
Abstract
Background
Regarding risk stratification of intermediate-risk pulmonary embolism, data are still not sufficient. Transthoracic echocardiography parameters may be useful in risk evaluation in those patients. Some novel echocardiographic indices mainly tricuspid regurgitation peak gradient (TRPG), pulmonary artery acceleration time, and tricuspid annulus plane systolic excursion (TAPSE) were evaluated showing that they may be used for risk stratification of normotensive cases with acute pulmonary embolism (APE).
Results
The studied cases were subdivided into two classes:
Class I with intermediate-low-risk pulmonary embolism included 32 patients (53.3%) and class II with intermediate high-risk pulmonary embolism involved 28 cases (46.7%). Dyspnea, tachypnea, troponin level, RVD, RVD/LVD, TR velocity, and TRPG/TAPSE were statistically higher in cases of class II than that of class I (p < 0.001). On the other hand, TAPSE and PA acceleration time were markedly lower in the case of class II than that of class I (p < 0.001). Ten cases (35.7%) of group II required thrombolytic agents with a significant difference (p<0.001).
Conclusions
RVD/LVD ratio, TAPSE, TRPG/TAPSE ratio, and PA acceleration time are echocardiographic parameters that might be helpful for risk stratification of cases with moderate-risk pulmonary embolism. The addition of elevated levels of cardiac troponins to imaging and clinical findings can improve PE-related risk identification.
Trial registration
NCT04020250. Registered on 16 July 2019.
Similar content being viewed by others

Explore related subjects
Find the latest articles, discoveries, and news in related topics.Background
A major health issue with a high death rate is pulmonary embolism (PE) [1]. PE has a significant rate of misdiagnosis because of its non-specific clinical symptoms and lack of a particular physical finding [2, 3]. Recently, clinicians utilized a variety of diagnostic procedures, including blood gas analysis, computed tomographic pulmonary angiography(CTPA), lower limb proximal deep vein compression ultrasound, and plasma D-dimer assays [4, 5].
Clinical classification of acute pulmonary embolism severity is depending on the evaluated 30-day death risk. Cases with shock resulting from acute pulmonary embolism consider a high-risk class for early mortality that is account more than 15% [6], while the intermediate-risk group constitutes a very heterogeneous class in which the early death rates are between 2 and 15%.
Most patients remain hemodynamically stable during taking anticoagulants, clinical deterioration is possible, and patients may require emergency thrombolysis or a surgical or percutaneous embolectomy if this happens [6].
RV dysfunction can be determined by using the bedside diagnostic method of echocardiography. The risk stratification of cases with normotensive APE can be done by using the tricuspid annulus plane systolic excursion (TAPSE) [7]. APE risk stratification may be aided by the tricuspid regurgitation peak gradient (TRPG), an echocardiographic marker of RV overload [8].
Aim of the study
The study aims:
-
1.
To assess the accuracy and prognostic significance of TRPG, TAPSE, and pulmonary artery acceleration time in risk stratification of cases with moderate risk pulmonary embolism
-
2.
To provide cut-off measurements for these parameters
-
3.
To determine the requirement for rescue thrombolysis in primary normotensive APE cases with rabid clinical deterioration
Patients and methods
This prospective cross-sectional study was performed at Chest Department, Assiut University Hospital, from August 2019 to May 2021, after approval by the Scientific Ethics Commission of the Faculty of Medicine of Assiut University (IRB no 17100850, dated 1/12/2019). Clinical trial number: NCT04020250
Sixty patients with acute pulmonary embolism (24 males and 36 females) were recorded in this work; computed tomographic pulmonary angiography (CTPA) was used to diagnose PE.
Inclusion criteria
Cases with moderate-risk pulmonary embolism that were:
-
a)
Age ≥ 18years old.
-
b)
Systolic blood pressure ≥ 90mmHg and no symptoms of peripheral hypoperfusion at admission.
-
c)
The sPESI (simplified pulmonary embolism severity index) is more than 1.
Exclusion criteria
Patients <18 years old.
Cases having valvular heart diseases.
Cases having acute massive pulmonary embolism who presented with hemodynamic instability.
Written informed approval was taken from whole involved cases in this study.
Whole cases were submitted to full medical history and clinical examination. Arterial blood gases, complete blood count, serum troponin levels, D-dimer, and renal and liver function tests were done for all enrolled patients. Each subject underwent detailed transthoracic echocardiography (TTE) within the first 24 h of admission.
Transthoracic echocardiography
During the first 24 h following approval, a transthoracic echocardiographic assessment was carried out using a Philips HD5 device (Philips Medical System, USA) with 2.5–3.5 MHz transducers, and the findings were recorded. Cases were evaluated while positioned to the left lateral position. In the parasternal short-axis imaging, the dimensions of the left and right ventricles were estimated. The simplified Bernoulli equation was used to determine the tricuspid regurgitation peak gradient (TRPG) on the tricuspid valve in the apical 4-chamber view by continuous wave Doppler. Pulsed wave Doppler was used to quantify the pulmonary ejection acceleration time (AT), with the sample volume put in the RV outflow tract immediately under the pulmonary valve in short parasternal view (aortic valve level). A value of pulmonary artery acceleration time less than 130 msec is considered abnormal. measurement were averaged over 3 consecutive heart cycles. RV performance was evaluated by measuring tricuspid annulus plane systolic excursion (TAPSE) using M mode. We have measured the distance (mm) of the systolic excursion of the lateral tricuspid valve annulus towards the apex in the apical 4-chamber view. A value of TAPSE less than 16 mm is considered abnormal. The parameter of TRPG/TAPSE was computed. Simpson’s formula was used to determine the left ventricular ejection fraction (LVEF) utilizing a 2D picture of the LV chamber in the 2- and 4-chamber apical views during systole and diastole.
Statistical analysis
Data of this study was gathered and examined utilizing SPSS (Statistical Package for the Social Science, version 20, IBM, and Armonk, New York). Continuous information was explained in shape of mean ± standard deviation or median while nominal information was explained in shape of frequent rate.
Groups were in comparison utilizing an ANOVA or Mann-Whitney U-test where data were ordinal, and χ2 test of independence or Fisher’s exact test for normal information. A p-value of <0.05 was considered statistically significant
Results
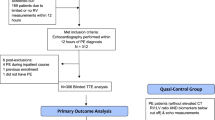
This study enrolled 60 cases (24 men and 36 women) with moderate-risk PE that are normotensive with simplified pulmonary embolism severity index (sPESI > 1). They were categorized into 2 classes, class I (32, 53.3%) (intermediate-low-risk PE) characterized by sPESI > 1 with either right ventricular (RV) dysfunction or positive troponin test or both are negative, and class II (28, 46.7%) (intermediate-high-risk PE) characterized by sPESI > 1 with concomitant RV dysfunction and positive troponin test.
Demographic data, risk factors, and comorbidities of the recorded cases are displayed in Table 1. The most frequent symptom was dyspnea which was reported in all patients with PE; chest pain was the second complaint with no statistical difference between both groups. Tachycardia was reported in all patients and tachypnea with respiratory rate > 30 was reported in all patients in group II.
Group II patients all had positive troponin, while only 11 (34.4%) patients of group I had positive troponin with a statistically significant difference (p< 0.001) between both classes (Table 2).
Echocardiographic parameters of studied patients are presented in Table 3. In group II patients, RVD, RVD/LVD ratio, TR velocity, and TRPG/TAPSE were significantly higher than those of group I, while TAPSE and acceleration time were markedly lower in group II. The most frequent anticoagulants used in those patients were parenteral anticoagulants in form of LMWH and warfarin or UFH for 24–48 h followed by warfarin. Ten cases have intermediate-high-risk PE that required thrombolytic therapy (p<0.001), while embolectomy was done in only one patient of group II (Table 4).
It was found that patients with positive troponin had significantly lower TAPSE and acceleration time and significantly higher TRPG/TAPSE (p< 0.001) in comparison to those with negative troponin (Table 5).
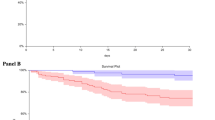
Table 6 shows the diagnostic accuracy of echocardiographic indices measured in predicting intermediate-high-risk PE. It was found that TAPSE at cutoff point < 1.70 cm had 100% sensitivity and 100% specificity for prediction of intermediate-high-risk APE with 100% accuracy and the area under the curve was 1.
TRPG/TAPSE ratio at cutoff point > 0.96 had 79% sensitivity and 94% specificity for prediction of intermediate-high-risk APE with 86.9% accuracy and area under the curve was 0.89. Acceleration time at cutoff point < 130 (msec) had 100% sensitivity and 87% specificity for the prediction of intermediate-high-risk APE with 93.1% accuracy and the area under the curve was 0.95 (Fig. 1).

Accuracy of new parameters in prediction of intermediate-high-risk PE
Discussion
This prospective cross-sectional study included 60 patients with intermediate-risk PE. The studied cases were classified into two classes:
Class I (intermediatelow-risk PE) and class II (intermediatehigh-risk PE). Most of our patients were females. De Miguel-Diez et al. observed variations in the occurrence and death from pulmonary embolism considering age and sex [9, 10]. Also, women had a significantly higher occurrence of PE and death than men, despite men having an elevated certain risk factor prevalence, like cancer and cigarette smoking. On the other side, Yang et al. in their study documented that the occurrence of PE was elevated in male cases [10]. Heit et al. documented a similar occurrence in both males and females [11], while Silverstein et al. reported a higher age-adjusted occurrence among men than women [12].
Dyspnea was the main complaint in all patients followed by chest pain. Similarly, in previous studies, dyspnea and chest pain were the most prevalent symptoms, also, tachycardia and tachypnea were the most common signs [13,14,15].
Both groups of patients had non-significant differences as regards baseline arterial blood gases and laboratory data (p> 0.05) with exception of significantly higher positive troponin among patients of class II in comparison to class I ( p <(0.001). Cardiac troponin level can recognize cases with an increased risk of mortality and sequelae through the acute stage of PE. In this regard, it was noted that circulating troponin T levels can enhance the risk stratification of normotensive cases with acute PE, and especially, identify cases who are at low risk of an early adverse outcome [16]. In contrast to those of the simplified PESI, a high sensitivity and negative predictive value were associated with a troponin level. They were recognized as independent predictors of 30-day complicated outcomes [17, 18]. By contrast, none of the cases with low-risk stratifications and low levels of troponin experienced reverse results, but the cases with low-risk simplified PESI and increased troponin had a higher rate of reverse results [18].
As regards the management of PE, echocardiography saves rapid and accurate risk assessment and helps the physician to choose the type of therapy [19]. In normotensive PE patients, right ventricular impairment on echocardiography provide prognostic data which is distinct from clinical results concise by the PE severity index (PESI) [20].
In this study, there were significant differences in echocardiographic parameters between the two groups. Patients in group II had higher RVD, RVD/LVD ratio, TR velocity, and TRPG/TAPSE ratio than those with group I patients. On the other hand, significantly lower TAPSE and acceleration time were found in group II in comparison to those with group I. Three studies reported an elevated risk of mortality in cases with high RVD [21, 22]. These studies were carried out on cases with different grades of clinical severity and did not involve only cases with intermediate PE. Moreover, they added that RVD could be demonstrated not only by acute PE but by cardiopulmonary comorbidities as well [23]. There was significantly lower TPASE and acceleration time in the high-risk group in comparison to those with low risk. Similarly, it was reported that echocardiographic parameters were utilized to apply the early risk of cases with PE. RVD/LVD diameter rate ≥1.0 and a TAPSE <16 mm are the results associated with unfavorable prognosis [24]. Totally, evidence for RV impairment on echocardiography is present in ≥25% of unselected cases with acute PE [6]. Meta-analyses and systematic reviews show that RV impairment on echocardiography is related to an increased short-term death risk in cases who appear hemodynamically stable at presentation [25]; however, a meta-analysis found that its overall positive predictive value for PE-related death was low (<10%) [22, 25].
Ciurzyński et al. stated that TAPSE and RV/LV ratio are useful to predict outcomes in non-elevated risk APE cases. Ciurzyński et al. set the cut-off point of TAPSE as >20 mm and this gives 100% NPV for the CE. Therefore, cases with TAPSE >20 mm represent a least-risk class with a good prognosis [26]. They also consider TRPG/TAPSE parameter as a second echocardiographic move for risk stratification. ROC analysis showed markedly higher AUC for TRPG/TAPSE than for RV/LV and TRPG alone in cases with TAPSE ≤20 mm.
It was noticed that TAPSE <17 mm is highly predictive of RV systolic dysfunction [27]. Ciurzyński et al. notified that TAPSE is a valuable parameter for risk stratification in normotensive APE cases, and TAPSE >20 mm can be utilized for the identification of low-risk cases [28]. It was tried to risk-stratify normotensive APE cases utilizing a stepwise echocardiographic program. As the initial step, TAPSE measurement was proposed. In most cases of intermediate-risk PE, the CE was noticed in cases with TAPSE ≤20 mm. Subsequently, TRPG/TAPSE was a recent echo parameter to differentiate these patients.
The preferred technique for noninvasively measuring pulmonary artery pressure at the systolic level is dependent on persistent wave Doppler assessment of TRPG. In APE cases without RV overload, a normal TRPG and an increased TAPSE and significantly lower TRPG/TAPSE were observed. The present study showed that TAPSE at a cutoff point < 17.0 mm had 100% sensitivity and 100% specificity for the prediction of high-intermediate-risk APE with 100% accuracy and the area under the curve was 1.
There were some limitations to this current study. The sample size in this study was relatively small so a large, prospective study is required to validate the observations reported. This current study was conducted in one center in Assiut University Hospital, Faculty of Medicine; further multi-centered study should be done.
Conclusions
Echocardiography is a convenient and noninvasive imaging technique that may provide important information about the right ventricular function.
RVD/LVD ratio, TAPSE, TRPG/TAPSE ratio, and PA acceleration time are echocardiographic parameters that may be useful in risk stratification of normotensive cases with APE, and they identify cases with a bad prognosis.
Increased levels of cardiac troponins have a relatively good impact in normotensive cases with acute PE; when interpreted in combination with imaging and clinical results, they can improve the identification of PE-linked risk and the further prognostic stratification of such cases.
Availability of data and materials
The corresponding author will provide the data sets utilized and/or assessed during the present study upon reasonable request.
Abbreviations
- APE:
-
Acute pulmonary embolism
- LVEF:
-
Left ventricular ejection fraction
- LVD:
-
Left ventricular diameter
- PE:
-
Pulmonary embolism
- PA:
-
Pulmonary artery
- RVD:
-
Right ventricle diameter
- PESI:
-
Pulmonary embolism severity index
- TAPSE:
-
Tricuspid annulus plane systolic excursion
- SPESI:
-
Simplified pulmonary embolism severity index
- TTE:
-
Transthoracic echocardiography
- TRPG:
-
Tricuspid regurgitation peak gradient
References
Molaee S, Ghanaati H, Safavi E, Foroumandi M, Peiman S (2015) Computed tomography pulmonary angiography for evaluation of patients with suspected pulmonary embolism: use or overuse. Iran J Radiol. 12(3):1–3
Benjamin E, Virani S, Callaway C, Chamberlain A, Chang A (2018) Cheng S et alHeart disease and stroke statistics - 2018 update: A report from the American Heart Association. Circulation. 137:67–492
Paparoupa M, Spineli L, Framke T, Ho H, Schuppert F, Gillissen A (2016) Pulmonary Embolism in Pneumonia: Still a Diagnostic Challenge? Results of a Case-Control Study in 100 Patients. Dis Markers. 2016:8682506. https://doi.org/10.1155/2016/8682506
Robert-Ebadi H, Glauser F, Planquette B, Moumneh T, Le Gal G, Righini M (2017) Safety of multidetector computed tomography pulmonary angiography to exclude pulmonary embolism in patients with a likely pretest clinical probability. J Thromb Haemost. 15(8):1584–1590
Lei M, Liu C, Luo Z, Xu Z, Jiang Y, Lin J et al (2021) Diagnostic management of inpatients with a positive D-dimer test: developing a new clinical decision-making rule for pulmonary embolism. Pulm Circ. 11(1):2045894020943378
Konstantinides SV, Meyer G, Bueno H, Galié N, Gibbs JSR, Ageno W et al (2020) 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European respiratory society (ERS). Eur Heart J. 41(4):543–603
Jurcut R, Giusca S, La Gerche A, Vasile S, Ginghina C, Voigt JU (2010) The echocardiographic assessment of the right ventricle: What to do in 2010? Eur J Echocardiogr. 11(2):81–96
Jaff MR, McMurtry MS, Archer SL, Cushman M, Goldenberg N, Goldhaber SZ et al (2011) Management of massive and submassive pulmonary embolism, iliofemoral deep vein thrombosis, and chronic thromboembolic pulmonary hypertension: a scientific statement from the american heart association. Circulation. 123(16):1788–1830
De Miguel-Diez J, Jiménez-Garcia R, Jiménez D, Monreal M, Guijarro R, Otero R et al (2014) Trends in hospital admissions for pulmonary embolism in Spain from 2002 to 2011. Eur Respir J. 44(4):942–950
Yang Y, Liang L, Zhai Z, He H, Xie W, Peng X et al (2011) Pulmonary Embolism Incidence and Fatality Trends in Chinese Hospitals from 1997 to 2008: A Multicenter Registration Study. PLoS ONE 6(11):e26861. https://doi.org/10.1371/journal.pone.0026861
Heit JA, Silverstein MD, Mohr DN, Petterson TM, O’Fallon WM, Melton LJ (2002) Risk factors for deep vein thrombosis and pulmonary embolism: a population-based case-control study. Arch Intern Med. 160(6):809–815
Silverstein MD, Heit JA, Mohr DN, Petterson TM, O’Fallon WM, Melton LJ (1998) Trends in the incidence of deep vein thrombosis and pulmonary embolism: a 25-year population-based study. Arch Intern Med. 158(6):585–593
Turan O, Turgut D, Gunay T, Yilmaz E, Turan A, Akkoclu A (2017) The contribution of clinical assessments to the diagnostic algorithm of pulmonary embolism. Adv Clin Exp Med. 26(2):303–309
Worsley DF, Alavi A (1995) Comprehensive analysis of the results of the PIOPED Study. Prospective Investigation of Pulmonary Embolism Diagnosis Study. J Nucl Med [Internet]. 36(12):2380–2387 Available from: http://www.ncbi.nlm.nih.gov/pubmed/8523135
Wicki J, Perneger TV, Junod AF, Bounameaux H, Perrier A (2001) Assessing clinical probability of pulmonary embolism in the emergency ward: a simple score. Arch Intern Med. 161(1):92–97
Lankeit M, Jiménez D, Kostrubiec M, Dellas C, Hasenfuss G, Pruszczyk P et al (2011) Predictive value of the high-sensitivity troponin T assay and the simplified pulmonary embolism severity index in hemodynamically stable patients with acute pulmonary embolism: a prospective validation study. Circulation. 124(24):2716–2724
Moores L, Aujesky D, Jiménez D, Díaz G, GóMez V, Martí D et al (2010) Pulmonary Embolism Severity Index and troponin testing for the selection of low-risk patients with acute symptomatic pulmonary embolism. J Thromb Haemost. 8(3):517–522
Jiménez D, Aujesky D, Moores L, Gómez V, Lobo JL, Uresandi F et al (2010) Simplification of the pulmonary embolism severity index for prognostication in patients with acute symptomatic pulmonary embolism. Arch Intern Med. 170(15):1383–1389
Goldhaber SZ (2002) Echocardiography in the management of pulmonary embolism. Ann Intern Med. 136(9):691–700
Sanchez O, Trinquart L, Planquette B, Couturaud F, Verschuren F, Caille V et al (2013) Echocardiography and pulmonary embolism severity index have independent prognostic roles in pulmonary embolism. Eur Respir J. 42(3):681–688
Jiménez D, Lobo JL, Monreal M, Otero R, Yusen RD (2012) Prognostic significance of multidetector computed tomography in normotensive patients with pulmonary embolism: rationale, methodology and reproducibility for the PROTECT study. J Thromb Thrombolysis. 34(2):187–192
Sanchez O, Trinquart L, Colombet I, Durieux P, Huisman MV, Chatellier G, Meyer G (2008) Prognostic value of right ventricular dysfunction in patients with haemodynamically stable pulmonary embolism: a systematic review. Eur Heart J. 29(12):1569–77. https://doi.org/10.1093/eurheartj/ehn208
Klok FA, Mos ICM, Huisman MV (2008) Brain-type natriuretic peptide levels in the prediction of adverse outcome in patients with pulmonary embolism: a systematic review and meta-analysis. Am J Respir Crit Care Med. 178(4):425–430
Schoepf UJ, Kucher N, Kipfmueller F, Quiroz R, Costello P, Goldhaber SZ (2004) Right ventricular enlargement on chest computed tomography: a predictor of early death in acute pulmonary embolism. Circulation. 110(20):3276–3280
Coutance G, Cauderlier E, Ehtisham J, Hamon M, Hamon M (2011) The prognostic value of markers of right ventricular dysfunction in pulmonary embolism: a meta-analysis. Crit Care. 15(2):R103. https://doi.org/10.1186/cc10119
Ciurzyński M, Kurnicka K, Lichodziejewska B, Kozłowska M, Pływaczewska M, Sobieraj P et al (2018) Tricuspid regurgitation peak gradient (TRPG)/tricuspid annulus plane systolic excursion (TAPSE): ― a novel parameter for stepwise echocardiographic risk stratification in normotensive patients with acute pulmonary embolism ―. Circ J. 82(4):1179–1185
Lang RM, Badano LP, Mor-Avi V, Afilalo J, Armstrong A, Ernande L et al (2015) Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr. 8:1–39. https://doi.org/10.1016/j.echo.2014.10.003
Piotr P, Sylwia G, Barbara L, Maciej K, Michał C, Katarzyna K et al (2014) Prognostic value of echocardiography in normotensive patients with acute pulmonary embolism. JACC Cardiovasc Imaging 7(6):553–560. https://doi.org/10.1016/j.jcmg.2013.11.004
Acknowledgements
The authors thank every employee in the Chest Department for their sincere efforts and careful attention to patient observation.
Funding
There was no funding.
Author information
Authors and Affiliations
Contributions
MME picked the research and helped in writing. DAH participated in the writing of the document while compiling the case’s information. The data analysis, writing, statistics, and publication are all done by RME and MNM. All authors certify that they have read, approved, and accepted the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study design was accepted by the Scientific Ethics commission of the Faculty of Medicine of Assiut University (IRB no 17100850, dated 1/12/2019).
Post-convention the inclusion criteria, informed written consent was gained from the cases pre-recording in the study. Number of clinical trial: NCT04020250
Consent for publication
Not relevant. There are no distinguishing images or any private or medical details about individuals that could threaten their privacy.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
El-Morshedy, R.M., El-kholy, M.M., Hamad, D.A. et al. Prognostic value of echocardiographic indices in risk stratification of intermediate-risk pulmonary embolism. Egypt J Bronchol 17, 6 (2023). https://doi.org/10.1186/s43168-023-00181-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43168-023-00181-x