
Abstract
Background
The respiratory system is the most frequently affected system by COVID-19. However, a variety of extra-pulmonary systems can be influenced by COVID-19 with subsequent morbidity and mortality.
Aim
This study aim is to report the most frequent extra pulmonary presentations of COVID-19 with comparison to patients with primary pulmonary presentation. Risk factors for ICU admission in both groups were examined.
Methods
In this prospective comparative cross-sectional study, detailed demographics, medical history, clinical assessment, and computed tomography (CT) scan of the chest were done to all recruited patients with COVID-19.
Result
This study included a total of 1664 confirmed COVID-19 patients. The patients were categorized into two groups. Patients with pulmonary manifestations included 716 patients while 948 patients presented with extrapulmonary manifestations. Patients in the extrapulmonary group were older. The prevalence of certain chronic comorbid conditions was higher in the extra pulmonary group as cardiac, CNS, hepatic, and renal diseases, while chronic respiratory disorders were more prevalent in the pulmonary group (P value: < 0.0001). No significant difference in CT severity score between both groups. CORAD 5 was predominant in the pulmonary group (P value: < 0.0001). Most cases in both groups required hospital admission either inward or in ICU with higher frequency of ICU admission was observed in the pulmonary group. The significant risk factors for ICU admission in both groups were critically ill category of patients, CT severity, low oxygen saturation level, and the presence of comorbid chronic disease (P < 0.0001 with adjusted Odds ratio). CNS, cardiac, renal, and metabolic dysfunctions exert significant risk for ICU admission in the extrapulmonary group.
Conclusion
Atypical or non-respiratory manifestations could be the presentation of a respiratory pathogen as reported in COVID-19. Our work highlights the extrapulmonary presentation of COVID-19. Older male patients were more prone to present with extra pulmonary symptoms. CNS, cardiac, renal, and metabolic dysfunctions were the most affected systems. This could impact the level of care required for patient management and the extent of resource utility.
Similar content being viewed by others


Introduction
The respiratory system is the most frequently affected system by COVID-19. Similar to SARS and MERS; fever, cough, dyspnea and sore throat were the most common clinical manifestations [1, 2]. Acute respiratory distress syndrome (ARDS) complicates some severe cases which carries high mortality [3]. However, a variety of extrapulmonary systems can be influenced by COVID-19 with subsequent morbidity and mortality.
Recent studies concluded that older patients who diagnosed with COVID-19 presented more commonly with extrapulmonary manifestations than young patients [4]. Various system affections were reported. This included acute kidney injury [5], gastrointestinal manifestations [6], pulmonary embolism [7], and neurological consequences [8].
As regard the pathogenesis of infection, the attachment of SARS-CoV-2 virus to the angiotensin-converting enzyme 2 receptor (ACEI2) is the portal into the host cell. These receptors are present in lung tissues and venous and arterial endothelial cells [9]. So, multiple organ failure can be attributable to the combination of direct viral damage with indirect pathogenic mechanisms. The latter includes immune system dysfunction, thrombo-inflammation, and the renin-angiotensin system dysregulation [10].
This work aimed to report the most frequent extra pulmonary presentations of COVID-19 in comparison to patients with primary pulmonary presentation regards patients’ characteristics and resource utility usage as reflected by the level of care required for the management. Risk factors for ICU admission in both groups were examined.
Methodology
Study design and participants
This prospective comparative cross-sectional study was conducted at Sohag University Hospital from December 2020 to August 2021.
Sampling
All adult patients (age ≥ 18 years) presented to our hospital during the study and proved positive for COVID-19 were included; other diagnosis than COVID-19 as a primary cause of presentation of the patient was excluded. Patients with mixed presentation were excluded from our analysis.
Accordingly, 716 cases with primary pulmonary presentation of COVID-19 and 948 cases with primary extrapulmonary presentation of COVID-19 were included in this study. Type of presentation either pulmonary or extrapulmonary was determined according to the patient reported main complaints and primary physician-based-evaluation of the patient at the emergency department.
Data collection
All included patients were subjected to the following: detailed demographic and clinical assessment and computed tomography (CT) scan of the chest.
The COVID-19 reporting and data system (CO-RADS) was used in the assessment of pulmonary affection of COVID-19 on non-contrast chest CT that categorized the probability of diagnosis from very low (CO-RADS category 1) to very high (CO-RADS category 5) [11].
CT severity score (CT-SS) was used to identify the severity of COVID-19.
Anatomically based 20 regions representing the 18 segments of both lungs are evaluated. The sum of the score in the 20 regions defines the total CT-SS which range from 0 to 40 points [12].
All patients diagnosed with COVID-19 based on the positive results of quantitative rRT-PCR testing of combined nasopharyngeal and oropharyngeal swabs.
Confirmed SARS-CoV-2 infected patients were categorized according to severity of illness into mild, moderate, severe, and critical illness according to the Centers of Disease Control (CDC) guidance [13].
Statistical analysis
STATA version 14.2 (Stata Statistical Software: Release 14.2 College Station, TX: StataCorp LP.) was used to analyze the data. Quantitative data was presented as mean, standard deviation. Mann–Whitney test was used to compare two groups, and Kruskal–Wallis test was used for comparison of three or more groups because the data was not normally distributed. Qualitative data was represented as number and percentage, and Chi square test was utilized for comparison. Logistic regression analysis was used to obtain Odds ratio. Excel was used to produce graphs. P value was considered significant when it was less than 0.05.
Results
This study included a total of 1664 confirmed COVID-19 patients. They were divided into 2 groups. A total of 716 patients (339 male, 377 female) presented with pulmonary manifestation of COVID-19, and 948 patients (517 male, 431 female) presented with extrapulmonary manifestation of COVID-19. The mean age of the pulmonary group was 56.20 ± 19.57, while the extrapulmonary group were significantly older with mean age 61.46 ± 16.49. Residence in rural areas was more common in the extrapulmonary group than the pulmonary group. There was statistically significant difference between the two groups as regard age, gender, and residence (P = 0.0001, 0.004, and 0.001, respectively). In both groups, about one-third of cases had chronic diseases. The prevalence of certain diseases was higher in the extra pulmonary group as cardiac, central nervous system (CNS), hepatic, and renal diseases, while chronic respiratory disorders were more prevalent in the pulmonary group (P value: < 0.0001); In regard to the level of care required for patient management, most cases in both groups required hospital admission either inward or in ICU. ICU admission was slightly higher in the pulmonary group (Table 1).
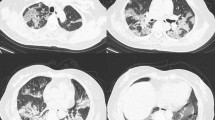
In terms of clinical and radiology evaluation, clinical case and CT severity, and complications. It was found that fever was more common in the pulmonary group. Clinical and radiological evaluation of patients in the extrapulmonary group revealed abnormalities in the oxygen saturation and CT chest despite the absence of overt respiratory manifestation as reported by the patient. The mean level of O2 saturation was significantly lower in the pulmonary group with more severe and critical ill cases in this group (P value 0.0001, < 0.0001 respectively). The mean value of CT severity was about 22.32 ± 10.21 in both groups with no significant statistical difference between both groups. CORAD 5 score was in favor of pulmonary presentation (P value: < 0.0001) (Table 2).
As regard the culprit of extrapulmonary system affection, Fig. 1 shows that central nervous system (CNS) affection was found in 236 patients (24.89%) in the extra-pulmonary group. This was in the form of cerebrovascular stroke and encephalitis with or without convulsions. Renal affection was the diagnosis in 185 patients (19.51%) of cases with 100 patients (54.05%) of them required renal replacement therapy. Other system affection in the form of (GIT, vascular, hematology, dermatology) was found in (30.59%) of the extrapulmonary group.

Type of extrapulmonary system affection of COVID-19
The multivariate analysis for risk factors of ICU admission in the pulmonary group revealed that CT severity, mean oxygen saturation, severe and critical ill disease and the presence of chronic co-morbidities are significant risk factors for ICU admission. These results preserved its statistical significance with adjusted odds ratio except for severe disease (Table 3). In the extrapulmonary group, factors that proved significance for ICU admission were CT severity, mean oxygen saturation, critical ill disease, the presence of concomitant pulmonary manifestation, and type of extrapulmonary system affection (P < 0.0001) (Table 4).
Discussion
Extrapulmonary presentation of COVID-19 is less studied than the pulmonary affection. It can be the sole manifestation or present concomitantly with the pulmonary disease [14]. This can delay proper diagnosis and management.
This study objective was to spotlight the extrapulmonary presentation of COVID-19 with hand to hand comparison to the pulmonary one and to identify risk factors for ICU admission in both situations.
Among 1664 patients that were included in our study, 716 patients (43.03%) presented with pulmonary manifestation of COVID-19, while 948 patients (57.97%) presented with extrapulmonary manifestations of COVID-19.
In this study, female gender dominates the pulmonary presentation group which was not the case in the extrapulmonary group. Patients with extrapulmonary presentation were significantly older. This is in agreement with a cross sectional study which reported that the most common age group affected in patients with pulmonary manifestations was between 40 and 60 years, while patients with extrapulmonary presentation of COVID were mostly older than 60 years [15]. Elderly patients have reduced cell-mediated and humeral immune response which increases their vulnerability to infection [16].
Almost one-third of patients in both groups had chronic comorbid conditions. It has been known that the existence of comorbidities rises up the chance of COVID-19 infection [17]. Having comorbid disease proved significance in our analysis as risk factor for ICU admission in the pulmonary group. In concordance with that, evidence in the literature identified increased rate of ICU admission in COVID patients with underlying comorbidities [18].
Patients with pulmonary manifestations commonly presented with fever and cough [19]. In our work, fever was found in more than half patients in each group. The mean level of O2 saturation was significantly lower in patients with pulmonary presentation than those with extrapulmonary presentation. In addition, higher percentages of severe and critically ill cases were recorded in the pulmonary presentation group. Demographics of this group showed increased prevalence of underlying chronic respiratory diseases which may explain this progressive course of the disease in the pulmonary group.
CT examination is valuable for the diagnosis and the follow-up of disease progression [20]. A study reported that CT imaging in the pulmonary and extrapulmonary presentation COVID-19 patients showed significant difference [21]; however, in our work, CT evaluation in the extrapulmonary group revealed positive finding with no significant difference in CT severity score compared to the pulmonary group. CORAD 5 was predominant in the pulmonary group.
The CNS affection was the most common extrapulmonary system involved in our work. A common CNS manifestation in our study was cerebrovascular stroke (CVS). This finding is supported by evidence in literature. In the research done by Majidi et al., 42% of patients presented with ischemic stroke without overt respiratory manifestation. COVID-19 symptoms appeared later on. Risk of thrombosis appeared to increase early in the disease journey which may explain such presentation [22].
Acute kidney injury (AKI) is a salient renal manifestation of corona virus disease.In our study, renal affection ranked second most common in the extrapulmonary group. Critically ill patients in particular are vulnerable to renal dysfunction [23]. Postulation for this affection was that the expression (ACE2) receptor leads to a direct impact of SARS-CoV-2 on the kidney [24, 25]. The cytokine storm also can be hazardous to renal function that may precipitate acute renal dysfunction and failure [26].
Cardiac affection was encountered in (12.76%) of cases in the extrapulmonary group in this study. Acute coronary syndrome, myocarditis, arrhythmias, and venous thrombo-embolic disorders have been described. Location of ACE2 receptors in the cardiac tissue leads to virus induced tissue degeneration and injury [27]. Hypoxia and hypercoagulable status are additional detrimental factors to the cardiac function. Reports of cardiac manifestation of COVID-19 are prevalent in the literature [28, 29].
More cases in the extrapulmonary group required ward and ICU admission.
Severe and critical cases of COVID mostly necessitate ICU admission and management. Mortality rate is estimated between 3.4% and 11% [30]. Thereby, recognition of risk factors of disease progression is very helpful. This study identified the risk factors for ICU admission in COVID-19 patients.
In the pulmonary presentation group, risk factors for ICU admission were critically ill category of patients, CT severity, oxygen saturation level, and the presence of comorbid chronic disease. In line with these results, CT severity score proved helpful on identifying severe disease [31]. Also, preexisting chronic diseases were recognized as hazardous for a more serious course of COVID as reported by published studies [32].
Risk factors for ICU admission in extrapulmonary presentations group of our work were almost similar to those in the pulmonary group. Cardiac, metabolic, and renal affection in particular proved significant risk for ICU admission.
Conclusion
We admit that cases of COVID are decreasing in number globally. Yet, the recent WHO warning about possibilities of future epidemic is an alarming sign. It might be too early to forget about COVID lessons. Atypical or non-respiratory manifestation could be the presentation of respiratory pathogen. Our work highlights the extrapulmonary presentation of COVID-19. Older male patients were more prone to present with extra pulmonary symptoms. CNS, cardiac, renal, and metabolic dysfunctions were the most commonly affected systems. All proved significant factors for ICU admission.
Though this study is single center, it includes a relatively large number size over two sequential waves of COVID-19 pandemic. This ensures that the results provide additional evidence to the literature.
Availability of data and materials
The datasets utilized or analyzed in this study can be obtained from the corresponding author on reasonable requests.
Abbreviations
- ACE 2:
-
Angiotensin-converting enzyme 2
- AKI:
-
Acute kidney injury
- ARDS:
-
Acute respiratory distress syndrome
- ICU:
-
Intensive care unit
- CDC:
-
Centers for Disease control and Prevention
- CNS:
-
Central nervous system
- CORAD:
-
COVID-19 reporting and data system
- COVID-19:
-
Corona virus 19
- CT:
-
Computed tomography
- CT-SS:
-
CT severity score
- CVS:
-
Cerebrovascular stroke
- SARS-CoV-2:
-
Severe acute respiratory syndrome-Corona virus-2
- rRT-PCR:
-
Recombinant reverse transcriptase-polymerase chain reaction
References
Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y et al (2020) Clinical features of patients infected with 2019 novel coronavirus in Wuhan China. Lancet 395:497–506
Chen N, Zhou M, Dong X, Qu J, Gong F, Han Y et al (2020) Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet 395:507–513
Rodriguez-Morales AJ, Cardona-Ospina JA, Gutierrez-Ocampo E, Villamizar-Pena R, Holguin-Rivera Y, Escalera-Antezana JP et al (2020) Clinical, laboratory and imaging features of COVID-19: a systematic review and meta-analysis. Travel Med Infect Dis 34:101623
Gómez-Belda AB, Fernández-Garcés M, Mateo-Sanchis E, Madrazo M, Carmona M, Piles-Roger L et al (2021) COVID-19 in older adults: what are the differences with younger patients? Geriatr Gerontol Int 21:60–65
Izzedine H, Jhaveri KD (2021) Acute kidney in patients with COVID-19: an update on the pathophysiology. Nephrol Dial Transplant 36(2):224–226
Mao R, Qiu Y, He JS, Tan JY, Li XH, Liang J et al (2020) Manifestations and prognosis of gastrointestinal and liver involvement in patients with COVID-19: a systematic review and meta-analysis. Lancet Gastroenterol Hepatol 5:667–678
Bavaro DF, Poliseno M, Scardapane A, Belati A, De Gennaro N, Stabile Ianota AA et al (2020) Occurrence of acute pulmonary embolism in COVID-19 — a case series. Int J Infect Dis 98:225–226
Azizi SA, Azizi SA (2020) Neurological injuries in COVID-19 patients: direct viral invasion or a bystander injury after infection of epithelial/endothelial cells. J Neurovirol 26:631–641
Miri SM, Roozbeh F, Omranirad A, Alavian SM (2020) Panic of buying toilet papers: a historical memory or a horrible truth? Systematic review of gastrointestinal manifestations of COVID-19. Hepat Mon 20(3):102729
Jin X, Lian JS, Hu JH, Gao J, Zheng L, Zhang YM et al (2020) Epidemiological, clinical and virological characteristics of 74 cases of coronavirus-infected disease 2019 (COVID-19) with gastrointestinal symptoms. Gut 69(6):1002–1009
An JY, Unsdorfer KML, Weinreb JC (2019) BI-RADS, C-RADS, CAD-RADS, LI-RADS, Lung-RADS, NI-RADS, O-RADS, PI-RADS, TI-RADS: reporting and data systems. Radiographics 39(5):1435–1436
Chang YC, Yu CJ, Chang SC et al (2005) Pulmonary sequelae in convalescent patients after severe acute respiratory syndrome: evaluation with thin-section CT. Radiology 236(3):1067–1075
Centers for Disease Control and Prevention (2020) COVID-19 (coronavirus disease): people with certain medical conditions. Available at: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/people-withmedical-conditions.html. Accessed 7 Dec 2020
AlSamman M, Caggiula A, Ganguli S, Misak M, Pourmand A (2020) Non respiratory presentations of COVID 19, a clinical review. Am J Emerg Med 38(2444):54
Nivea B, Kamath V, Markanday K, Jacob MJ, Mohan D (2021) A cross-sectional study of pulmonary and extrapulmonary manifestations of COVID-19. APIK J Int Med 9:250–255
Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z et al (2020) Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet 395(10229):1054–1062. https://doi.org/10.1016/S0140-6736(20)30566-3. (Epub 2020 Mar 11)
CDC (2020) Coronavirus (COVID-19): symptoms of coronavirus. Centers for Disease Control and Prevention. [Accessed April 18, 2020, https://www.cdc.gov/coronavirus/2019-ncov/symptoms-testing/symptoms.html]
Sanyaolu A, Okorie C, Marinkovic A, Patidar R, Younis K, Desai P, Hosein Z, Padda I, Mangat J, Altaf M (2020) Comorbidity and its impact on patients with COVID-19. SN Compr Clin Med 2(8):1069–1076. https://doi.org/10.1007/s42399-020-00363-4. Epub 2020 Jun 25. PMID: 32838147; PMCID: PMC7314621
Varghese GM, John R, Manesh A, Karthik R, Abraham OC (2020) Clinical management of COVID-19. Indian J Med Res 151:401–410
Metlay JP, Waterer GW, Long AC et al (2019) Diagnosis and treatment of adults with community-acquired pneumonia: an official clinical practice guideline of the American Thoracic Society and Infectious Disease Society of America. Am J Respir Crit Care Med 200:e45–67
Yang Z, Chen X, Huang R, Li S, Lin D, Yang Z et al (2021) Atypical presentations of coronavirus disease 2019 (COVID-19) from onset to readmission. BMC Infect Dis 21:127
Majidi S, Fifi JT, Ladner TR, Lara-Reyna J, Yaeger KA, Yim B et al (2020) Emergent large vessel occlusion stroke during New York City’s COVID-19 outbreak: Clinical characteristics and paraclinical findings. Stroke 51:2656–2663
Zheng KI et al (2021) Extrapulmonary Complications of COVID-19: a Multisystem Disease? J Med Virol 93:323–335. https://doi.org/10.1002/jmv.26294
Hamming I, TimensW, BulthuisMLC, Lely AT, Navis G, van Goor H (2004) Tissue distribution of ACE2 protein, the functional receptor for SARS coronavirus. A first step in understanding SARS pathogenesis. J Pathol 203: 631–7. https://doi.org/10.1002/path.1570
Angel-Korman A, Brosh T, Glick K, Leiba A (2020) COVID-19, the kidney and hypertension. Harefuah 159:231–234
Naicker S, Yang CW, Hwang SJ, Liu BC, Chen JH, Jha V (2020) The novel coronavirus 2019 epidemic and kidneys. Kidney Int 97:824–828. https://doi.org/10.1016/j.kint.2020.03.001
Nishiga M, Wang DW, Han Y, Lewis DB, Wu JC (2020) COVID-19 and cardiovascular disease: From basic mechanisms to clinical perspectives. Nat Rev Cardiol 17:543–558
Shi S, Qin M, Shen B, Cai Y, Liu T, Yang F et al (2020) Association of cardiac injury with mortality in hospitalized patients with COVID-19 in Wuhan. China JAMA Cardiol 5:802–810
Zheng YY, Ma YT, Zhang JY, Xie X (2020) COVID-19 and the cardiovascular system. Nat Rev Cardiol 17:259–260. https://doi.org/10.1038/s41569-020-0360-5
Rajgor DD, Lee MH, Archuleta S et al (2020) The many estimates of the COVID-19 case fatality rate. Lancet Infect Dis 20(7):776–777
Zayed NE, Bessar MA, Lutfy S (2021) CO-RADS versus CT-SS scores in predicting sever COVID-19 patients:retrospective comparative study. Egypy J Bronchol 15:13
Wolff D, Nee S, Hickey NS et al (2020) Risk factors for Covid-19 severity and fatality: a structured literature review. Infection 28:1–14
Acknowledgements
Not applicable.
Funding
The researchers declare that they have not received any funding for publishing the manuscript.
Author information
Authors and Affiliations
Contributions
HE, AK, HS.M, HM, and DG all share in conception, design of the work, acquisition, analysis, and interpretation of data. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval was obtained from the Medical Research Ethics Committee of Faculty of Medicine-Sohag University, IRB No. Soh-Med- 21–04-25, and registered on ClinicalTrials.gov ID: NCT04896762. The study was conducted in compliance with the principles of the 1964 Declaration of Helsinki and its 2013 amendment. Written informed consent was got from all participant patients.
Consent for publication
Informed consent was obtained from the patient participating in our study.
Competing interests
There are no conflicts of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Esmaeel, H.M., Mohamed, H.S., Khalaf, A.R. et al. Extra pulmonary versus pulmonary presentation of COVID-19 patients: comparative study. Egypt J Bronchol 17, 67 (2023). https://doi.org/10.1186/s43168-023-00241-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43168-023-00241-2