
Abstract
Background
The characteristics of patients with dermatitis herpetiformis (DH) in France is poorly documented. Furthermore, the risk of fractures and bone mineral density (BMD) in DH remain under-described, and recommendations for systematic screening for osteoporosis in DH are lacking.
Objectives
To describe the characteristics of DH in a large French cohort and evaluate the association between BMD and features of osteoporosis.
Materials and methods
Patients were recruited from the French Association of Gluten Intolerants (AFDIAG) and a single university dermatology department. A telephone questionnaire was used to record features of DH, history of fractures, calcium intake, treatment, and the gluten-free diet (GFD). Serum calcium and 25(OH) vitamin D3+D2 levels, as well as BMD, were measured.
Results
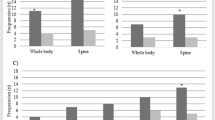
We included 53 patients (27 men) with a median age of 49 years (range: 23-86). Median disease duration before inclusion was 14 years (range: 2-55); 51 patients (96%) were adherent to a GFD and had no digestive symptoms. Overall, 18 (34%) had a history of fractures; 16 high-velocity (traumatic) and two low-velocity (nontraumatic). Mean BMD, measured in 48 patients, was normal (femoral neck: 0.956 ± 0.210 g/cm2; lumbar spine: 1.091 ± 1.199 g/cm2). In all, 18 patients (38%) had osteopenia and one (2%) osteoporosis. T-score for bone density did not differ with and without fractures. Calcium intake and serum calcium level were normal in all patients.
Conclusion
Screening for osteoporosis does not appear to be mandatory for DH patients with good adherence to a GFD and without digestive symptoms or additional risk factors of osteoporosis.
Similar content being viewed by others


References
Salmi TT, Hervonen K, Kautiainen H, Collin P, Reunala T. Prevalence and incidence of dermatitis herpetiformis: a 40-year prospective study from Finland. Br J Dermatol 2011; 165: 354–9.
Reunala TL. Dermatitis herpetiformis. Clin Dermatol 2001; 19: 728–36.
Ingen-Housz-Oro S. Dermatitis herpetiformis: a review. Ann Dermatol Venereol 2011; 138: 221–7.
Bolotin D, Petronic-Rosic V. Dermatitis herpetiformis. Part I. Epidemiology, pathogenesis, and clinical presentation. J Am Acad Dermatol 2011; 64: 1017–26.
Reunala T, Collin P. Diseases associated with dermatitis herpetiformis. Br J Dermatol 1997; 136: 315–8.
Alonso-Llamazares J, Gibson LE, Rogers RS. Clinical, pathologic, and immunopathologic features of dermatitis herpetiformis: review of the Mayo Clinic experience. Int J Dermatol 2007; 46: 910–9.
Hjelle AM, Apalset E, Mielnik P, Bollerslev J, Lundin KEA, Tell GS. Celiac disease and risk of fracture in adults-a review. Osteoporos Int 2014; 25: 1667–76.
Lucendo AJ, García-Manzanares A. Bone mineral density in adult coeliac disease: an updated review. Rev Esp Enferm Dig 2013; 105: 154–62.
Di Stefano M, Jorizzo RA, Veneto G, Cecchetti L, Gasbarrini G, Corazza GR. Bone mass and metabolism in dermatitis herpetiformis. Dig Dis Sci 1999; 44: 2139–43.
Abuzakouk M, Barnes L, O’Gorman N, et al. Dermatitis herpetiformis: no evidence of bone disease despite evidence of enteropathy. Dig Dis Sci 2007; 52: 659–64.
Lewis NR, Logan RFA, Hubbard RB, West J. No increase in risk of fracture, malignancy or mortality in dermatitis herpetiformis: a cohort study. Aliment Pharmacol Ther 2008; 27: 1140–7.
Lorinczy K, Juhász M, Csontos Á, et al. Does dermatitis herpetiformis result in bone loss as coeliac disease does? A cross sectional study. Rev Esp Enferm Dig 2013; 105: 187–93.
Kanis JA. Assessment of fracture risk and its application to screening for postmenopausal osteoporosis: synopsis of a WHO report. WHO Study Group. Osteoporos Int 1994; 4: 368–81.
Gaspari AA, Huang CM, Davey RJ, Bondy C, Lawley TJ, Katz SI. Prevalence of thyroid abnormalities in patients with dermatitis herpetiformis and in control subjects with HLA-B8/-DR3. Am J Med 1990; 88: 145–50.
Cunningham MJ, Zone JJ. Thyroid abnormalities in dermatitis herpetiformis. Prevalence of clinical thyroid disease and thyroid autoantibodies. Ann Intern Med 1985; 102: 194–6.
Leonard JN, Tucker WF, Fry JS, et al. Increased incidence of malignancy in dermatitis herpetiformis. Br Med J (Clin Res Ed) 1983; 286: 16–8.
Lewis HM, Renaula TL, Garioch JJ, et al. Protective effect of glutenfree diet against development of lymphoma in dermatitis herpetiformis. Br J Dermatol 1996; 135: 363–7.
Sigurgeirsson B, Agnarsson BA, Lindelöf B. Risk of lymphoma in patients with dermatitis herpetiformis. BMJ 1994; 308: 13–5.
Collin P, Pukkala E, Reunala T. Malignancy and survival in dermatitis herpetiformis: a comparison with coeliac disease. Gut 1996; 38: 528–30.
Hervonen K, Vornanen M, Kautiainen H, Collin P, Reunala T. Lymphoma in patients with dermatitis herpetiformis and their first-degree relatives. Br J Dermatol 2005; 152: 82–6.
Clarindo MV, Possebon AT, Soligo EM, Uyeda H, Ruaro RT, Empinotti JC. Dermatitis herpetiformis: pathophysiology, clinical presentation, diagnosis and treatment. An Bras Dermatol 2014; 89: 865–75, quiz: 876-7.
Fry L. Dermatitis herpetiformis: problems, progress and prospects. Eur J Dermatol 2002; 12: 523–31.
Tenenhouse A, Joseph L, Kreiger N, et al. Estimation of the prevalence of low bone density in Canadian women and men using a population-specific DXA reference standard: the Canadian Multicentre Osteoporosis Study (CaMos). Osteoporos Int 2000; 11: 897–904.
Looker AC, Wahner HW, Dunn WL, et al. Updated data on proximal femur bone mineral levels of US adults. Osteoporos Int 1998; 8: 468–89.
Boyanov MA. Prevalence of low central bone mineral density in a Bulgarian female referral population: a pilot study. Rheumatol Int 2006; 26: 523–9.
Pantaleoni S, Luchino M, Adriani A, et al. Bone mineral density at diagnosis of celiac disease and after 1 year of gluten-free diet. Scientific World Journal 2014; 2014: 173082.
Author information
Authors and Affiliations
Corresponding author
About this article

Cite this article
Lheure, C., Ingen-Housz-Oro, S., Guignard, S. et al. Dermatitis herpetiformis and bone mineral density: analysis of a French cohort of 53 patients. Eur J Dermatol 27, 353–358 (2017). https://doi.org/10.1684/ejd.2017.3029
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1684/ejd.2017.3029