viewed by others

References
Antoniucci D, Valenti R, Migliorini A et al (2001) Direct infarct artery stenting without predilation and no-reflow in patients with acute myocardial infarction. Am Heart J 142:684–690
Loubeyre C, Morice MC, Lefèvre T et al (2002) A randomized comparison of direct stenting with conventional stent implantation in selected patients with acute myocardial infarction. J Am Coll Cardiol 39:15–21
Möckel M, Vollert J, Lansky AJ et al (2011) Horizons-AMI Trial Investigators. Comparison of direct stenting with conventional stent implantation in acute myocardial infarction. Am J Cardiol 108:1697–1703
Lang RM, Bierig M, Devereux RB et al (2006) Recommendations for chamber quantification. Eur J Echocardiogr 7:79–108
Van de Werf F, Bax J, Betriu A et al (2008) Management of acute myocardial infarction in patients presenting with persistent ST-segment elevation: the Task Force on the Management of ST-Segment Elevation Acute Myocardial Infarction of the European Society of Cardiology. Eur Heart J 29:2909–2945
World Health Organization (1968) Nutritional anemias: report of a WHO Scientific Group. World Health Organization, Geneva
Levey AS, Bosch JP, Lewis JB et al (1999) A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Modification of Diet in Renal Disease Study Group. Ann Intern Med 130:461–470
Morrow DA, Antman EM, Charlesworth A et al (2000) TIMI risk score for STelevation myocardial infarction: a convenient, bedside, clinical score for risk assessment at presentation. Circulation 102:2031–2037
Sianos G, Morel MA, Kappetein AP et al (2005) The SYNTAX score: an angiographic tool grading the complexity of coronary artery disease. EuroIntervention 1:219–227
Gibson CM, de Lemos JA, Murphy SA et al (2001) Combination therapy with Abciximab reduces angiographically evident thrombus in acute myocardial infarction: a TIMI 14 Substudy. Circulation 103:2550–2554
van’t Hof AW, Liem A, Suryapranata H et al (1998) Angiographic assessment of myocardial reperfusion in patients treated with primary angioplasty for acute myocardial infarction: myocardial blush grade. Zwolle Myocardial Infarction Study Group. Circulation 97:2302–2306
de Lemos JA, Braunwald E (2001) ST segment resolution as a tool for assessing the efficacy of reperfusion therapy. J Am Coll Cardiol 38:1283–1294
Thygesen K, Alpert JS, White HD, Joint ESC/ACCF/AHA/WHF Task Force for the Redefinition of Myocardial Infarction (2007) Universal definition of myocardial infarction. Eur Heart J 28:2525–2538
Cutlip DE, Windecker S, Mehran R et al (2007) Clinical end points in coronary stent trials: a case for standardized definitions. Circulation 115:2344–2351
Reffelmann T, Kloner RA (2002) The no-reflow phenomenon: basic science and clinical correlates. Heart 87:162–168
Henriques JP, Zijlstra F, Ottervanger JP et al (2002) Incidence and clinical significance of distal embolization during primary angioplasty for acute myocardial infarction. Eur Heart J 23:1112–1117
Heusch G, Schulz R, Baumgart D et al (2001) Coronary microembolization [review]. Prog Cardiovasc Dis 44:217–230
Rogers C, Parikh S, Seifert P et al (1996) Endogenous cell seeding: remnant endothelium after stenting enhances vascular repair. Circulation 94:2909–2914
Cuisset T, Hamilos M, Melikian N et al (2008) Direct stenting for stable angina pectoris is associated with reduced periprocedural microcirculatory injury compared with stenting after pre-dilation. J Am Coll Cardiol 51:1060–1065
Hoffmann R, Takimoglu-Boerekci M, Langenberg R et al (2004) Randomized comparison of direct stenting with predilatation followed by stenting on vessel trauma and restenosis. Am Heart J 147:E13
Brodie BR, Stuckey TD, Hansen C et al (2000) Benefit of coronary reperfusion before intervention on outcomes after primary angioplasty for acute myocardial infarction. Am J Cardiol 85:13–18
Ishihara M, Inoue I, Kawagoe T et al (2002) Impact of spontaneous anterograde flow of the infarct artery on left ventricular function in patients with a first anterior wall acute myocardial infarction. Am J Cardiol 90:5–9
Magro M, Nauta ST, Simsek C et al (2012) Usefulness of the SYNTAX score to predict “no reflow” in patients treated with primary percutaneous coronary intervention for ST-segment elevation myocardial infarction. Am J Cardiol 109:601–606
Magro M, Nauta S, Simsek C et al (2011) Value of the SYNTAX score in patients treated by primary percutaneous coronary intervention for acute ST-elevation myocardial infarction: the MI SYNTAXscore study. Am Heart J 161:771–781
Gasior M, Gierlotka M, Lekston A et al (2007) Comparison of outcomes of direct stenting versus stenting after balloon predilation in patients with acute myocardial infarction (DIRAMI). Am J Cardiol 100:798–805
Antoniucci D, Valenti R, Migliorini A et al (2004) Comparison of rheolytic thrombectomy before direct infarct artery stenting versus direct stenting alone in patients undergoing percutaneous coronary intervention for acute myocardial infarction. Am J Cardiol 93:1033–1035
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
A. Kalayci, V. Oduncu, C. Karabay, A. Erkol, A.C. Tanalp, I.H. Tanboga, O. Candan, C. Gecmen, I.A. Izgi, and C. Kirma declare that they have no competing interests.
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Kalayci, A., Oduncu, V., Karabay, C.Y. et al. Outcomes of direct stenting in patients with ST-elevated myocardial infarction. Herz 43, 447–454 (2018). https://doi.org/10.1007/s00059-017-4581-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00059-017-4581-2