
Abstract
Objectives
The purposeof this study was to evaluate the diagnostic accuracy of transthoracic ultrasound in patients with bronchiectasis and compare it with high-resolution computed tomography (HRCT) chest.
Patients and methods
Sixty-one patients with bronchiectasis underwent transthoracic ultrasound. Radiological severity of bronchiectasis was assessed using a modified Reiff score (number of lobes involved in six lobes multiplied by the degree of bronchial dilatation) (tubular=1, varicose=2, cystic=3). Transthoracic findings were compared with that of the HRCT and pulmonary function tests.
Results
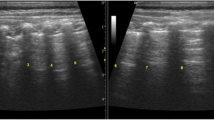
Two patterns of sonographic abnormalities were detected: B-line pattern and c-profile (consolidation) pattern. The first was detected in 42 (68.8%) patients and the later was detected in seven (11.1%) patients. Twelve (19.7%) patients had normal sonographic examination. There was significant positive correlation between severity of bronchiectasis by the modified Reiff score pattern. The highest score correlated with the c-profile pattern and the lower score correlated with the B-line pattern (P≤0.001), while patients with very low score (≤20) had normal examination. There was a negative correlation between HRCT score, ultrasound pattern, and Partial pressure of oxygen tension (PO2) (P≤0.001).
Conclusion
Bronchiectasis can be assessed by chest ultrasound; pattern of sonography is correlated to the radiological severity and functional impairment of the disease.
Article PDF
Similar content being viewed by others

References
Volpicelli G. Lung sonography. J Ultrasound Med 2013; 32:165–171.
Bove T, Oppizzi M, Marino G, Zangrillo A, Margonato Aand Picano E. Ultrasound comet-tail images:a marker of pulmonary edema:a comparative study with wedge pressure and extravascular lung water. Chest J 2005; 127:1690–1695.
Pasteur MC, Helliwell SM, Houghton SJ, Webb SC, Foweraker JE, Coulden RA, et al. An investigation into causative factors in patients with bronchiectasis. Am J Respir Crit Care Med 2000; 162:1277–1284.
Chalmers JD, Mchugh BJ, Doherty C, Smith MP, Govan JR, Kilpatrick DC, et al. Mannose-binding lectin deficiency and disease severity in non-cystic fibrosis bronchiectasis:a prospective study. Lancet Respir Med 2013; 1:224–232.
Reiff DB, Wells AU, Carr DH, Cole Pand Hansell D. CT findings in bronchiectasis:limited value in distinguishing between idiopathic and specific types. Am J Roentgenol 1995; 165:261–267.
Volpicelli G, Elbarbary M, Blaivas M, Lichtenstein DA, Mathis G, Kirkpatrick AW, et al. International evidence-based recommendations for point-of-care lung ultrasound. Intensive Care Med 2012; 38:577–591.
Piette E, Daoust R, Denault A. Basic concepts in the use of thoracic and lung ultrasound. Curr Opin Anesthesiol 2013; 26:20–30.
Sayed S, Agmy G, Said A, Kasem A. Assessment of transthoracic sonography in patients with interstitial lung diseases. Egypt J Bronchol 2016; 10:105–112.
Hasan A, Makhlouf H. B-lines:transthoracic chest ultrasound signs useful in assessment of interstitial lung diseases. Ann Thorac Med 2014; 9:99–103.
Lichtenstein D, MÉziÈre G, Biderman P, Gepner A, BarrÉ O. The comet-tail artifact. Am J Respir Crit Care Med 1997; 156:1640–1646.
Gehmacher O, Mathis G, Kopf A, Scheier M. Ultrasound imaging of pneumonia. Ultrasound Med Biol 1995; 21:1119–1122.
Lichtenstein DA, Lascols N, Mezière G, Gepner A. Ultrasound diagnosis of alveolar consolidation in the critically ill. Intensive Care Med 2004; 30:276–281.
Mathis G, Blank W, Reißig A, Lechleitner P, Reuß J, Schuler A, et al. Thoracic ultrasound for diagnosing pulmonary embolism:a prospective multicenter study of 352 patients. Chest J 2005; 128:1531–1538.
Parlamento S, Copetti R, Di Bartolomeo S. Evaluation of lung ultrasound for the diagnosis of pneumonia in the ED. Am J Emerg Med 2009; 27:379–384.
Reissig A, Kroegel C. Sonographic diagnosis and follow-up of pneumonia:a prospective study. Respiration 2007; 74:537–547.
Ooi GC, Khong PL, Chan-Yeung M, Ho JC, Chan PK, Lee JC, et al. High-resolution CT quantification of bronchiectasis:clinical and functional correlation. Radiology 2002; 225:663–672.
Landau L, Phelan P, Williams H. Ventilatory mechanics in patients with bronchiectasis starting in childhood. Thorax 1974; 29:304–312.
Kang EY, Miller R, Müller NL. Bronchiectasis:comparison of preoperative thin-section CT and pathologic findings in resected specimens. Radiology 1995; 195:649–654.
Author information
Authors and Affiliations
Corresponding author
Additional information
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
Rights and permissions
This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ghany, M.F.A. Transthoracic ultrasound in the diagnosis of bronchiectasis: is it valuable?. Egypt J Bronchol 13, 303–308 (2019). https://doi.org/10.4103/ejb.ejb_2_19
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.4103/ejb.ejb_2_19