
Abstract
Mini abstract
This work studies the direct cost of hip fractures in Egypt. The direct cost was calculated based on the incidence of hip fracture in Egypt retrieved from the national database. The result of this work raises red flags to the policy makers in Egypt that such fragility fractures are preventable, should appropriate approaches be implemented.
Background
This study provides an analysis for the healthcare system in Egypt. It was carried out to assess the direct annual cost incurred to the Egyptian healthcare system in 2023 as a result of fragility hip fractures in older adult Egyptians.
Results
The direct costs of hip fractures incurred during the first year after the injury were estimated at 1,969,385,000 Egyptian pounds (US $63,734,142.4). Time from fracture to surgery was 2.2 + 0.5 days. The average hospital stay after hip fracture surgery was 5.2 + 2.6 days. 4.5% of patients died after surgery, on average 2.3 + 0.4 months. After being discharged from the hospital, all patients needed home care.
Conclusion
Hip fractures have a significant clinical and financial impact on patients and the healthcare system. This study raises red flags for the healthcare policy makers in Egypt, as the financial burden due to the direct costs of hip fractures justifies extensive prevention programs for osteoporosis and fragility fractures. There is an urgent need to implement diagnostic approaches and validated management protocols for bone health disorders and its associated fractures in Egypt.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Background
Osteoporosis is a chronic disorder characterized by a progressive reduction in bone mass and microarchitectural deterioration which eventually cause bones to become weak and fragile, increasing the risk of fragility fractures. Such fractures have serious consequences for the individual, causing chronic pain and long-term disability. Hip fractures, in particular, are a leading cause of death and disability worldwide, particularly among the elderly. Moreover, hip fractures are associated with physical and mental impairment as well as high costs for hospitalization [1,2,3]. According to reports, there is a high risk of a subsequent fracture occurring within 1 to 2 years after an incident fragility fracture, known as an imminent fracture risk [4]. However, only a small portion of eligible women and men receive osteoporosis treatment, indicating a significant treatment gap, despite new clinical practice guidelines and interventions to lower fracture risk [5, 6].
Bone mineral density decreases progressively with age, with a faster rate of bone loss in women [7]. Consequently, older women have the highest rates of osteoporosis and hip fractures [8]. It is estimated that 53.9% of postmenopausal women in Egypt have osteopenia, and 28.4% have osteoporosis [9]. On the male side, previous data demonstrated that 26% of men over the age of 50 are osteopenic, while 21.9% have osteoporosis [9, 10]. In concordance with the changes in population demographics worldwide, Egypt is expected to face a similar challenge, as the number of older adults will significantly rise over the coming decades. In 2020, the number of older adults was 8.42 million, and this is expected to rise to 11.47 million in 2030. The number of older adults is expected to increase further by 2050, as it is anticipated to be 22.03 million. These people are at a high risk of developing osteoporotic fragility fractures and suffering the associated morbidity. Osteoporotic hip fractures affect people’s quality of life as well as place a heavy financial burden on families and the healthcare system [11]. Each year, over five million disability adjusted life years (DALYs) are caused by osteoporosis and osteopenia [12]. Over 40% of the DALYs brought on by osteoporosis are caused by fragility hip fractures [2]. These people’s mortality rates range from 8.1 to 10.5% at 30 days to 21.6–31.2% at 1 year [13, 14]. Current knowledge of the financial burden of hip fracture and cost-effectiveness assessments of the interventions under consideration are necessary for policy decisions regarding the investment in new services or interventions. When estimating the impact of hip fractures and osteoporosis, accurate data on the cost of hip fractures is a crucial factor to take into account. It is also a significant input in cost-effectiveness analyses. So far, there is limited knowledge about the economic burden of osteoporosis and fragility fractures in Egypt. The purpose of this study was to determine the annual cost of inpatient care for hip fractures in Egypt in terms of bed days and direct hospital costs.
Methods
Data source
The Egyptian Hip Fracture Database is a clinically led, extranet-based system [15] where data are collected through the hospital-based fracture liaison services (FLS). This service is clinically supported by the Egyptian Academy of Bone Health and Metabolic Bone Diseases. The electronic system is the standard against which the fracture liaison service is benchmarked.
National cost of hip fracture
Based on the incidence of osteoporotic hip fractures in Egypt [16], the national direct cost of hip fractures has been calculated. The annual number of acute hospital bed days was obtained by multiplying the mean length of stay by the total number of hip fracture cases in a given year. The price for each specific procedure was multiplied by the number of episodes recorded.
The average exchange rate in 2023 (US $1 = 30.9 Egyptian pounds) was used to convert all costs to US dollars.
Patient population
To be able to assess the details of the hip fracture costs, data were analyzed from 3 centers from March 2022 to March 2023. The extracted data were anonymized before being used for analysis. The number of calendar days from admission to discharge from the hospital was used to calculate the length of stay. The 2023 January Price List was applied to calculate direct hospital costs.
Eligibility criteria
The study encompassed men and postmenopausal women with an inpatient hospital stay or outpatient attendance at the fracture clinic with a primary diagnosis of fragility fracture, defined as a closed low-impact fracture without trauma codes of the hip, neck of the femur, or pelvis. Fractures with a trauma code were not included in the study. The index date has been defined as the date of fragility fracture diagnosis in an outpatient setting or discharge from an inpatient setting. Only data on patients with osteoporotic hip fractures were collected for this study.
Data collection and data entry
The data was collected from each center through a secure portal. The system was the primary source of demographic, clinical, and administrative data on all cases of fragility fractures and deaths from the various fracture liaison centers across the country. All the 3 FLS centers voluntarily submitted data on patients that had been discharged following hip as well as major osteoporotic fractures. Data were entered prospectively in each center by a coordinator under supervision from the local FLS clinical lead. The data collected were collected for each fracture episode and based on a questionnaire collecting data on:
-
History of a fragility fracture after the age of 50 apart from the current hip fracture.
-
Menstrual history for women only.
-
Assessment of the 10-year probability of hip and major osteoporotic fractures using the fracture risk assessment (FRAX) assessment tool without BMD prior to the index date [17].
-
Assessment of fall risk using the falling risk assessment (FRAS) questionnaire [18].
-
A short questionnaire to assess for reasons and different mechanisms of falling.
-
Medical history including osteoporosis medications, other medications that may affect bone health and chronic medical conditions.
-
Functional disability using the Arabic HAQ questionnaire [19].
-
Type of surgery and clinical outcomes.
Data quality and data validation
Data validation reports were shared with each center along with monthly reports. The data analysis team verified the data with the contributing FLS center. Through regular two-way feedback and monthly meetings with the local coordinators, the data quality was kept under review. An annual report was created after the data had been verified.
Activity‑based funding
There are different levels of management of fractures in Egypt. Public hospitals in Egypt provide either free service supported by public funds or economy service paid for by the individual patient. The third level of management is the privately funded management. The price included in this work was based on the surgical intervention only. Other costs of emergency department activity, medical management, rehabilitation, or investigations were calculated but have not been included in the direct cost. Activity-based funding was calculated taking into account the length of hospital admission.
Ethical approval
This study is in agreement with the ethical guidelines of the Declaration of Helsinki and was approved by the institution’s ethics board of Tanta Faculty of Medicine. Ethical approval number 33997/8/20. Informed consent was obtained from all patients in accordance with the local ethical committee. Privacy of all patients’ data was granted as there was a code number for every patient file that included all investigations.
Statistical analysis
The collected data were tabulated and analyzed using an SPSS computer program. Comparing risk factors was carried out using the chi-square test for associations. The P value was set at 0.05.
Results
Incidence of hip fracture
The estimated annual incidence of low-impact hip fractures in individuals aged 50 years or more in Egypt 2022–2023 was 123.34 per 100,000 in women and 55.19 per 100,000 in men. Based on the total population of Egypt as of 2022, a total number of Egyptian women above the age of 50 years old is 12.5 million whereas the number of Egyptian men above 50 years old is 13.63 million. This equates to 15,417 postmenopausal women and 7522.4 men who had sustained osteoporotic hip fractures.
Population assessed
Basic characteristics
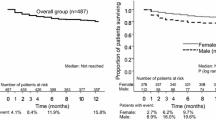
Table 1 shows the demographics and risk factors of the 412 Egyptian population sample included in this work. Table 2 shows the incidence of hip fractures among older adult Egyptians stratified to their age groups. The standardized hip fracture rate was significantly higher in post-menopausal women compared to men. 4.5% of the patients passed away with a mean duration of 2.3 + 0.4 months after surgery.
Surgical management
Time to surgery was 2.2 + 0.5 days. The mean length of stay for hip fractures surgery was 5.2 days. Cemented hemi-arthroplasty was the most common surgical repair (39%) followed by cemented total hip replacement surgery (31%) and internal fixation with short Intramedullary nail/dynamic hip screw (30%). Spinal anesthesia remains the most common type of anesthesia, either alone (52%), or in combination with a nerve block (20%).
Length of stay
There was considerable variation amongst the patients in terms of length of acute hospital stay following hip fracture. This has been attributed to different patient demographics, associated comorbidities, or other medical abnormalities. In general, hip surgery was carried out within 48 h and the average hospital stay was 5.2 + 2.6 days.
Bed days
Hip fractures place a significant strain on the acute hospital sector. The average length of stay for hip fracture was 5.2 + 2.6 days, excluding any other periods of hospital admission to treat the medical condition(s). This accounts for 114,697 bed days (5 × the number of patients with hip fractures).
Direct costs of hip fracture
The direct hospital costs of hip fracture care have been calculated using the 2023 Price List, which outlines charges incurred for inpatient surgical intervention. Table 2 shows the percentage of the different types of hip surgery, whereas Table 3 shows the mean total direct nonsurgical healthcare costs in the first year after osteoporotic hip fracture. Per patient, the total direct cost of hip fracture is calculated based on the type of the fracture and the surgical approach of management: 39% of the patients had hemi-arthroplasty with an estimated direct cost of the fractured hip of 671,025,000 Egyptian pounds (US $21,716,019.4). On the other hand, 31% had total hip replacement cemented with an estimated direct cost of the fractured hip of 782,210,000 Egyptian pounds (US $25,314,239.4), whereas 30% had internal fixation—dynamic hip screw with estimated direct cost of 516,150,000 Egyptian pounds (US $16,703,883). This is based on the estimated hospital stay of 5 days which includes in total 114,700 days of admission. This equates to a total cost of 1,969,385,000 Egyptian pounds (US $63,734,142.4).
BMD assessment
BMD and fracture risk assessment
BMD was measured in 141 patients, and DXA scans revealed that 120 (85.1%) patients were osteoporotic. The mean FRAX 10-year probability of major osteoporosis fracture was 18.37 ± 10.1 with 55.1% at high risk and 40.4% at moderate risk. The mean 10-year probability of hip fracture was 8.08 ± 7.1 with 74.9% at high risk and 22.1% at moderate risk.
Falls risk
All patients were evaluated for their risk of falling. The high fracture risk group had a higher risk of falling. Falling was more common indoors (75%) than outdoors (25%). The main cause of indoor falling was ablution (25%), indoor slipping (19%), indoor falling (16%), indoor stumbling (15%), and outdoor stumbling (13%), whereas outdoor falling occurred in 12%.
In postmenopausal women, there was also a significant relationship (p < 0.05) between functional disability and fracture risk.
Discussion
Osteoporosis and subsequent fragility fractures not only have a significant impact on the patients’ general health and quality of life but also impose a major economic burden on the healthcare system. The economic costs of a disease can be used to estimate the burden of that disease. Such economic costs can be divided into two sections, including direct and indirect costs. Direct costs are expenses for the use of resources incurred for disease prevention, diagnosis, and management, while indirect or productivity costs represent the value of labor earnings lost because of disease-related disability [20]. The purpose of this study was to determine the annual direct cost of hip fractures in Egypt in terms of both bed days and direct surgical costs.
Results of this work revealed that the average direct cost of surgical management in Egypt was in the range of 75,000–110,000 Egyptian pounds (US $2427.2–3559.9) per episode of care. These figures are in concordance with the costs of hip fractures reported globally. In the Republic of Ireland [21], from 2014 to 2020, the Irish health service spent approximately €296 million on hip fracture hospitalization, which is equivalent to roughly €11,700 per episode of care. The hospitalization expenses related to index admission for primary hip fracture in the UK [22] were £8663, while the cost of direct hospitalization for hip fractures in Italy increased from €343 to €457 million from 2000 to 2014 [23]. Williamson et al. [24] conducted a systematic review and meta-analysis of over 100 studies to assess the global cost of fragility fractures, and the results revealed an average cost of $10,075 for the index hospital admission.
Annual costs of hip fractures are useful as it provides greater clinical implication for health policy decision-making. The 1-year direct cost of hip fracture among women and men in Egypt amounted to 1,969,385,000 Egyptian pounds (US $63,734,142.4). This cost was calculated based on average economic prices and did not include private sector cost which covers about 16% of the medical service in Egypt. This would incur further expenses. Though it is difficult to generalize costing analyses between different countries because of variations in the actual costs, treatment patterns, and health-care systems, the results of this work are comparable to other countries. In the European Union, the cost of osteoporosis-associated fractures has been estimated to be 37 billion euros [25]. In the USA, the direct medical cost of osteoporosis was estimated to be 13.7 to 20.3 billion dollars. Additionally, it is anticipated that by 2025, there will be more than 3 million osteoporotic fracture cases annually, with a corresponding cost of $25.3 billion [26, 27].
Almost all patients with hip fractures are hospitalized. Their length of stay in the hospital is relatively long, and most of the cases, if not all, home care is required after discharge from the hospital [28]. Notably, the costs recorded in this study reflect the estimated direct costs of hip fractures in Egypt. This might be undervalued if contrasted to the direct cost in other countries. This might be attributed to the fact that no additional costs, such as the cost of medical therapies and medical care (which was included in the estimates of other countries) [29] as well as rehab, have been included in this work calculations. However, the figures recorded in this work remain valid as they represent the direct hip fracture costs which form the main bulk of the expenses.
Despite the high prevalence of prior history of low trauma fracture particularly in the past 2 years (imminent fracture risk) reported in this study, which was also supported by the high prevalence of the 10-year probability of hip fracture risk, none of the patients was on any form of osteoporosis therapy. This could explain the significant treatment gap in osteoporosis management in Egypt [5] and in the meantime represent the missed opportunity for osteoporosis therapy. The result of this work raises red flags to the policy makers in Egypt that such fragility fractures are preventable, should appropriate approaches such as fracture liaison service be implemented as a standard in Egypt. Health economics studies in the secondary prevention of fragility fractures in Egypt [30] documented the cost-effectiveness of fracture liaison services compared to standard fracture care.
Demographics of this work revealed that the incidence of hip fractures was higher in women in comparison to men (incidence in postmenopausal women was 123.34/100,000, whereas in men, it was 55.19/100,000). Most of the fractured patients were older than 60 years old. These data agree with that reported from other countries [31, 32] documenting the higher incidence of hip fractures in women in the same age group. These data also highlight the importance of having a national register that facilitates tracking patients with imminent fracture risk or those at high risk of sustaining a fracture.
Falls and fractures in older people are often preventable. Falling is a cause of distress, pain, injury, loss of confidence, loss of independence, and mortality. Therefore, reducing falls and fractures is important for maintaining the health, wellbeing, and independence of older people [33]. This study highlighted the importance of patient education to reduce the likelihood of falling. Falling during ablution was the most common indoor cause of hip fracture followed by cardiovascular causes. Hence, approaches to prevent falling (and accordingly prevent hip fractures) or at least decrease the incidence of falling should be a top priority. Unfortunately, there is no such dedicated service to falling in Egypt. A national program for fall prevention should be urgently considered in Egypt in a trial to improve the quality of life of older adults Egyptians, minimize the likelihood to sustain a fragility fracture and consequently reduce healthcare spending.
Limitation of the study
Though 412 hip fractures were included in this work, and only 141 of those patients had BMD assessment. This could be attributed to the nature of the hip fracture and the difficulty to transport the patients. Recording of the BMD is important for monitoring the patient’s response to management. Also, the hip fracture cost included in this work was based on the economic tariff, and the national bill of the hip fracture cost is expected to go higher if the private sector expenses have been included.
In conclusion, hip fractures have a significant clinical and financial impact on patients and the healthcare system, with acute hospitalization contributing to a significant amount of the costs incurred. A timely operation can shorten the hospital stay and lower the cost of admission. The incidence and prevalence of osteoporosis and related fractures are rising as a result of longer life expectancies and an aging population, which will drive up costs in the future. The most economically advantageous surgical intervention approach may be chosen with the aid of a preoperative assessment of bone health status.
Availability of data and materials
The data will be available upon reasonable request.
Abbreviations
- BMD:
-
Bone mineral density
- DALYs:
-
Disability adjusted life years
- DXA:
-
Dual energy X-ray absorptiometry
- FLS:
-
Fracture liaison service
- FRAS:
-
Falling risk assessment score
- FRAX:
-
Fracture risk assessment
- HAQ:
-
Health Assessment Questionnaire
References
Cooper C (1997) Advances in the epidemiology, prevention, and treatment of osteoporosis and fracturesthe crippling consequences of fractures and their impact on quality of life. Am J Med 103(2):S12–S19
Johnell O, Kanis JA (2006) An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos Int 17(12):1726–1733
Leal J, Gray AM, Prieto-Alhambra D, Arden NK, Cooper C, Javaid MK, Judge A (2016) Impact of hip fracture on hospital care costs: a population-based study. Osteoporos Int 27(2):549–558
Johansson H, Siggeirsdottir K, Harvey NC, Oden A, Gudnason V, McCloskey E et al (2017) Imminent risk of fracture after fracture. Osteoporos Int 28(3):775–780
El Miedany Y, El Gaafary M, Gadallah N, Mahran S, Fathi N, Abu Zaid MH, Tabra SAH, Hassan W, Elwakil W (2023) Osteoporosis treatment gap in patients at risk of fracture in Egypt: a multi-center, cross-sectional observational study. Arch Osteoporos 18(1):58. https://doi.org/10.1007/s11657-023-01252-8
Kanis JA, Svedbom A, Harvey N et al (2014) (2014) The osteoporosis treatment gap. J Bone Miner Res 29:1926–1928
Keen RW (2014) Pathophysiology of osteoporosis. In: Clunie GPR, Keen RW (eds) Osteoporosis, 2nd edn. Oxford University Press, Oxford
Borgström F, Johnell O, Kanis JA, Jönsson B, Rehnberg C (2006) At what hip fracture risk is it cost-effective to treat? Osteoporos Int 17(10):1459–1471
El-Tawab SS, Saba EKA, Elweshahi HMT, Ashry MH (2016) Knowledge of osteoporosis among women in Alexandria (Egypt): a community based survey. Egypt Rheumatol 8(3):225–231
El Miedany Y, Gadallah NA, Toth M (2022) Optimizing osteoporosis management: targeting to treat — an initiative by the Egyptian Academy of Bone Health. Egypt Rheumatol Rehabil 49:61. https://doi.org/10.1186/s43166-022-00161-x
Häussler B, Gothe H, Göl D, Glaeske G, Pientka L, Felsenberg D (2007) Epidemiology, treatment and costs of osteoporosis in Germany—the Bone EVA Study. Osteoporosis Int 18(1):77–84
Lim SS, Vos T, Flaxman AD, et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 2012; 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 380(9859):2224-2260. https://doi.org/10.1016/S0140-6736(12)61766-8
Chia PH, Gualano L, Seevanayagam S, Weinberg L (2013) Outcomes following fractured neck of femur in an Australian metropolitan teaching hospital. Bone Joint Res 2(8):162–168. https://doi.org/10.1302/2046-3758.28.2000177
Panula J, Pihlajamäki H, Mattila VM, Jaatinen P, Vahlberg T, Aarnio P, Kivelä S-L (2011) Mortality and cause of death in hip fracture patients aged 65 or older - a population-based study. BMC Musculoskelet Disord 12(1):105
Gadallah N, El Miedany Y (2022) Operative secondary prevention of fragility fractures: national clinical standards for fracture liaison service in Egypt—an initiative by the Egyptian Academy of Bone Health. Egypt Rheumatol Rehabil 49:11
El Miedany Y, El Gaafary M, Gadallah N, Mahran S, Fathi N, Abu Zaid MH et al (2023) Incidence and geographic characteristics of the population with osteoporotic hip fracture in Egypt— by the Egyptian Academy of Bone Health. Arch Osteoporos 18:115. https://doi.org/10.1007/s11657-023-01325-8
Kanis JA, Johnell O, Oden A et al (2008) FRAX and the assessment of fracture probability in men and women from the UK. Osteoporos Int 19(4):385–397
El Miedany Y, El Gaafary M, Toth M, Palmer D, Ahmed I (2011) Falls risk assessment score (FRAS): time to rethink. J Clin Gerontol Geriatr 2(1):21–26
El Miedany Y, El Gaafary M, Youssef SS, Palmer D (2010) Incorporating patient reported outcome measures in clinical practice: development and validation of a questionnaire for inflammatory arthritis. Clin Exp Rheumatol 28(5):734–744
Panopalis P, Yazdany J, Gillis JZ, Julian L, Trupin L, Hersh AO, Criswell LA, Katz P, Yelin E (2008) Health care costs and costs associated with changes in work productivity among persons with systemic lupus erythematosus. Arthritis Rheum 59(12):1788–1795. https://doi.org/10.1002/art.24063
Ferris H, Brent L, Sorensen J (2022) Cost of hospitalisation for hip fracture-findings from the Irish hip fracture database. Osteoporos Int 33(5):1057–1065. https://doi.org/10.1007/s00198-021-06294-7
Judge A, Javid MK, Leal J, UK study 14 et al (2016) Models of care for the delivery of secondary fracture prevention after hip fracture: a health service cost, clinical outcomes and cost effectiveness study within a region of England. NIHR Journals Library, Southampton (UK)
Piscitelli P, Neglia C, Feola M, Rizzo E, Argentiero A, Ascolese M et al (2020) Updated incidence and costs of hip fractures in elderly Italian population. Aging Clin Exp Res 32(12):2587–2593
Williamson S, Landeiro F, McConnell T et al (2017) Costs of fragility fractures globally: a systematic review and meta-regression analysis. Osteoporosis Int 28(10):2791–2800
Zamani B, Ebadi S, Ahmadvand A, Mousavi G (2010) The Frequency of Osteoporosis in hip fracture following minor trauma and the resulting mortality rate and direct treatment costs in patients over 45 years old in Kashan Naghavi Hospital during 2005–2007. J Kerman Univ Med Sci 17(2):137–144
Burge R, Dawson-Hughes B, Solomon DH, Wong JB, King A, Tosteson A (2007) Incidence and economic burden of osteoporosis-related fractures in the United States, 2005–2025. J Bone Miner Res 22(3):465–475
Rashki Kemmak A, Rezapour A, Jahangiri R, Nikjoo S, Farabi H, Soleimanpour S (2020) Economic burden of osteoporosis in the world: a systematic review. Med J Islam Repub Iran 34:154. https://doi.org/10.34171/mjiri.34.154
Dyer SM, Crotty M, Fairhall N, Magaziner J, Beaupre LA, Cameron ID et al (2016) A critical review of the long-term disability outcomes following hip fracture. BMC Geriatr 16(1):158
Nazrun AS, Tzar MN, Mokhtar SA, Mohamed IN (2014) A systematic review of the outcomes of osteoporotic fracture patients after hospital discharge: morbidity, subsequent fractures, and mortality. Ther Clin Risk Manage 10:937
Y. El Miedany, M. El Gaafary, S. Mahran, W. Hassan, N. Gadallah, M. H. Abu-Zaid, W. Elwakil. Health economics in secondary prevention of fragility fractures: cost effectiveness of fracture liaison services compared to standard fracture care in Egypt: An initiative by the Egyptian Academy of Bone Health. ESCEO conference 2023; P306: 262 https://www.wco-iof-esceo.org/sites/wco_23/pdf/WCO23-AbstractBook.pdf
Melton LJ 3rd (2000) Who has osteoporosis? A conflict between clinical and public health perspectives. J Bone Miner Res 15:2309–2314
Stephens AS, Toson B, Close JCT (2014) Current and future burden of incident hip fractures in new South Wales. Australia Arch Osteoporos 9:200
Falls: applying All Our Health. Guidance. 2022. https://www.gov.uk/government/publications/falls-applying-all-our-health/falls-applying-all-our-health [Accessed on 14th Jul 2023]
Duplicate publication
This is to confirm that the content of the manuscript has not been published or submitted for publication elsewhere.
Funding
The costs of DXA scanning and lab testing as well as the admin staff in charge of the electronic data recording were covered by Amgen Egypt. No funding was received by any one of the authors.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study methodology, analysis, and interpretation of the data and outcomes as well as the manuscript writing, reading, and approval of the final version.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study is in agreement with the ethical guidelines of the Declaration of Helsinki, and it follows the ethical standards of Tanta Faculty of Medicine, with the institution’s ethics board approval number 33997/8/20. Informed written consent from all patients was obtained in accordance with the local ethical committee. Privacy of all patients’ data was granted as there was a code number for every patient file that included all investigations.
Consent for publication
Not applicable.
Competing interests
The authors declare that Mohammed H Abu-Zaid is an associate editor in the Egyptian Rheumatology and Rehabilitation. Waleed Hassan, Safaa Mahran, Naglaa GadAllah, and Yasser El Miedany are from the editorial board of the journal.
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
El Miedany, Y., El Gaafary, M., Gadallah, N. et al. Health economics: direct cost of osteoporotic hip fracture in Egypt—an analysis for the Egyptian healthcare system by the Egyptian Academy of Bone Health. Egypt Rheumatol Rehabil 50, 50 (2023). https://doi.org/10.1186/s43166-023-00218-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43166-023-00218-5