
Abstract
Background
Diffuse parenchymal lung diseases (DPLDs) constitute a heterogeneous group of lung diseases characterized by variable degrees of inflammation and fibrosis. In some DPLD, significant morbidity and unfavorable prognosis, comparable to those of neoplastic diseases, are seen. Efficient and safe methods for the diagnosis of DPLD are needed.
Aim
of the work To assess the characteristic features of DPLD in Fayoum Governorate based on clinical, radiological, and functional assessment.
Patients and methods
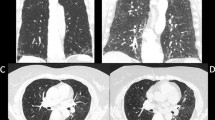
This study included 100 patients with undiagnosed DPLD who were selected from the Chest Department, Fayoum University Hospital, during the period from June 2015 to June 2016. All patients were subjected to written informed consent, full medical history, echocardiography, collagen profile, arterial blood gas analysis, spirometry, 6 min walk test, high-resolution computed tomography (HRCT) of the chest and lung biopsy when indicated.
Results
Out of the 100 patients included in the study, 72 (72%) were women, 28 (28%) were men, 15 (15%) were smokers, and 73 (73%) had a history of raising birds. The mean age was 45.4 years(range, 8–85 years). HRCT showed different patterns of parenchymal affection. Idiopathic interstitial pneumonia was the predominant diagnosis (51%), followed by DPLD of known cause (33%), then granulomatous DPLD (12%), and lastly other rare forms of DPLD (4%).
Conclusion
The historical ‘gold standard’ of histological DPLD diagnosis is replaced by a ‘dynamic integrated approach’ using multidisciplinary discussion. The optimal HRCT technique for the evaluation of DPLD is crucial. HRCT of the chest was the diagnostic tool in 75% of the study patients without the need for biopsy.
Article PDF
Similar content being viewed by others


References
Belloli EA, Beckford R, Hadley R, Flaherty KR. Idiopathic non-specific interstitial pneumonia. Respirology 2016; 21: 259–268.
Talmadge KE Jr. Approach to the adult with interstitial lung disease: clinical evaluation. UpToDat 2014; 214.
Raghu G, Chen SY, Yeh WS, Maroni B, Li Q, Lee YC, Collard HR. Idiopathic pulmonary fibrosis in US Medicare beneficiaries aged 65 years and older: incidence, prevalence, and survival, 2001–11. Lancet Respir Med 2014; 2: 566–572.
Desai SR, Wells AU. Imaging. In: Costabel U, Du Bois RM, Egan JJ, (eds). Diffuse parenchymal lung disease. Basel: Karger 2007. 36: 29–43.
Travis WD, Costabel U, Hansell DM, King TE Jr, David A. An official AmericanThoracic Society/European Respiratory Society Statement: update of the international multidisciplinary classification of the idiopathic interstitial pneumonias. Am J Respir Crit Care 2013; 188: 733–748.
Perez LL. Office spirometry. Osteopathic Fam Physician 2013; 5: 65–69.
Webb WR, Muller NL, Naidich DP. High-resolution CT of the lung (5th ed.). In: Lawrence R. Goodman (ed). LWW 2014. 752.
Bossone E, D’Andrea A, D’Alto M, Citro R, Argiento P, Ferrara F, et al. Echocardiography in pulmonary arterial hypertension from diagnosis to prognosis. J Am Soc Echocardiogr 2013; 26: 1–14.
Sehgal IS, Bal A, Dhooria S, Agrawal P, Gupta N, Ram B, et al. A prospective randomized controlled trial comparing the efficacy and safety of cup vs alligator forceps for performing transbronchial lung biopsy in patients with sarcoidosis. Chest 2016; 149: 1584–1586.
Clement A, Nathan N, Epaud R, Fauroux B, Corvol H. Interstitial lung diseases in children. Orphanet J Rare Dis 2010; 5: 22.
Ahmed S, El Hindawi A, Mashhour S. Spectrum of diffuse parenchymal lung diseases using medical thoracoscopic lung biopsy: an experience with 55 patients during 2013–2015. Egypt J Chest Dis Tuberc 2016; 65: 717–722.
Abdel Salam E. Medical thoracoscopy for diagnosis of DPLD other than UIP [MD thesis]. Cairo: Faculty of Medicine, Cairo University. 2015.
López-Campos J, Rodríguez-Becerra E; Neumosur Task Group; Registry of Interstitial Lung Diseases. Incidence of interstitial lung diseases in the south of Spain 1998–2000: the RENIA study. Eur J Epidemiol 2004; 19: 155–161.
Lederer DJ, Enright PL, Kawut SM, Hoffman EA, Hunninghake G, van Beek EJR, et al. Cigarette smoking is associated with subclinical parenchymal lung disease the multi-ethnic study of atherosclerosis (MESA)-lung study. Am J Respir Crit Care Med 2009; 180: 407–414.
McSharry C, Dye GM, Ismail T, Anderson K, Spiers EM, Boyd G. Quantifying serum antibody inbird fanciers’ hypersensitivity pneumonitis. BMC Pulm Med 2006; 6: 16.
Appel JZ, Lee SM, Hartwig MG, Li B, Hsieh CC, Cantu E IIIrd, et al. Characterization of the innate immune response to chronic aspiration in a novel rodent model. Respir Res 2007; 8: 87.
Raghu G, Freudenberger TD, Yang S, Curtis JR, Spada C, Hayes J, et al. High prevalence of abnormal acid gastro-oesophageal reflux in idiopathic pulmonary fibrosis. Eur Respir J 2006; 27: 136–142.
Manganelli P, Salaffi F, Pesci A. Hepatitis C virus and pulmonary fibrosis. Recenti Prog Med 2002; 93: 322–326.
Lettieri CJ, Nathan SD, Barnett SD, Ahmad S, Shorr AF. Prevalence and outcomes of pulmonary arterial hypertension in advanced idiopathic pulmonary fibrosis. Chest 2006; 129: 746–752.
Hamada K, Nagai S, Tanaka S, Handa T, Shigematsu M, Nagao T, et al. Significance of pulmonary arterial pressure and diffusion capacity of the lung as prognosticator in patients with idiopathic pulmonary fibrosis. Chest 2007; 131: 650–656.
Martinez FJ, Flaherty K. Pulmonary function testing in idiopathic interstitial pneumonias. Proc Am Thorac Soc 2006; 3: 315–321.
Ishie RT, Cardoso J, Silveira RJ, Stocco L. Video-assisted thoracoscopy for the diagnosis of diffuse parenchymal lung disease. J Bras Pneumol 2009; 35: 234–241.
Wuyts W. Surgical lung biopsy is not the golden standard in diagnosis of diffuse parenchymal lung diseases. Eur J Cardiothorac Surg 2008; 34: 1271–1272.
Chang AC, Yee J, Orringer MB, Iannettoni MD. Diagnostic thoracoscopic lung biopsy: an outpatient experience. Ann Thorac Surg 2002; 74: 1942–1947.
Faraga TS, Adawya ZR, Sakrb LK, Abdellateefa HS. Transthoracic ultrasonographic features of diffuse parenchymal lung diseases. Egypt J Bronchol 2017; 11: 179–187.
Author information
Authors and Affiliations
Corresponding author
Additional information
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
Rights and permissions
This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
AbouYoussef, H.A., Sabri, Y.Y.Y., El Essawy, A.F. et al. Clinico-radiography and pulmonary functional assessment of patients with diffuse parenchymal lung diseases in al-fayoum governorate. Egypt J Bronchol 13, 125–131 (2019). https://doi.org/10.4103/ejb.ejb_40_18
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.4103/ejb.ejb_40_18