
Abstract
Background
Standard treatment for unresectable locally advanced esophageal cancer is definitive chemoradiotherapy (dCRT). Although salvage esophagectomy is the only curative treatment available following dCRT failure, the appropriate candidates for salvage esophagectomy remain unclear.
Patients and Methods
Three hundred seventeen patients who underwent dCRT from April 2004 to December 2016 were stratified into three study groups—a complete response (CR) group, chemotherapy or best supportive care (BSC) group, and salvage esophagectomy group—and compared. We also investigated the clinical outcomes and prognostic factors of salvage esophagectomy.
Results
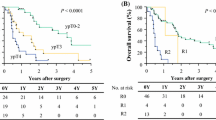
Seventy-one patients (22.4%) achieved CR after dCRT, 18 patients (5.7%) underwent salvage esophagectomy, and 228 patients (71.9%) underwent palliative chemotherapy or BSC. The 5-year overall survival (OS) rates of the CR group, salvage esophagectomy group, and chemotherapy or BSC group were 83.0%, 51.6%, and 1.3%, respectively. Salvage esophagectomy recipients had a worse OS rate than CR patients (p < 0.001) but a better OS rate than those in the chemotherapy or BSC group (p < 0.001). Incomplete resection was the only significant variable associated with poor OS on univariate Cox proportional-hazards analysis (hazard ratio: 7.633, 95% confidence interval: 1.692–34.482; p = 0.008). Patients with tumors in the upper thoracic esophagus were more likely to undergo incomplete resection (p = 0.011).
Conclusions
Patients who achieve R0 resection are good candidates for salvage esophagectomy regardless of their response to dCRT. Those with upper thoracic esophageal tumors are at risk of incomplete resection; careful attention is required when considering these patients for salvage esophagectomy.



Similar content being viewed by others


References
Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin. 2015;65:87–108.
Ando N, Ozawa S, Kitagawa Y, Shinozawa Y, Kitajima M. Improvement in the results of surgical treatment of advanced squamous esophageal carcinoma during 15 consecutive years. Ann Surg. 2000;232:225–32.
Kawakami T, Tsushima T, Omae K, et al. Risk factors for esophageal fistula in thoracic esophageal squamous cell carcinoma invading adjacent organs treated with definitive chemoradiotherapy: a monocentric case-control study. BMC Cancer. 2018;18:573.
Ohtsu A, Boku N, Muro K, et al. Definitive chemoradiotherapy for T4 and/or M1 lymph node squamous cell carcinoma of the esophagus. J Clin Oncol. 1999;17:2915–21.
Okamura A, Hayami M, Kozuki R, et al. Salvage esophagectomy for initially unresectable locally advanced T4 esophageal squamous cell carcinoma. Esophagus. 2019. https://doi.org/10.1007/s10388-019-00700-0
Kitagawa Y, Uno T, Oyama T, et al. Esophageal cancer practice guidelines 2017 edited by the Japan esophageal society: part 1. Esophagus. 2019;16:1–24.
Kitagawa Y, Uno T, Oyama T, et al. Esophageal cancer practice guidelines 2017 edited by the Japan Esophageal Society: part 2. Esophagus. 2019;16:25–43.
Brierley JD, Gospodarowicz MK, Wittekind C. TNM classification of malignant tumors: International Union against Cancer. 8th ed. Oxford: Wiley; 2017.
Shinoda M, Ando N, Kato K, et al. Randomized study of low-dose versus standard-dose chemoradiotherapy for unresectable esophageal squamous cell carcinoma (JCOG0303). Cancer Sci. 2015;106:407–12.
Therasse P, Arbuck SG, Eisenhauer EA, et al. New guidelines to evaluate the response to treatment in solid tumors. J Natl Cancer Inst. 2000;92:205–16.
Eisenhauer E, Therasse P, Bogaerts J, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45:228–47.
Japan Esophageal Society. Japanese classification of esophageal cancer, 11th ed. Part II and III. Esophagus. 2017;14:37–65.
Clavien PA, Barkun J, de Oliveira ML, et al. The Clavien–Dindo classification of surgical complications: five-year experience. Ann Surg. 2009;250:187–96.
Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240:205–13.
Tachimori Y, Kanamori N, Uemura N, Hokamura N, Igaki H, Kato H. Salvage esophagectomy after high-dose chemoradiotherapy for esophageal squamous cell carcinoma. J Thorac Cardiovasc Surg. 2009;137:49–54.
Watanabe M, Mine S, Nishida K, et al. Salvage esophagectomy after definitive chemoradiotherapy for patients with esophageal squamous cell carcinoma: Who really benefits from this high-risk surgery? Ann Surg Oncol. 2015;22:4438–44.
de Manzoni G, Pedrazzani C, Pasini F, et al. Chemoradiotherapy followed by surgery for squamous cell carcinoma of the thoracic esophagus with clinical evidence of adjacent organ invasion. J Surg Oncol. 2007;95:261–6.
Ikeda K, Ishida K, Sato N, et al. Chemoradiotherapy followed by surgery for thoracic esophageal cancer potentially or actually involving adjacent organs. Dis Esophagus. 2001;14:197–201.
Ohkura Y, Ueno M, Iizuka T, Udagawa H. Prognostic factors and appropriate lymph node dissection in salvage esophagectomy for locally advanced T4 esophageal cancer. Ann Surg Oncol. 2019;26:209–16.
Booka E, Takeuchi H, Nishi T, et al. The impact of postoperative complications on survivals after esophagectomy for esophageal cancer. Medicine. 2015;94:e1369.
Booka E, Takeuchi H, Suda K, et al. Meta-analysis of the impact of postoperative complications on survival after oesophagectomy for cancer. BJS Open. 2018;2:276–84.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosure
The authors declare that they have no conflicts of interest or funding to report in relation to this study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Booka, E., Haneda, R., Ishii, K. et al. Appropriate Candidates for Salvage Esophagectomy of Initially Unresectable Locally Advanced T4 Esophageal Squamous Cell Carcinoma. Ann Surg Oncol 27, 3163–3170 (2020). https://doi.org/10.1245/s10434-020-08440-7
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-020-08440-7