
Abstract
Introduction
Although up to 50–70% of patients with intrahepatic cholangiocarcinoma (ICC) recur following resection, data to predict post-recurrence survival (PRS) and guide treatment of recurrence are limited.
Methods
Patients who underwent resection of ICC between 2000 and 2020 were identified from an international, multi-institutional database. Data on primary disease as well as laboratory and radiologic data on recurrent disease were collected. Factors associated with PRS were examined and a novel scoring system to predict PRS (PRS score) was developed and internally validated.
Results
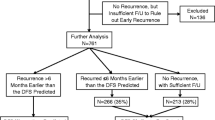
Among 986 individuals who underwent resection for ICC, 588 (59.6%) patients developed recurrence at a median follow up of 20.3 months. Among patients who experienced a recurrence, 97 (16.5%) underwent re-resection/ablation for recurrent ICC; 88 (15.0%) and 403 (68.5%) patients received intra-arterial treatment or systemic chemotherapy/supportive therapy, respectively. Patient American Society of Anesthesiologists (ASA) class > 2 (1 point), primary tumor N1/Nx status (1 point), primary R1 resection margin (1 point), primary tumor G3/G4 grade (1 point), carbohydrate antigen (CA) 19-9 > 37 UI/mL (2 points) at recurrence and carcinoembryonic antigen (CEA) > 5 ng/mL (2 points) at recurrence, as well as recurrent bilateral disease (1 point) and early recurrence (1 point) were included in the PRS score. The PRS score successfully stratified patients relative to PRS and demonstrated strong discriminatory ability (C-index 0.70, 95% confidence interval 0.68–0.72). While a PRS score of 0–3 was associated with a 3-year PRS of 62.5% following resection/ablation for recurrent ICC, a PRS score > 3 was associated with a low 3-year PRS of 35.5% (p = 0.03).
Conclusions
The PRS score demonstrated strong discriminatory ability to predict PRS among patients who had developed recurrence following initial resection of ICC. The PRS score may be a useful tool to guide treatment among patients with recurrent ICC.


Similar content being viewed by others

References
Singal AK, Vauthey JN, Grady JJ, Stroehlein JR. Intra-hepatic cholangiocarcinoma–frequency and demographic patterns: thirty-year data from the M.D. Anderson Cancer Center. J Cancer Res Clin Oncol. 2011;137(7):1071–8.
Wu L, Tsilimigras DI, Paredes AZ, et al. Trends in the incidence, treatment and outcomes of patients with intrahepatic cholangiocarcinoma in the USA: facility type is associated with margin status, use of lymphadenectomy and overall survival. World J Surg. 2019;43(7):1777–87.
Mavros MN, Economopoulos KP, Alexiou VG, Pawlik TM. Treatment and Prognosis for patients with intrahepatic cholangiocarcinoma: systematic review and meta-analysis. JAMA Surg. 2014;149(6):565–74.
Benson AB, D’Angelica MI, Abrams T, et al. NCCN guidelines(R) insights: biliary tract cancers, version 2.2023. J Natl Compr Cancer Netw. 2023;21(7):694–704.
Tsilimigras DI, Sahara K, Wu L, et al. Very early recurrence after liver resection for intrahepatic cholangiocarcinoma: considering alternative treatment approaches. JAMA Surg. 2020;155(9):823–31.
European Association for the Study of the Liver. Electronic address EEE, European Association for the Study of the L. EASL-ILCA Clinical Practice Guidelines on the management of intrahepatic cholangiocarcinoma. J Hepatol. 2023;79(1):181–208.
Tsilimigras DI, Moris D, Mehta R, et al. The systemic immune-inflammation index predicts prognosis in intrahepatic cholangiocarcinoma: an international multi-institutional analysis. HPB (Oxford). 2020;22(12):1667–74.
Strasberg SM. Nomenclature of hepatic anatomy and resections: a review of the Brisbane 2000 system. J Hepatobiliary Pancreat Surg. 2005;12(5):351–5.
Amin MB, Greene FL, Edge SB, et al. The Eighth Edition AJCC Cancer Staging Manual: continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA A Cancer J Clin. 2017;67(2):93–9.
de Jong MC, Nathan H, Sotiropoulos GC, et al. Intrahepatic cholangiocarcinoma: an international multi-institutional analysis of prognostic factors and lymph node assessment. J Clin Oncol. 2011;29(23):3140–5.
Endo I, Gonen M, Yopp AC, et al. Intrahepatic cholangiocarcinoma: rising frequency, improved survival, and determinants of outcome after resection. Ann Surg. 2008;248(1):84–96.
Maithel SK, Gamblin TC, Kamel I, Corona-Villalobos CP, Thomas M, Pawlik TM. Multidisciplinary approaches to intrahepatic cholangiocarcinoma. Cancer. 2013;119(22):3929–42.
Spolverato G, Vitale A, Cucchetti A, et al. Can hepatic resection provide a long-term cure for patients with intrahepatic cholangiocarcinoma? Cancer. 2015;121(22):3998–4006.
Yuan ZB, Fang HB, Feng QK, Li T, Li J. Prognostic factors of recurrent intrahepatic cholangiocarcinoma after hepatectomy: a retrospective study. World J Gastroenterol. 2022;28(15):1574–87.
Ohira M, Kobayashi T, Hashimoto M, et al. Prognostic factors in patients with recurrent intrahepatic cholangiocarcinoma after curative resection: a retrospective cohort study. Int J Surg. 2018;54(Pt A):156–62.
Si A, Li J, Xing X, et al. Effectiveness of repeat hepatic resection for patients with recurrent intrahepatic cholangiocarcinoma: factors associated with long-term outcomes. Surgery. 2017;161(4):897–908.
Bartsch F, Eberhard J, Ruckert F, et al. Repeated resection for recurrent intrahepatic cholangiocarcinoma: a retrospective German multicentre study. Liver Int. 2021;41(1):180–91.
Nickkholgh A, Ghamarnejad O, Khajeh E, et al. Outcome after liver resection for primary and recurrent intrahepatic cholangiocarcinoma. BJS Open. 2019;3(6):793–801.
Spolverato G, Kim Y, Alexandrescu S, et al. Management and outcomes of patients with recurrent intrahepatic cholangiocarcinoma following previous curative-intent surgical resection. Ann Surg Oncol. 2016;23(1):235–43.
Acknowledgements
None.
Funding
No sources of funding were used to assist in the preparation of this work.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This work was accepted as an E-Poster at the Society of Surgical Oncology (SSO) 2024 Annual Meeting, Atlanta, GA, USA.
Supplementary Information
Below is the link to the electronic supplementary material.
10434_2024_15210_MOESM1_ESM.pdf
Online Resource Fig. 1 Violin plot of recurrent disease treatment allocation relative to PRS score. The hollow dot represents the median value, the gray box represents the IQR, while gray lines indicate the minimum and maximum values. The width represents the frequency of observations. PRS Post-recurrence score, IQR Interquartile range (PDF 68 KB)
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Tsilimigras, D.I., Endo, Y., Guglielmi, A. et al. Recurrent Intrahepatic Cholangiocarcinoma: A 10-Point Score to Predict Post-Recurrence Survival and Guide Treatment of Recurrence. Ann Surg Oncol (2024). https://doi.org/10.1245/s10434-024-15210-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1245/s10434-024-15210-2