
Abstract
Background
People with prediabetes or type 2 diabetes (T2D) need to be physically active, including moderate-to-vigorous intensity physical activity (MVPA) and light-intensity physical activity (LIPA) and reduce time in sedentary behaviour (SB). Few studies have evaluated the effect of randomised controlled trials taking all movement behaviours into account. This study aimed to investigate the effects of a 2-year pedometer-based intervention in people with prediabetes or T2D on relative time in movement behaviours.
Methods
Secondary analysis of longitudinal data on individuals with prediabetes or T2D from a three-armed randomised controlled trial, the Sophia Step Study, was conducted. The three groups were (1) a multi‑component group (self‑monitoring of steps with a pedometer plus counselling), (2) a single‑component group (self‑monitoring of steps with a pedometer, without counselling), and (3) a standard care group (control). The three behaviours MVPA, LIPA and SB during waking hours were measured with an ActiGraph GT1M accelerometer at baseline, 6, 12, 18 and 24 months. Relative time in MVPA, LIPA and SB for each participant at each time point was calculated and used as outcome measures. Linear mixed models assessed the effect of the intervention over time.
Results
In total 184 participants with mean (SD) age 64.3 (7.6) years and 41% female was included. In the multi-component group, compared to the control group, a significant group-by-time interaction effect for relative time in all three behaviours was found at 6 and 18 months and for MVPA and SB at 24 months. In the single-component group, compared to the control group, an effect occurred in the MVPA and SB behaviours at 6 months and MVPA and LIPA at 24 months. The estimated marginal means ranged from 0.9 to 1.5% of more MVPA, 1.9–3.9% of less LIPA and from 0.5% of less SB to 1.7 more SB in the intervention groups compared to the control group.
Conclusions
The findings show a beneficial effect on all behaviours over time in the two intervention groups compared to the control group. A more pronounced effect occurred in the multi-component intervention compared to the single-component intervention, implicating the importance of counselling in pedometer-based interventions.
Trial registration ClinicalTrials.gov, NCT02374788
Similar content being viewed by others

Background
The prevalence of prediabetes and type 2 diabetes (T2D) is rising globally [1]. Regular physical activity is associated with preventing and controlling the disease [2, 3]. However, most people with prediabetes or T2D do not meet recommended physical activity levels [4,5,6]. One way to reach this patient group is by using primary care as an arena [7], together with interventions using pedometers as a motivational tool. Pedometers has been shown to have a positive short-term effect on increasing physical activity [8,9,10,11,12,13]. For people with T2D, the intensity of physical activity seems especially relevant. Time in moderate-to-vigorous intensity physical activity (MVPA) and light-intensity physical activity (LIPA) is linked to better cardiovascular risk profiles, while the opposite occurs in sedentary behaviour (SB) [14]. In addition, a decrease in prolonged SB and an increase in MVPA are associated with reduced HbA1c levels [15].
Accelerometers, which generate data in different intensities, are commonly used to assess physical activity [16]. The MVPA, LIPA and SB intensities can be expressed as interdependent movement behaviours, i.e., if time in one movement behaviour increases, time in other movement behaviours decreases, given that time is an invariant quantity. Analysing movement behaviours as separate isolated behaviours, with each behaviour in absolute time, is the most commonly applied method. However, analysis methods with relative time in each behaviour in relation to the other movement behaviours should be considered [17, 18]. Using absolute time can lead to an incomplete picture of movement behaviours. Also, more studies using relative time in different populations (e.g., T2D) are needed [19]. The most beneficial effects in people with prediabetes or T2D would be an increase in MVPA concomitant with a decrease in SB. Interrupting extended periods of SB and replacing them with LIPA can benefit glucose control [20] and blood pressure [21]. To our knowledge, only few studies have evaluated the effect of randomised controlled trials (RCTs) with an outcome based on relative time and where all movement behaviours are considered [22,23,24].
The Sophia Step Study was a 2-year, three-armed pedometer-based intervention developed for primary care to support individuals with prediabetes or T2D to become physically active by regularly increasing their daily number of steps [25]. The 2-year effect of the intervention was assessed earlier using absolute time in each movement behaviour as the outcome [26]. However, because these analyses were conducted with absolute time in each movement behaviour and did not consider the relative time of the three behaviours, the results do not show the entire picture of how the behaviours change over time in relation to each other. Therefore, this study examines the effects of a 2-year pedometer-based intervention in people with prediabetes or T2D on relative time in different movement behaviours.
Methods
Study design and population
This study is a secondary analysis of the RCT Sophia Step Study [25]. Data were collected between 2013 and 2020. Participants were recruited from one rural and two urban primary care centres in Sweden by their diabetes nurse and randomised to one of the two intervention groups or the control group by sealed envelopes. All participants signed written informed consent prior to participation. Demographics and data on health conditions and medications were collected by a questionnaire and from patient medical records at baseline. The inclusion criteria were HbA1c > 39 mmol/mol or fasting glucose > 5.6 mmol/l, 40–80 years of age and fluency in Swedish. Exclusion criteria were myocardial infarction in the past 6 months, serum creatinine > 140 mmol/l, diabetic foot ulcer or risk of ulcer (severe peripheral neuropathy), patients newly prescribed insulin (< 6 months), other disease prohibiting physical activity, suffering repeated hypoglycaemia or severe hypoglycaemia in the past 12 months, very physically active according to the Stanford Brief Activity Survey [27] and those with no access to the internet.
Intervention
The 2-year intervention was developed for the primary care context to support individuals with prediabetes or T2D to become physically active regularly. The RCT was three-armed with a multi-component intervention group that self-monitored their daily steps with a pedometer and registered them on a web-based platform. They were also offered group and individual counselling. The counselling was most intense for the first year (eight individual and ten group sessions) compared to the second year (two individual and two group sessions). A second group was offered a single-component intervention, including only self-monitoring and registration of daily steps. The third group was a control group receiving usual care. Details of the intervention and data collection can be found elsewhere [25].
Measurement of movement behaviours
Time spent in MVPA, LIPA and SB was measured objectively using the ActiGraph GT1M accelerometer (ActiGraph, Pensacola, FL). Participants wore the accelerometer during waking hours. The accelerometer was placed on the participants’ lower back [28] for seven consecutive days at five time points (0 [baseline], 6, 12, 18 and 24 months). Additionally, the participants logged their daily wear time in a diary. The diaries were used to verify wear time and the number of valid days. The accelerations were sampled at 10 Hz and summed over 60 s using the software ActiLife v.6.13.4. Non-wear time was set to > 90 min (min) of consecutive zero counts, allowing for 2 min of nonzero counts [29]. Data were included for participants with ≥ 3 days and ≥ 10 h per day of valid wear time [30]. Wear time was allocated into activity categories based on count-based thresholds: SB < 100 counts per min (cpm) [31], LIPA 100–1951 cpm and MVPA ≥ 1952 cpm [32].
Statistical analysis
All analyses were conducted using the R statistical system version 1.2.5019 and IBM SPSS version 27.0. Difference between groups at baseline were assessed with Chi-square test for categorical variables and ANOVA for continuous variables. Linear mixed models were used to investigate change in relative time in each movement behaviour (MVPA, LIPA, SB) in the three groups. Compositional means of time spent in MVPA, LIPA and SB were calculated by creating the geometric mean and summarising the behaviours to 100%. The daily time for each participant was expressed as a set of two isometric log-ratio (ilr) coordinates, including all relative information about the three compositional parts, as exemplified below for MVPA.

A separate linear mixed model for relative time in each movement behaviour (MVPA, LIPA, SB) was conducted with the ilr1 variable for each behaviour as the outcome and 95% confidence intervals (CIs). This approach has been used elsewhere [22]. Participants were included as a random effect, age, randomisation group, time (as a categorical variable) and time by randomisation group interaction as fixed factors. Point estimates from the marginal means from the linear mixed models were back transformed into a percentage. The percentages from the three movement behaviours were adjusted to sum up to 100%. Contrast between baseline and 24 months were performed for relative time in each movement behaviour (MVPA, LIPA, SB).
Results
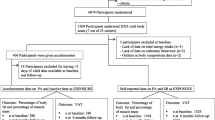
In total 184 participants fulfilled the inclusion criteria and were randomised into the two intervention and control group. Figure 1 displays the number of participants with valid accelerometer data in each group at each time point. Table 1 presents the baseline participant characteristics by intervention group. Overall, 22% of the participants had prediabetes: mean (± SD) age was 64 ± 7.5 years, 41% were female and 47% had a university education. No statistically significant differences between the groups were found at baseline.

Flowchart of the number of participants with valid accelerometer data at each time point
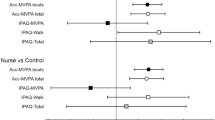
Table 2 shows the intervention effect over time between the two intervention groups and the control group. Overall, the effect over time favoured the intervention groups, although there was some variation in the magnitude of the effects at the different time points. In the multi-component group, compared to the control group, the intervention reached a statistically significant effect (interaction between time and group) on the relative time at 6 and 18 months in MVPA, LIPA and SB and for relative time at 24 months in MVPA and SB. In the single-component group compared with the control group, the intervention reached a statistically significant effect on relative time at 6 months in MVPA and SB and 24 months in MVPA and LIPA. For the control group, the within-group mean difference between baseline and 24 months showed a significant decrease in relative time in MVPA and an increase in relative time in LIPA and SB, see details in Table 3. No significant within-group changes were found between baseline and 24 months in the multi- or single-component groups. Table 4 lists relative time in per cent with 95% CIs for all movement behaviours for each group and measurement point based on the back-transformed point estimates from the linear mixed model. Figure 2 depicts changes in relative time in the movement behaviours over the 2-year study period (based on the numbers listed in Table 4).

Changes in the relative time in per cent with 95% confidence intervals in movement behaviours over the 2-year study period. Values and related confidence intervals are based on the predicted group means from the linear mixed model analysis. MVPA moderate-to-vigorous intensity physical activity, LIPA light-intensity physical activity, SB sedentary behaviour
Discussion
This study investigated the effects of a 2-year pedometer-based intervention in people with prediabetes or T2D on relative time in movement behaviours. We found an intervention effect on all behaviours targeted in both intervention groups, although some variations in the magnitude and time point of the effects were noted. In the multi-component group an effect for all targeted behaviours was seen at 6 and 18 months; for the MVPA and SB behaviours, an effect was found at 24 months. In the single-component group an effect occurred at 6 months for MVPA and SB and 24 months for MVPA and LIPA. At these time points, the estimated marginal means (transformed into per cent) ranged from 0.9 to 1.5% of more MVPA, 1.9 to 3.9% of less LIPA and from 0.5% of less SB to 1.7 more SB in the intervention groups compared to the control group. Assuming that the participants were awake 16 h per day, these differences in percentages correspond to 9 to 15 min/day in more MVPA, 18 to 37 min/day in less LIPA and 5 min/day less SB to 16 min/day more SB in the intervention groups compared to the control group.
The magnitude of our results seems to be larger and longer lasting compared to other pedometer-based interventions evaluating physical activity behaviours using absolute time in people with prediabetes or T2D [33,34,35]. These studies have shown mixed results ranging from no effect to a small effect (MVPA + 3.5 min/day, LIPA + 5.1 to + 14.1 min/day, SB − 5.2 to − 14.4 min/day) at 6 or 12 months. Yet, the effects were not sustained in the long run (up to 48 months). Moreover, systematic reviews have concluded that pedometer-based interventions, often together with counselling, can positively impact increasing physical activity in people with T2D [10, 13]. However, the effects were only evident during the intervention period [13].
Moreover, the within-group mean difference between baseline and 24 months showed that the control group decreased the relative time in MVPA, which was compensated by increased relative time in LIPA and SB. This trend was not observed in the multi-component or single-component groups. Another pedometer-based intervention found an increase in SB and LIPA. At the same time, MVPA decreased in the control group [34], suggesting that pedometer-based interventions can help prevent unhealthy physical activity behaviours from developing over time.
The present findings should be viewed in relation to our previous study, in which our outcome measures were absolute time of each behaviour. This earlier study found significant intervention effects only in MVPA: at all time points in the multi-component group and at the 6-month time point in the single-component group. No intervention effects were found in LIPA or SB [26]. For people with prediabetes or T2D, increased time in MVPA and decreased time in SB seem necessary to improve glucose control [6, 36], raising the possibility that using relative time could be a preferred option to present a more thorough conceptualisation of how all movement behaviours are affected by interventions.
Given all movement behaviours taken together, the most beneficial change can be seen in the multi-component group at 6 and 18 months, with increased relative time in MVPA and decreased relative time in LIPA and SB. However, the improvements seem to return to baseline values at 24 months. The individual and group counselling interventions were most intense during the first year, indicating the need for continuous follow-up [37].
Results have varied in other population groups depending on whether relative or absolute time was used. Chastin et al., for instance, found a difference of about 10 min in MVPA when they compared relative to absolute mean times in cross-sectional data [17]. Gupta et al. analysed time spent in SB, standing and physical activity during work and leisure in cross-sectional data using relative and absolute time approaches. They concluded that effect sizes could differ, favouring the relative time approach, even if the results with both techniques were significant [38]. Other RCTs have used both relative and absolute time or absolute time alone to evaluate the effect of physical activity interventions. Pasanen et al. did not find any effect of an activity tracker intervention when they used relative time at 6 months [23] or absolute time at 12 months [39, 40]. Another RCT that reduced office workers’ sitting time found a significant effect when a relative and absolute time approach was used [24, 41]. A recent RCT examined the effect of physical activity and SB interventions on office workers. The authors could not find any effect on relative time in physical activity behaviours [22].
Strengths and limitations
The main strengths of this study are the longitudinal design, the use of device-based measures for movement and having relative time in all three behaviours as outcomes, as this considers the complex nature of physical activity [17]. A limitation of this study was that we did not measure sleep time, making it impossible to address 24-h movement behaviour patterns. However, this would not affect the intervention effect between the groups due to equal groups by the RCT design of the study. Also, the baseline values indicate that the participants were already active at baseline (mean MVPA in the entire group was 29.3 min per day). Thus, we might have failed to reach the inactive people who could benefit most from this type of intervention. Using accelerometers includes limitations, such as the failure to detect activities (e.g., bicycling and muscle-strengthening activities). Finally, the fact that participants were aware of being measured can affect their behaviour during the measurement period, leading to a failure to capture actual behaviours.
Conclusion
In this study relative time was used to evaluate the effects of a physical activity intervention. The findings show a beneficial effect on all movement behaviours over time in both intervention groups, with a more pronounced effect in the multi-component group. The control group had a negative trend in change and compensation among the behaviours over time, implying that counselling should be a key component in pedometer-based interventions. Using relative time as the outcome measure provides a more comprehensive assessment of the pattern of change in physical activity interventions, than using absolute time.
Availability of data and materials
The datasets generated or analysed during the current study are not publicly available because the data can be traced back to the study participants. According to Swedish and EU data legislation, access can only be granted upon a reasonable request. The request should be addressed to the PI and will be handled on a case‑by‑case basis. Data sharing will be regulated via a data transfer and use agreement with the recipient.
References
International Diabetes Federation. IDF Diabetes Atlas. Brussels, Belgium; 2021.
Cosentino F, Grant PJ, Aboyans V, Bailey CJ, Ceriello A, Delgado V, et al. 2019 ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD. Eur Heart J. 2019.
Savikj M, Zierath JR. Train like an athlete: applying exercise interventions to manage type 2 diabetes. Diabetologia. 2020;63(8):1491–9.
Zethelius B, Gudbjornsdottir S, Eliasson B, Eeg-Olofsson K, Cederholm J. Level of physical activity associated with risk of cardiovascular diseases and mortality in patients with type-2 diabetes: report from the Swedish National Diabetes Register. Eur J Prev Cardiol. 2014;21(2):244–51.
Kennerly A-M, Kirk A. Physical activity and sedentary behaviour of adults with type 2 diabetes: a systematic review. Practical Diabet. 2018;35(3):86–9.
Swindell N, Mackintosh K, McNarry M, Stephens JW, Sluik D, Fogelholm M, et al. Objectively measured physical activity and sedentary time are associated with cardiometabolic risk factors in adults with prediabetes: the PREVIEW study. Diabetes Care. 2018;41(3):562–9.
Milton K, Cavill N, Chalkley A, Foster C, Gomersall S, Hagstromer M, et al. Eight investments that work for physical activity. J Phys Act Health. 2021;18(6):625–30.
Qiu S, Cai X, Chen X, Yang B, Sun Z. Step counter use in type 2 diabetes: a meta-analysis of randomized controlled trials. BMC Med. 2014;12:36.
Vaes AW, Cheung A, Atakhorrami M, Groenen MT, Amft O, Franssen FM, et al. Effect of ‘activity monitor-based’ counseling on physical activity and health-related outcomes in patients with chronic diseases: a systematic review and meta-analysis. Ann Med. 2013;45(5–6):397–412.
Baskerville R, Ricci-Cabello I, Roberts N, Farmer A. Impact of accelerometer and pedometer use on physical activity and glycaemic control in people with Type 2 diabetes: a systematic review and meta-analysis. Diabet Med. 2017;34:612–20.
Hodkinson A, Kontopantelis E, Adeniji C, van Marwijk H, McMillan B, Bower P, et al. Accelerometer- and pedometer-based physical activity interventions among adults with cardiometabolic conditions: a systematic review and meta-analysis. JAMA Netw Open. 2019;2(10): e1912895.
Franssen WMA, Franssen G, Spaas J, Solmi F, Eijnde BO. Can consumer wearable activity tracker-based interventions improve physical activity and cardiometabolic health in patients with chronic diseases? A systematic review and meta-analysis of randomised controlled trials. Int J Behav Nutr Phys Activity. 2020;17(1):57.
Alothman S, Yahya A, Rucker J, Kluding PM. Effectiveness of interventions for promoting objectively measured physical activity of adults with type 2 diabetes: a systematic review. J Phys Act Health. 2017;14(5):408–15.
Balducci S, D’Errico V, Haxhi J, Sacchetti M, Orlando G, Cardelli P, et al. Level and correlates of physical activity and sedentary behavior in patients with type 2 diabetes: a cross-sectional analysis of the Italian Diabetes and Exercise Study_2. PLoS ONE. 2017;12(3): e0173337.
Garcia JM, Cox D, Rice DJ. Association of physiological and psychological health outcomes with physical activity and sedentary behavior in adults with type 2 diabetes. BMJ Open Diabetes Res Care. 2017;5(1): e000306.
Migueles JH, Cadenas-Sanchez C, Ekelund U, Delisle Nystrom C, Mora-Gonzalez J, Lof M, et al. Accelerometer data collection and processing criteria to assess physical activity and other outcomes: a systematic review and practical considerations. Sports Med (Auckland, NZ). 2017;47(9):1821–45.
Chastin SF, Palarea-Albaladejo J, Dontje ML, Skelton DA. Combined effects of time spent in physical activity, sedentary behaviors and sleep on obesity and cardio-metabolic health markers: a novel compositional data analysis approach. PLoS ONE. 2015;10(10): e0139984.
Dumuid D, Pedišić Ž, Palarea-Albaladejo J, Martín-Fernández JA, Hron K, Olds T. Compositional Data Analysis in Time-Use Epidemiology: What, Why, How. International journal of environmental research and public health. 2020;17(7).
Chastin SFM, McGregor DE, Biddle SJH, Cardon G, Chaput JP, Dall PM, et al. Striking the right balance: evidence to inform combined physical activity and sedentary behavior recommendations. J Phys Activity Health. 2021:1–7.
Dempsey PC, Blankenship JM, Larsen RN, Sacre JW, Sethi P, Straznicky NE, et al. Interrupting prolonged sitting in type 2 diabetes: nocturnal persistence of improved glycaemic control. Diabetologia. 2017;60(3):499–507.
Dempsey PC, Sacre JW, Larsen RN, Straznicky NE, Sethi P, Cohen ND, et al. Interrupting prolonged sitting with brief bouts of light walking or simple resistance activities reduces resting blood pressure and plasma noradrenaline in type 2 diabetes. J Hypertens. 2016;34(12):2376–82.
Larisch L-M, Bojsen-Møller E, Nooijen CFJ, Blom V, Ekblom M, Ekblom Ö, et al. Effects of two randomized and controlled multi-component interventions focusing On 24-hour movement behavior among office workers: a compositional data analysis. Int J Environ Res Public Health. 2021;18(8):4191.
Pasanen J, Leskinen T, Suorsa K, Pulakka A, Virta J, Auranen K, et al. Effects of physical activity intervention on 24-h movement behaviors: a compositional data analysis. Sci Rep. 2022;12(1):8712.
Stephens SK, Winkler EAH, Eakin EG, Clark BK, Owen N, Moodie M, et al. Temporal features of sitting, standing and stepping changes in a cluster-randomised controlled trial of a workplace sitting-reduction intervention. Int J Behav Nutr Phys Activity. 2019;16(1):111.
Rossen J, Yngve A, Hagstromer M, Brismar K, Ainsworth BE, Iskull C, et al. Physical activity promotion in the primary care setting in pre- and type 2 diabetes—the Sophia step study, an RCT. BMC Public Health. 2015;15:647.
Rossen J, Larsson K, Hagströmer M, Yngve A, Brismar K, Ainsworth B, et al. Effects of a three-armed randomised controlled trial using self-monitoring of daily steps with and without counselling in prediabetes and type 2 diabetes-the Sophia Step Study. Int J Behav Nutr Phys Activity. 2021;18(1):121.
Taylor-Piliae RE, Norton LC, Haskell WL, Mahbouda MH, Fair JM, Iribarren C, et al. Validation of a new brief physical activity survey among men and women aged 60–69 years. Am J Epidemiol. 2006;164(6):598–606.
Yngve A, Nilsson A, Sjostrom M, Ekelund U. Effect of monitor placement and of activity setting on the MTI accelerometer output. Med Sci Sports Exerc. 2003;35(2):320–6.
Choi L, Liu Z, Matthews CE, Buchowski MS. Validation of accelerometer wear and nonwear time classification algorithm. Med Sci Sports Exerc. 2011;43(2):357–64.
Hart TL, Swartz AM, Cashin SE, Strath SJ. How many days of monitoring predict physical activity and sedentary behaviour in older adults? Int J Behav Nutr Phys Activity. 2011;8:62.
Matthews CE, Chen KY, Freedson PS, Buchowski MS, Beech BM, Pate RR, et al. Amount of time spent in sedentary behaviors in the United States, 2003–2004. Am J Epidemiol. 2008;167(7):875–81.
Freedson PS, Melanson E, Sirard J. Calibration of the computer science and applications, Inc. accelerometer. Med Sci Sports Exercise. 1998;30(5):777–81.
Khunti K, Griffin S, Brennan A, Dallosso H, Davies MJ, Eborall HC, et al. Promoting physical activity in a multi-ethnic population at high risk of diabetes: the 48-month PROPELS randomised controlled trial. BMC Med. 2021;19(1):130.
De Greef KP, Deforche BI, Ruige JB, Bouckaert JJ, Tudor-Locke CE, Kaufman JM, et al. The effects of a pedometer-based behavioral modification program with telephone support on physical activity and sedentary behavior in type 2 diabetes patients. Patient Educ Couns. 2011;84(2):275–9.
Yates T, Edwardson CL, Henson J, Gray LJ, Ashra NB, Troughton J, et al. Walking Away from Type 2 diabetes: a cluster randomized controlled trial. Diabet Med. 2017;34(5):698–707.
Moghetti P, Balducci S, Guidetti L, Mazzuca P, Rossi E, Schena F. Walking for subjects with type 2 diabetes: a systematic review and joint AMD/SID/SISMES evidence-based practical guideline. Nutr Metab Cardiovasc Dis. 2020;30(11):1882–98.
Kettle VE, Madigan CD, Coombe A, Graham H, Thomas JJC, Chalkley AE, et al. Effectiveness of physical activity interventions delivered or prompted by health professionals in primary care settings: systematic review and meta-analysis of randomised controlled trials. BMJ (Clinical research ed). 2022;376: e068465.
Gupta N, Mathiassen SE, Mateu-Figueras G, Heiden M, Hallman DM, Jorgensen MB, et al. A comparison of standard and compositional data analysis in studies addressing group differences in sedentary behavior and physical activity. Int J Behav Nutr Phys Activity. 2018;15(1):53.
Leskinen T, Suorsa K, Tuominen M, Pulakka A, Pentti J, Löyttyniemi E, et al. The effect of consumer-based activity tracker intervention on physical activity among recent retirees-an RCT study. Med Sci Sports Exerc. 2021;53(8):1756–65.
Suorsa K, Leskinen T, Pulakka A, Pentti J, Löyttyniemi E, Heinonen I, et al. The effect of a consumer-based activity tracker intervention on accelerometer-measured sedentary time among retirees: a randomized controlled REACT trial. J Gerontol A Biol Sci Med Sci. 2022;77(3):579–87.
Healy GN, Eakin EG, Owen N, Lamontagne AD, Moodie M, Winkler EA, et al. A cluster randomized controlled trial to reduce office workers’ sitting time: effect on activity outcomes. Med Sci Sports Exerc. 2016;48(9):1787–97.
Acknowledgements
We thank all study participants engaged in the Sophia Step Study and the diabetes specialist nurses.
Funding
Open access funding provided by Sophiahemmet University College. This work was supported by the Sophiahemmet Foundation, Forte (Vårdalsstiftelsen), the Skandia and Sibling Svensson’s Foundation for Medical Research, The Swedish Diabetes Foundation and the King Gustav V and Queen Victoria’s Order of Freemasons Research Foundation. The funders had no role in the study design or conduct, data collection, analysis or interpretation, management, manuscript preparation, review or approval.
Author information
Authors and Affiliations
Contributions
KL designed the study in collaboration with MH, U-BJ, PvR and JR. JR collected the data and KL performed the analysis in collaboration with PvR. KL drafted the manuscript and all authors made substantial contributions to the content by reviewing and revising the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Swedish Ethical Review Authority in Stockholm (Dnr.2012/1570-31/3) and complied with the Declaration of Helsinki. All participants signed informed consent prior to enrolment.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Larsson, K., Von Rosen, P., Rossen, J. et al. Relative time in physical activity and sedentary behaviour across a 2-year pedometer-based intervention in people with prediabetes or type 2 diabetes: a secondary analysis of a randomised controlled trial. JASSB 2, 10 (2023). https://doi.org/10.1186/s44167-023-00020-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s44167-023-00020-w