
Abstract
Background
The Prospective Surveillance Model (PSM) of rehabilitation for patients with breast cancer aims for early identification, treatment, and support of physical impairments postoperatively. The purpose of this study was to describe the incidence of impairments during the first postoperative year and the differences between the patients requiring rehabilitation intervention versus those not requiring intervention.
Methods
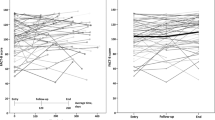
A total of 120 patients were enrolled. Impairment measures included: pain, range of motion, and self-reported measures of function using the Upper Extremity Functional Index (UEFI) and Quick Disability of the Arm, Shoulder and Hand (QuickDASH) questionnaires. These measures were performed at designated intervals during the first postoperative year. All patients received exercise and education, and patients with identified impairments underwent individualized rehabilitation intervention. Clinical factors associated with need for intervention were determined using univariate analysis.
Results
Thirty-six patients required rehabilitation intervention. There were no statistically significant differences between intervention and no-intervention groups for body mass index, breast surgery type, reconstruction type, or radiotherapy. Statistically significant differences were found between intervention and no-intervention groups in early postoperative UEFI, QuickDASH, pain scores, age, number of lymph nodes removed [9.3 (intervention) vs. 5.6 (no-intervention)], axillary surgery type, chemotherapy, and breast cancer stage.
Conclusions
Survivorship practitioners should have heightened awareness for rehabilitation intervention in patients with greater axillary surgery and burden of disease. Patients with more activity restriction and lower levels of function in the early postoperative period may benefit from rehabilitation intervention. Future studies should focus on implementing a screening tool to identify patients in need of rehabilitation referral.

Similar content being viewed by others


References
Petrek JA, Senie RT, Peters M, Rosen PP. Lymphedema in a cohort of breast carcinoma survivors 20 years after diagnosis. Cancer. 2001;92:1368–77.
Stout NL, Binkley JM, Schmitz KH, et al. A prospective surveillance model for rehabilitation for women with breast cancer. Cancer. 2012;118:2191–200.
Stratford PW, Binkley JM, Stratford DM. Development and initial validation of the upper extremity functional index. Physiother Can. 2001;53:259–67.
Kennedy CA, Beaton DE, Solway S, McConnell S, Bombardier C. Disabilities of the arm, shoulder and hand (DASH). The DASH and QuickDASH Outcome Measure User’s Manual. 3rd ed. Institute for Work and Health: Toronto; 2011.
Cowher MS, Grobmyer SR, Lyons J, O’Rourke C, Baynes D, Crowe JP. Conservative axillary surgery in breast cancer patients undergoing mastectomy: long-term results. J Am Coll Surg. 2014;218:818–24.
DiSipio T, Rye S, Newman B, Hayes S. Incidence of unilateral arm lymphoedema after breast cancer: a systematic review and meta-analysis. Lancet Oncol. 2013;14:500–15.
Hack TF, Kwan WB, Thomas-Maclean RL, Towers A, Miedema B, Tilley A, Chateau D. Predictors of arm morbidity following breast cancer surgery. Psycho-Oncology. 2010;19:1205–12.
Herd-Smith A, Russo A, Muraca MG, Del Turco MR, Cardona G. Prognostic factors for lymphedema after primary treatment of breast carcinoma. Cancer. 2001;92:1783–7.
Kiel KD, Rademacker AW. Early-stage breast cancer: arm edema after wide excision and breast irradiation. Radiology. 1996;198:279–83.
Miller CL, Specht MC, Skolny MN, et al. Risk of lymphedema after mastectomy: potential benefit of applying ACOSOG Z0011 protocol to mastectomy patients. Breast Cancer Res Treat. 2014;144:71–7.
Paskett ED, Naughton MJ, McCoy TP, Case LD, Abbott JM. The epidemiology of arm and hand swelling in premenopausal breast cancer survivors. Cancer Epidemiol Biomark Prev. 2007;16:775–82.
Mansel RE, Fallowfield L, Kissin M, et al. Randomized multicenter trial of sentinel node biopsy versus standard axillary treatment in operable breast cancer: the ALMANAC trial. J Natl Cancer Inst. 2006;98:599–609.
McLaughlin SA, Wright MJ, Morris KT, et al. Prevalence of lymphedema in women with breast cancer 5 years after sentinel lymph node biopsy or axillary dissection: objective measurements. J Clin Oncol. 2008;26:5213–9.
Tsai RJ, Dennis LK, Lynch CF, Snetselaar LG, Zamba GK, Scott-Conner C. The risk of developing arm lymphedema among breast cancer survivors: a meta-analysis of treatment factors. Ann Surg Oncol. 2009;16:1959–72.
Sclafani LM, Baron RH. Sentinel lymph node biopsy and axillary dissection: added morbidity of the arm, shoulder and chest wall after mastectomy and reconstruction. Cancer J. 2008;14:216–22.
Lee MJ, Beith J, Ward L, Kilbreath S. Lymphedema following taxane-based chemotherapy in women with early breast cancer. Lymphat Res Biol. 2014;12:282–8.
Swaroop MN, Ferguson CM, Horick NK, et al. Impact of adjuvant taxane-based chemotherapy on development of breast cancer-related lymphedema: results from a large prospective cohort. Breast Cancer Res Treat. 2015;151:393–403.
Avraham T, Daluvoy SV, Riedel ER, Cordeiro PG, Van Zee KJ, Mehrara BJ. Tissue expander breast reconstruction is not associated with an increased risk of lymphedema. Ann Surg Oncol. 2010;17:2926–32.
Basta MN, Fischer JP, Kanchwala SK, et al. A propensity-matched analysis of the influence of breast reconstruction on subsequent development of lymphedema. Plast Reconstr Surg. 2015;136:134e–43e.
Blanchard M, Arrault M, Vignes S. Positive impact of delayed breast reconstruction on breast-cancer treatment-related arm lymphoedema. J Plast Reconstr Aesthet Surg. 2012;65:1060–3.
Powell SN, Taghian AG, Kachnic LA, Coen JJ, Assaad SI. Risk of lymphedema after regional nodal irradiation with breast conservation therapy. Int J Radiat Oncol Biol Phys. 2003;55:1209–15.
Borup Christensen S, Lundgren E. Sequelae of axillary dissection vs. axillary sampling with or without irradiation for breast cancer A randomized trial. Acta Chir Scand. 1989;155:515–9.
Donker M, van Tienhoven G, Straver ME, et al. Radiotherapy or surgery of the axilla after a positive sentinel node in breast cancer (EORTC 10981-22023 AMAROS): a randomized, multicenter, open-label, phase 3 non-inferiority trial. Lancet Oncol. 2014;15:1303–10.
Acknowledgment
This study was funded by a grant from the Avon Foundation. We additionally acknowledge the Avon patient navigators, TurningPoint Breast Cancer Rehabilitation for donation of supplies and equipment, and medical student Austin Eckhoff for assistance with data collection.
Disclosure of any financial interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Lai, L., Binkley, J., Jones, V. et al. Implementing the Prospective Surveillance Model (PSM) of Rehabilitation for Breast Cancer Patients with 1-Year Postoperative Follow-up, a Prospective, Observational Study. Ann Surg Oncol 23, 3379–3384 (2016). https://doi.org/10.1245/s10434-016-5315-z
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-016-5315-z